

The Clinical Effect of Compound Multi-point Optical Defocusing Lens on Myopia Progression in Children
-
摘要:
目的 观察儿童配戴复合多点光学离焦镜片对延缓近视效果。 方法 选取2022年11月至2023年3月于云南大学附属医院儿童眼科就诊近视患者,其中单焦点镜片配戴者52例为对照组,复合多点光学离焦镜片配戴者78例作为实验组。比较2组在戴镜前及戴镜后的第3、6、9、12个月,期间主要观察等效球镜度、眼轴长度的变化,对不同组间近视控制效果进行比较。 结果 2组戴镜前后等效球镜度均有不同程度的变化,对照组和实验组治疗效果差异有统计学意义(F = 13.80,P < 0.001)。自佩戴6个月起,对照组屈光度显著低于实验组(P < 0.05),且佩戴时间越长,2组之间的效果差距越大。2组戴镜前后眼轴长度也均有不同程度的变化,但对照组和实验组治疗效果差异无统计学意义(F = 0.028,P = 0.876),提示2种镜片对眼轴的影响差异无统计学意义。 结论 与单焦点镜片相比,复合多点光学离焦镜片能有效延缓儿童近视进展。 Abstract:Objective To observe the effect of the delay of myopia in children wearing composite multi-point optical defocusing lens. Methods A total of 52 cases (n = 104) of monocal lens wearers were selected as the control group, and 78 cases (n = 156) of compound multi-point optical distrocal lens wearers were selected as the experimental group. The effect of myopic control between two groups was compared before and after wearing glasses at 3, 6, 9 and 12 months, during which the changes of equivalent spherical lens and eye axis length were mainly observed. Results The equivalent spherical degree of the two groups before and after wearing glasses had different degrees of change and the treatment effect between the control group and the experimental group was statistically significant (F = 13.80, P < 0.001). After 6 months of wearing glasses, the diopter of the control group was significantly lower than that of the experimental group, and the longer the wearing time, the greater the difference between the two groups. The axial length of the eyes of the two groups also changed to different degrees before and after wearing glasses, but there was no statistical significance in the treatment effect between the control group and the experimental group (F = 0.028, P = 0.876), suggesting that there was no statistical significance in the influence of the two lenses on the axial of the eyes. Conclusion Compared with the single-focus lenses, composite multi-point optical defocus lenses can effectively delay the progression of myopia in children. -
Key words:
- Myopia /
- Peripheral defocusing /
- Axis oculi /
- Composite multi-point optical defocusing
-
冠状动脉血管平滑肌细胞增殖(coronary artery smooth muscle cell,CASMC)是动脉粥样硬化和血管损伤后再狭窄的关键事件[1],因此研究平滑肌增殖对冠心病的治疗有重要作用。钙库操纵型钙通道(store-operated calcium channel,SOCC)目前被认为在CASMC增殖方面起着重要作用[2]。SOCC由3个重要组成分子组成:瞬时受体电位阳离子通道,基质相互作用分子和Orai家族[3]。Orai在人体中有Orai1、Orai2、Orai3 3种结构高度相似同源物[4],有文献表明[5]Orai3在调节细胞生存和死亡通路中的起着关键作用。Orai3过表达与多支癌症特征相关,包括细胞增殖、迁移和凋亡等[6]。目前多项研究表明Orai1参与血管平滑肌细胞增殖与血管内膜形成,但Orai3与血管平滑肌细胞增殖的关系研究较少,因此本研究旨在探讨Orai3分子与CASMC增殖的关系,为冠心病治疗提供一定理论基础。
1. 材料与方法
1.1 主要试剂
大鼠原代冠状动脉平滑肌细胞(普诺赛公司);DMEM/F12(1∶1)培养液和胎牛血清(BI公司); 0.25%胰蛋白酶-EDTA消化液(Gibco公司);Lipofectamine 3000(美国Thermo Fisher公司);Opti-MEM培养液(Gibco公司);Cell Counting Kit 8(MCE公司);逆转录试剂盒FastQuant RT Kit和qPCR试剂盒Supernal premix plus(北京天根公司);Orai3兔抗大鼠抗体(SAB公司);β-Actin小鼠抗大鼠抗体(Affinity公司)。
1.2 细胞培养
大鼠冠状动脉血管平滑肌细胞采用10%胎牛血清的DMEM培养液培养,取5~8代用于实验,血清饥饿采用无血清的DMEM培养液培养48 h。
1.3 Orai3的干扰及过表达质粒
Orai3干扰采用小干扰RNA序列:5′-GCUGGAGAGCGAUCAUGAATT-3′;5′-UUCAUGAUCGCUCUCCAGCTT-3′(和元生物有限公司)转染。合成过表达质粒:PcDNA3.1(+)-Orai3-3×FLAG-p2A-EGF(和元生物有限公司)用于实验。转染小干扰RNA和过表达质粒72 h后大鼠冠状动脉血管平滑肌细胞进行后续实验。
1.4 QPCR实验
用Trizol法提取总RNA,逆转录成cDNA,得到的cDNA扩增作sybr green 荧光QPCR实验。β-Actin:上游引物5′-TGCTATGTTGCCCTAGACTTCG-3′;下游引物5′-GTTGGCATAGAGGTCTTTACGG-3′(武汉塞维尔)。Orai3:上游引物5′-CACTTCTGCTCTGCTGTCGG-3′;下游引物5′-TCAATATGGGGCAGCAGACA-3′(武汉塞维尔)。选择反应条件:预变性:95 ℃ 15 min;PCR:(95 ℃ 10 s+60 ℃ 30 s)×40循环。
1.5 Western Blot实验
10%的SDS-PAGE用于电泳分离蛋白;200 mA,1 h转膜;用0.5% Tween20的TBST溶液配制5%脱脂牛奶封闭PVDF膜,一抗β-actin (1∶5000),Orai3(3∶1000)配置后4 ℃过夜孵育后0.5% Tween20的TBST洗膜,二抗常温摇床孵育1 h,ECL显影液显影。
1.6 细胞计数和CCK8检测细胞增殖
血清饥饿0~96 h作生长曲线;转染后细胞接种24~96 h作生长曲线。
1.7 统计学处理
数据分析使用SPSS17.0统计学软件,计量资料用均数±标准差(
$\bar x \pm s $ )表示,组间比较采用t检验,P < 0.05表示差异具有统计学意义。2. 结果
2.1 CASMC增殖时Orai3表达量变化情况
分别用CCK8实验和细胞计数实验检测无血清培养和10%血清培养时CASMC增殖情况。CCK8实验:培养48 h后无血清组与10%血清组之间CASMC细胞增殖,差异有统计学意义(P < 0.01),见表1。细胞计数实验(1×104个):培养24 h后无血清组与10%血清组之间CASMC细胞增殖,差异有统计学意义(P < 0.01),见表2。2组实验表明培养24 h~48 h后无血清组较10%血清组CASMC增殖速率下降(P < 0.01),即无血清培养抑制CASMC细胞增殖,见图1。
表 1 CCK8检测CASMC增殖[($\bar x \pm s $ ),n = 5]Table 1. Growth curve of CASMC cells by CCK8 assay [($\bar x \pm s $ ),n = 5]时间(h) FBS+ FBS− t P 0 0.0634 ± 0.0291 0.0804 ± 0.0310 0.8947 0.3971 24 0.3662 ± 0.1092 0.2629 ± 0.0645 1.8200 0.1062 48 1.0450 ± 0.0942 0.4709 ± 0.0642 11.2700 < 0.0001** 72 1.6350 ± 0.1015 0.5659 ± 0.0946 17.2300 < 0.0001** 96 1.9710 ± 0.1611 0.5015 ± 0.0905 17.7800 < 0.0001** FBS+为10%血清的完全培养液培养,FBS-为无血清的不完全培养基培养。与FBS+组比较,**P < 0.01。 表 2 CASMC细胞计数(1×104)[($\bar x \pm s $ ),n = 5]Table 2. Growth curve of CASMC cells by cell counting assay (1×104)[($\bar x \pm s $ ),n = 5]时间(h) FBS+ FBS− t P 0 1.3400 ± 0.3209 1.6000 ± 0.4183 1.1030 0.3022 24 4.9000 ± 0.7416 3.3500 ± 0.4183 4.0700 0.0036** 48 11.7000 ± 0.9747 4.4500 ± 0.9083 12.1700 < 0.0001** 72 13.5500 ± 1.0950 4.7000 ± 0.8909 14.0100 < 0.0001** 96 14.3500 ± 0.9618 3.5500 ± 1.0370 17.0800 < 0.0001 ** FBS+为10%血清的完全培养液培养,FBS-为无血清的不完全培养基培养。 与FBS+比较,**P < 0.01。  图 1 无血清组及10%血清组CASMC细胞增殖情况A:CCK8实验分别检测无血清组(FBS-)和10%血清组(FBS+)培养下CASMC增殖情况;B:细胞计数实验分别检测无血清组(FBS-)和10%血清组(FBS+)培养下CASMC细胞增殖情况。与FBS+比较,**P < 0.01。Figure 1. The coronary vessel smooth muscle cell proliferation difference between 0%FBS medium cultured group and 10% FBS medium cultured group
图 1 无血清组及10%血清组CASMC细胞增殖情况A:CCK8实验分别检测无血清组(FBS-)和10%血清组(FBS+)培养下CASMC增殖情况;B:细胞计数实验分别检测无血清组(FBS-)和10%血清组(FBS+)培养下CASMC细胞增殖情况。与FBS+比较,**P < 0.01。Figure 1. The coronary vessel smooth muscle cell proliferation difference between 0%FBS medium cultured group and 10% FBS medium cultured group分别用Western Blot实验和QPCR实验检测血清饥饿48 h后Orai3表达量情况,无血清组与10%血清组相比相对蛋白表达量下降,P < 0.01;无血清组与10%血清组相比RNA蛋白表达量下降,P < 0.05,见表3,图2。结果表明无血清组较10%血清组CASMC中Orai3表达量下降,结合前期无血清抑制CASMC细胞增殖,表明抑制细胞增殖Orai3表达量下降(P < 0.01)。
表 3 CASMC的Orai3相对表达量[($\bar x \pm s $ ),n = 3]Table 3. Orai3 expression of CASMC cells [($\bar x \pm s $ ),n = 3]Orai3 FBS+ FBS- t P 蛋白表达量 1.0270 ± 0.2925 0.2036 ± 0.1434 7.0090 0.0060** RNA表达量 1.0150 ± 0.2065 0.1498 ± 0.0167 7.5450 0.0171* FBS+为10%血清的完全培养液培养,FBS-为无血清的不完全培养基培养。与FBS+比较,*P < 0.05,**P < 0.01。 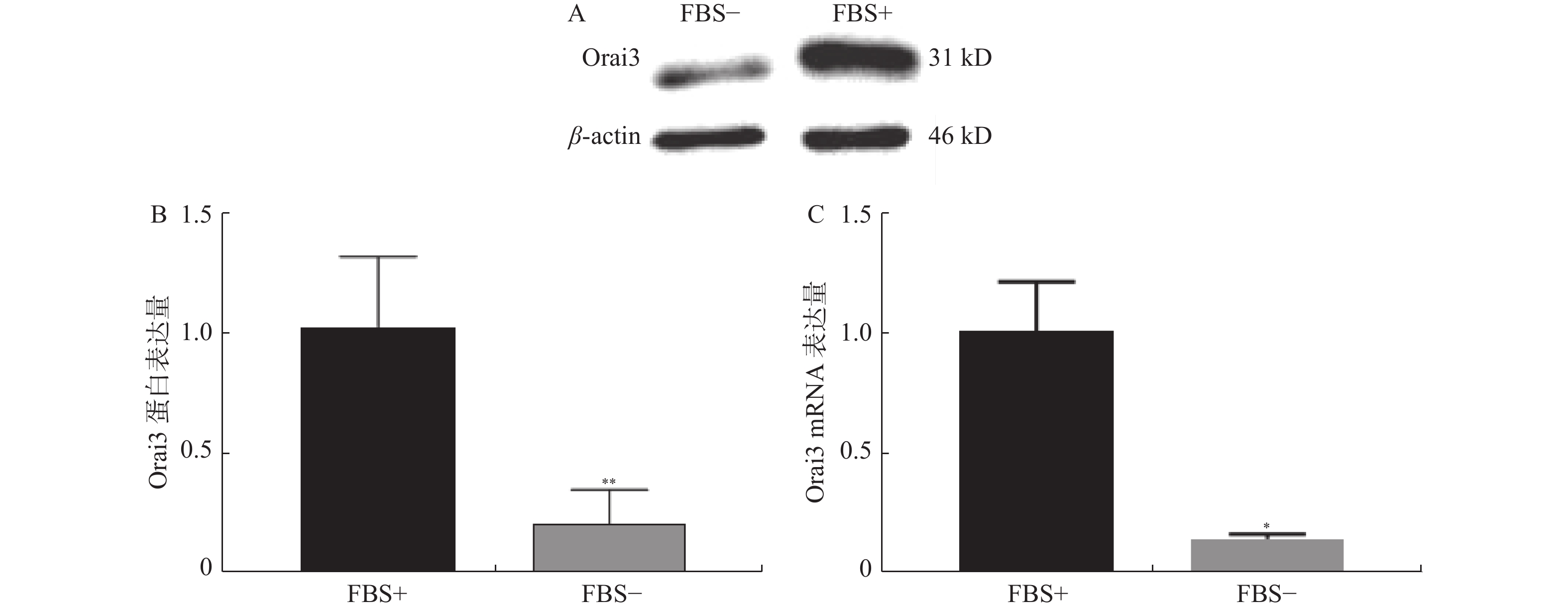 图 2 无血清组及10%血清组Orai3表达量情况A:血清组(FBS-)和10%血清组(FBS+)培养下CASMC细胞提取蛋白Western Blot检测Orai3表达量条带图;B:Western Blot实验分别检测无血清组(FBS-)和10%血清组(FBS+)培养下CASMC增殖情况;C:QPCR实验分别检测无血清组(FBS-)和10%血清组(FBS+)培养下CASMC细胞增殖情况。与FBS+比较,*P < 0.05,**P < 0.01。Figure 2. Orai3 expression difference between 0%FBS medium cultured group and 10% FBS medium cultured group
图 2 无血清组及10%血清组Orai3表达量情况A:血清组(FBS-)和10%血清组(FBS+)培养下CASMC细胞提取蛋白Western Blot检测Orai3表达量条带图;B:Western Blot实验分别检测无血清组(FBS-)和10%血清组(FBS+)培养下CASMC增殖情况;C:QPCR实验分别检测无血清组(FBS-)和10%血清组(FBS+)培养下CASMC细胞增殖情况。与FBS+比较,*P < 0.05,**P < 0.01。Figure 2. Orai3 expression difference between 0%FBS medium cultured group and 10% FBS medium cultured group2.2 干扰Orai3后CASMC增殖情况
干扰Orai3后72 h提取RNA和蛋白质作干扰效率检测:干扰效率WB检测和QPCR检测,WB检测Orai3相对蛋白表达量:干扰组(siOrai3)为(0.3089±0.0219),阴性对照组(siOrai3-NC)为(0.9661±0.1018)。 QPCR检测Orai3相对RNA表达量:干扰组(siOrai3)为(0.2129±0.0761),阴性对照组(siOrai3-NC)为(1.0140±0.2028)。结果表明干扰后Orai3表达下降70%以上。
干扰后CCK8实验和细胞计数实验检测CASMC增殖情况,CCK8实验:干扰后培养48 h后siOrai3与siOrai3-NC相比,增殖差异有统计学意义(P < 0.01),见表4。细胞计数实验(1×104个):干扰后培养48 h后siOrai3与siOrai3-NC相比增殖差异有统计学意义(P < 0.01),见表5。结果表明与对照组相比干扰Orai3后抑制CASMC增殖,在48 h后开始出现差异(P < 0.01),见图3。
表 4 CCK8检测siOrai3干扰后CASMC增殖情况[($\bar x \pm s $ ),n = 5]Table 4. Growth curve of siOrai3 CASMC cells by CCK8 assay[ ($\bar x \pm s $ ),n = 5]时间(h) siOrai3-NC siOrai3 t P 24 0.0801 ± 0.0288 0.0985 ± 0.0418 0.8098 0.4415 48 0.4464 ± 0.0603 0.1966 ± 0.0130 9.0590 < 0.0001** 72 0.8322 ± 0.1142 0.6127 ± 0.0842 3.4590 0.0086** 96 1.4200 ± 0.0547 0.6499 ± 0.1201 13.0400 0.0034** siOrai3-NC为转染siOrai3阴性对照组,siOrai3为转染siOrai3实验组。与siOrai3-NC比较,**P < 0.01。 表 5 siOrai3干扰后CASMC细胞计数(1×104)($\bar x \pm s $ ,n = 3)Table 5. Growth curve of siOrai3 CASMC cells by cell counting assay (1×104)($\bar x \pm s $ ,n = 3)时间(h) siOrai3-NC siOrai3 t P 24 2.0830 ± 1.0100 1.2500 ± 0.2500 1.3870 0.2378 48 8.1670 ± 1.2580 4.4170 ± 0.6292 4.6170 0.0099 ** 72 12.0000 ± 1.0000 7.0000 ± 0.5000 7.7460 0.0015** 96 14.0000 ± 1.0000 7.8330 ± 0.7638 8.4880 0.0011** siOrai3-NC为转染siOrai3阴性对照组,siOrai3为转染siOrai3实验组。与NC组比较,**为P < 0.01。 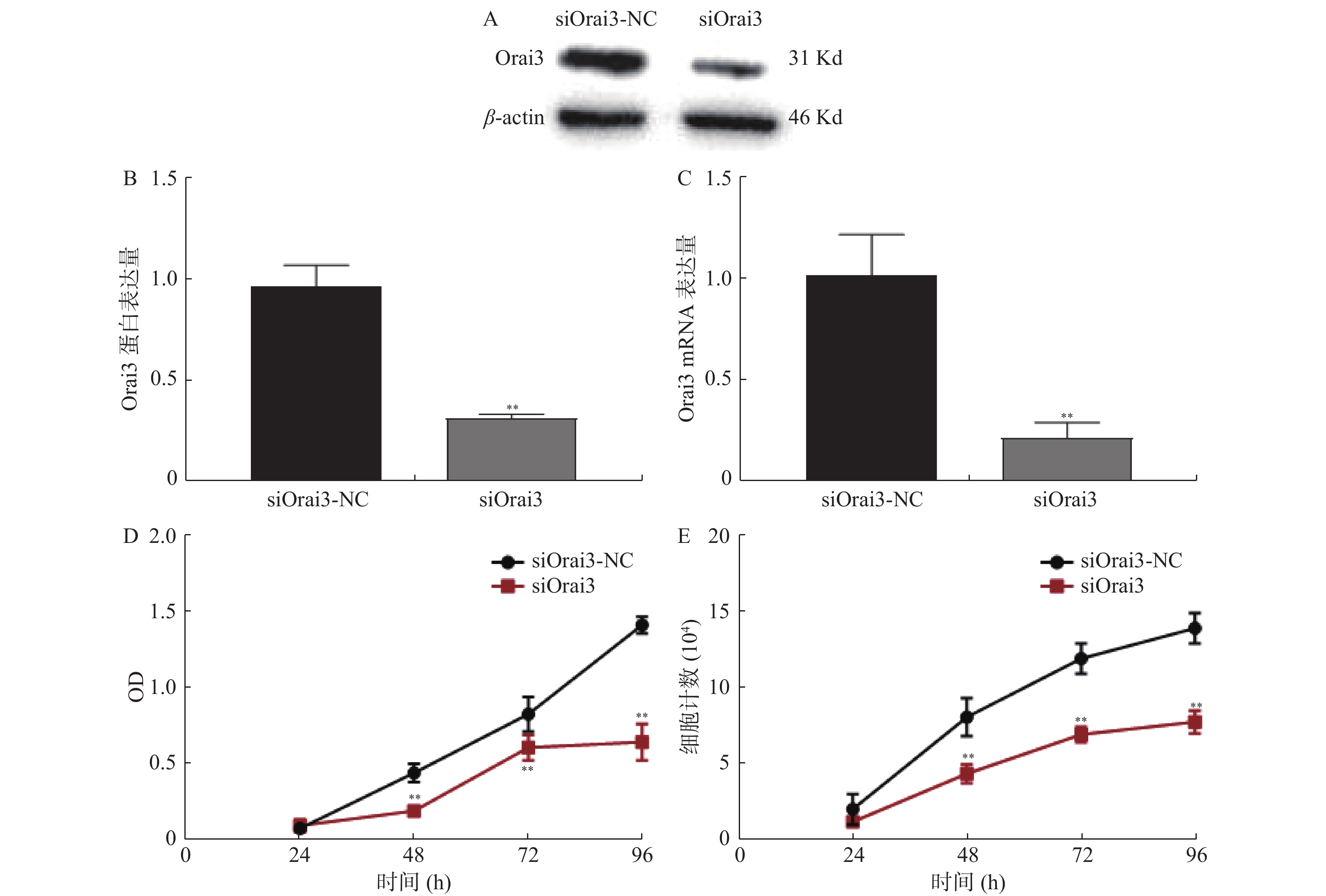 图 3 干扰Orai3后CASMC细胞增殖情况A :干扰Orai3后CASMC细胞提取蛋白Western Blot检测Orai3表达量条带图。B:干扰Orai3后Western Blot实验检测干扰效率;C:干扰Orai3后QPCR实验检测干扰效率;D:干扰Orai3后CCK8实验检测CASMC增殖情况;E:干扰Orai3后细胞计数实验检测CASMC增殖情况;siOrai3-NC:Orai3干扰阴性对照组;siOrai3:Orai3干扰组。与FBS+比较,**P < 0.01。Figure 3. Orai3 interfering and the Coronary vessel smooth muscle cell proliferation.
图 3 干扰Orai3后CASMC细胞增殖情况A :干扰Orai3后CASMC细胞提取蛋白Western Blot检测Orai3表达量条带图。B:干扰Orai3后Western Blot实验检测干扰效率;C:干扰Orai3后QPCR实验检测干扰效率;D:干扰Orai3后CCK8实验检测CASMC增殖情况;E:干扰Orai3后细胞计数实验检测CASMC增殖情况;siOrai3-NC:Orai3干扰阴性对照组;siOrai3:Orai3干扰组。与FBS+比较,**P < 0.01。Figure 3. Orai3 interfering and the Coronary vessel smooth muscle cell proliferation.2.3 过表达Orai3后CASMC增殖情况
过表达Orai3后72 h提取RNA和蛋白质作过表达效率检测:过表达效率WB检测和QPCR检测,WB检测Orai3相对蛋白表达量:过表达组(oeOrai3)为(1.3230±0.1124) ,阴性对照组(oe-NC)为(0.7448±0.1054)。 QPCR检测Orai3相对表达量:过表达组(oeOrai3)为 (4.4630±0.7038),阴性对照组(oe-NC)为(1.0070±0.1526)。结果显示过表达后细胞中Orai3表达量增加。
过表达后CASMC细胞增殖情况CCK8实验和细胞计数实验,CCK8实验:过表达后培养48 h后oe-Orai3与oe-NC相比,增殖差异有统计学意义(P < 0.01),见表6。细胞计数实验(1×104个):过表达后培养48 h后oe-Orai3与oe-NC相比,增殖差异有统计学意义(P < 0.01),见表7。结果表明与对照组相比,过表达Orai3后促进CASMC增殖,在48 h开始出现差异(P < 0.01),见图4。
表 6 CCK8检测oe-Orai3转染后CASMC增殖情况[($\bar x \pm s $ ),n = 5]Table 6. Growth curve of oe-Orai3 CASMC cells by CCK8 assay [($\bar x \pm s $ ),n = 5]时间(h) oe-NC oe-Orai3 t P 24 0.0621 ± 0.0143 0.0640 ± 0.0062 0.2802 0.7865 48 0.4469 ± 0.0564 1.1080 ± 0.0712 16.2700 < 0.0001** 72 0.8993 ± 0.0979 1.8710 ± 0.1437 12.4900 < 0.0001 ** 96 1.4570 ± 0.0842 2.0770 ± 0.0820 11.7800 < 0.0001** oe-NC为转染阴性对照组,Orai2、Orai3阴性对照组为同一空白载体;oe-Orai2为过表达Orai2质粒DNA组,oe-Orai3为过表达Orai3质粒DNA组。与NC组比较,**为P < 0.01。 表 7 oe-Orai3转染后CASMC细胞计数(1×104)[($\bar x \pm s $ ),n = 3]Table 7. Growth curve of oe-Orai3 CASMC cells by cell counting assay[ ($\bar x \pm s $ ),n = 3]时间(h) oe-NC oe-Orai3 t P 24 2.5000 ± 0.8660 5.9170 ± 2.0050 2.7090 0.0536 48 10.0800 ± 1.8430 24.1700 ± 2.0210 8.9190 0.0009 ** 72 17.0800 ± 1.7740 26.6700 ± 2.0820 6.0690 0.0037** 96 19.7500 ± 3.4370 30.1700 ± 3.2150 3.8340 0.0186* oe-NC为转染阴性对照组,Orai2、Orai3阴性对照组为同一空白载体;oe-Orai2为过表达Orai2质粒DNA组,oe-Orai3为过表达Orai3质粒DNA组。与NC组比较,*P < 0.05,**P < 0.01。  图 4 过表达Orai3后CASMC细胞增殖情况A:过表达Orai3后CASMC细胞提取蛋白Western Blot检测Orai3表达量条带图;B:过表达Orai3后Western Blot实验检测干扰效率;C:过表达Orai3后QPCR实验检测干扰效率;D:过表达Orai3后CCK8实验检测CASMC细胞增殖情况;E:过表达Orai3后细胞计数实验检测CASMC细胞增殖情况;oe-NC:Orai3干扰阴性对照组即空白载体;oe-Orai3:Orai3干扰组。与FBS+比较,*P < 0.05,**P < 0.01。Figure 4. Orai2 over-expression and the Coronary vessel smooth muscle cell proliferation
图 4 过表达Orai3后CASMC细胞增殖情况A:过表达Orai3后CASMC细胞提取蛋白Western Blot检测Orai3表达量条带图;B:过表达Orai3后Western Blot实验检测干扰效率;C:过表达Orai3后QPCR实验检测干扰效率;D:过表达Orai3后CCK8实验检测CASMC细胞增殖情况;E:过表达Orai3后细胞计数实验检测CASMC细胞增殖情况;oe-NC:Orai3干扰阴性对照组即空白载体;oe-Orai3:Orai3干扰组。与FBS+比较,*P < 0.05,**P < 0.01。Figure 4. Orai2 over-expression and the Coronary vessel smooth muscle cell proliferation3. 讨论
本研究结果表明Orai3在大鼠冠状动脉血管平滑肌细胞(CASMC)体外实验中促进CASMC增殖。首先,无血清培养抑制CASMC增殖,且同时Orai3表达量在RNA和蛋白水平均有下降,表明抑制CASMC增殖时Orai3表达量降低;其次,干扰Orai3抑制CASMC增殖,过表达Orai3促进CASMC增殖。
本实验表明血清饥饿抑制平滑肌细胞增殖。血清饥饿被定义为在血清减少,无血清或无血清和蛋白培养基环境中生长细胞,被用作分子机理研究的研究工具,如细胞增殖等多种生理过程。血清饥饿对不同蛋白的表达及磷酸化也有不同作用[7],不同细胞种类对血清饥饿的反应不同,且有不同的蛋白质的磷酸化等反应[8]。因此有必要验证血清饥饿与CASMC增殖的关系。由于冠心病病理机制之一是冠状动脉血管平滑肌细胞增殖,因此选择增殖型CASMC而非收缩型CASMC作为研究样本,即为培养5代以后的细胞,CCK8和细胞计数分别检测无血清培养液及10%血清培养液培养0 h,24 h,48 h,72 h,96 h的细胞增殖情况,结果显示无血清培养48 h后较正常血清培养组减少,P < 0.05,表明无血清培养抑制CASMC细胞增殖。选择QPCR从RNA水平和Western Blot从蛋白水平验证Orai3表达量,实验结果显示无血清组较10%血清组时Orai3表达量降低,P < 0.05。结合前期血清饥饿抑制CASMC增殖结果,表明冠状动脉血管平滑肌细胞(CASMC)增殖状态下Orai3表达量高,抑制CASMC增殖表达量下降。因此,笔者猜测Orai3影响CASMC增殖可能,并通过干扰和过表达Orai3进行验证。
进一步实验表明在体外实验中Orai3对冠状动脉血管平滑肌增殖有重要作用。钙离子是常见的第2信使,与多种生理功能有关,包括增殖、分化、分泌、免疫等。细胞增殖是通过细胞内与钙Ca2+信号相关的多种蛋白来协调的。实验证据表明,来自内质网的Ca2+的波动对细胞增殖具有关键的生理作用,内质网中Ca2+的消耗触发Ca2+通过质膜的内流,这种现象称为钙库操纵型钙内流(SOCE) [9]。钙释放激活钙调节器Orai是钙库操纵型钙内流SOCE的重要组成分子。目前在人类基因中鉴定到的有3个Orai同源物(Orai1-3),3种蛋白结构高度相似,但特征上有所不同,可形成不同性质的异质通道。已有研究表明[10]Orai1促进血管平滑肌细胞增殖作用。钙释放激活钙通道CRAC主要由Orai1组成,但是有研究表明Orai2和Orai3亚基也有参与[11]。HEK293和Hela细胞中Orai1和Orai3的表达水平决定细胞增殖速率,沉默Orai1或Orai3使细胞增殖速率降低50%,过表达Orai1或Orai3使细胞增殖速率增加50%[12]。在重组前列腺癌细胞体外模型中证明,增强的Orai3表达促进增殖[13]。笔者对CASMC中Orai3分子进行干扰干预,QPCR验证siOrai3干扰效率约80%,通过WB检测干扰后Orai3蛋白水平明显下降,P < 0.05。通过细胞计数和CCK8检测干扰Orai3后的CASMC的增殖情况:CASMC干扰Orai3后细胞增殖较阴性对照组有所下降,P < 0.05,证明干扰Orai3抑制冠状动脉血管平滑肌细胞增殖。对CASMC中Orai3分子进行过表达干预,QPCR实验显示Orai3表达量明显升高(约阴性对照组4倍),WB实验显示转染后Orai2和Orai3蛋白水平均较前有所升高,P < 0.05。通过细胞计数和CCK8检测过表达Orai3后的CASMC增殖情况,过表达后CASMC增殖较阴性对照组升高,P < 0.05,证明过表达Orai2、Orai3促进冠状动脉血管平滑肌细胞增殖。
综上所述,Orai3在体外实验中促进冠状动脉血管平滑肌细胞增殖。目前钙库操纵型钙通道是细胞增殖的研究热门,而Orai蛋白作为通道的一个门控蛋白在其中起到关键作用,Orai家族中Orai1已有多项研究表明与血管平滑肌细胞增殖有重要作用,而Orai3则多与肿瘤细胞增殖等研究较多见,且被认为是一类潜在的抗肿瘤机制[14]。冠状动脉血管平滑肌细胞增殖是冠心病进展的一大主要病理机制,因此Orai3可能是冠心病防治及治疗的一个新的靶点。因Orai3在哺乳动物中不仅参与了钙库操纵型钙通道,还参与了受体操纵型钙通道,而因此对于其与血管平滑肌细胞增殖的影响的研究仍需进一步验证此促进作用属于哪种机制,此外仍需进行动物实验进行体内实验验证。
-
表 1 基线数据($\bar x \pm s $)
Table 1. Baseline data($\bar x \pm s $)
组别 年龄(岁) n(男/女) 基线眼轴(mm) 基线屈光度(D) 对照组 11.36±1.53 52(26/26) 24.22±0.81 −2.01±0.68 实验组 10.70±1.67 78(43/35) 24.33±0.79 −1.90±0.67 χ2/t −3.202 0.646 1.068 1.247 P 0.002* 0.422 0.286 0.214 *P <0.05。  下载: 导出CSV
下载: 导出CSV
表 2 戴镜前后屈光度的变化($\bar x \pm s $)
Table 2. Change in diopter before and after wearing glasses ($\bar x \pm s $)
组别 戴镜前(D) 戴镜后(3个月) 戴镜后(6个月) 戴镜后(9个月) 戴镜后(12个月) 对照组(n=104) −2.01±0.68 −2.14±0.72 −2.41±0.78 −2.59±0.83 −2.78±0.82 实验组(n=156) −1.90±0.67 −1.96±0.72 −2.07±0.74 −2.13±0.75 −2.18±0.78 t 1.247 1.952 3.582 4.690 5.981 P 0.214 0.052 <0.001* <0.001* <0.001* *P <0.05。
下载: 导出CSV
表 3 戴镜前后眼轴的变化($\bar x \pm s $)
Table 3. Changes of eye axis before and after wearing glasses ($\bar x \pm s $)
组别 戴镜前(D) 戴镜后(3个月) 戴镜后(6个月) 戴镜后(9个月) 戴镜后(12个月) 对照组(n=104) 24.22±0.81 24.32±0.80 24.44±0.77 24.52±0.77 24.62±0.78 实验组(n=156) 24.33±0.79 24.37±0.79 24.40±0.78 24.44±0.81 24.51±0.80 t 1.068 0.447 −0.404 −0.856 −1.093 P 0.286 0.655 0.686 0.393 0.275
下载: 导出CSV
-
[1] Eyayu G. Causes of blindness and vision impairment in 2020 and trends over 30 years,and prevalence of avoidable blindness in relation to VISION 2020: The right to sight: An analysis for the global burden of disease study[J]. Lancet Glob Health,2021,9(2):e144-e160. doi: 10.1016/S2214-109X(20)30489-7 [2] Holden B A ,Fricke T R ,Wilson D A ,et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050[J]. Ophthalmology,2016,123(5): 1036. [3] Baird P N,Saw S M,Lanca C,et al. Myopia[J]. Nat Rev Dis Primers,2020,6(1):99 doi: 10.1038/s41572-020-00231-4 [4] Zhang H ,Lam C,Tang W ,et al. Changes in relative peripheral refraction in children who switched from single-vision lenses to defocus incorporated multiple segments lenses[J]. Ophthalmic and Physiological Optics,2022,43(3):319-326. [5] Dong L,Kang Y K,Li Y,et al. Prevalence and time trends of myopia in children and adolescents in China: A systemic review and meta-analysis[J]. Retina,2020,40(3):399-411 doi: 10.1097/IAE.0000000000002590 [6] Haarman A E G,Enthoven C A,Tideman J W L,et al. The complications of myopia: A review and meta-analysis[J]. The Association for Research in Vision and Ophthalmology,2020,61(4):49. [7] Li F F,Zhang Y,Zhang X,et al. Age effect on treatment responses to 0.05%,0.025%,and 0.01% atropine: Low-concentration atropine for myopia progression study[J]. Ophthalmology,2021,128(8):1180-1187. doi: 10.1016/j.ophtha.2020.12.036 [8] Zhang X J,Zhang Y,Yip Bhk,et al. Five-year clinical trial of the low-concentration atropine for myopia progression (LAMP) study: Phase 4 report[J]. Ophthalmology,2024,131(9):1011-1020. doi: 10.1016/j.ophtha.2024.03.013 [9] Huang J,Wen D,Wang Q,et al. Efficacy comparison of 16 interventions for myopia control in children: A network meta-analysis[J]. Ophthalmology,2016,123(4):697-708. doi: 10.1016/j.ophtha.2015.11.010 [10] Olenich M. Use of orthokeratology contact lenses in the treatment of progressive myopia spravočnik vrača obŝej praktiki[J]. Journal of Family Medicine,2020,53(7):18-22. [11] Smith M J,Walline J J. Controlling myopia progression in children and adolescents[J]. Adolesc Health Med Ther,2015,6(1):133-140. [12] Wallman J,Winawer J. Homeostasis of eye growth and the question of myopia[J]. Neuron,2004,43(4):447-468. doi: 10.1016/j.neuron.2004.08.008 [13] Zhang H Y ,Lam C S Y ,Tang W C ,et al. Impact of defocus incorporated multiple segments (DIMS) spectacle lenses on relative peripheral refraction (RPR): A 2-year randomized clinical trial[J]. Investigative Ophthalmology & Visual Science,2019,31(9):60-67. [14] Lam C S Y,Tang W C,Zhang H Y,et al. Long-term myopia control effect and safety in children wearing DIMS spectacle lenses for 6 years[J]. Sci Rep,2023,13(1):5475-5482. doi: 10.1038/s41598-023-32700-7 [15] Qin Z,Peng T,Zhang Z,et al. Myopia progression and stabilization in school-aged children with single-vision lenses[J]. Acta 0phthalmol,2021,100(4):e950-e956. [16] Li N,Lin W,Liang R,et al. Comparison of two different orthokeratology lenses and defocus incorporated soft contact (DISC) lens in controlling myopia progression[J]. Eye Vis (Lond),2023,10(1):43. doi: 10.1186/s40662-023-00358-x [17] Li S M,Kang M T,Wu S S,et al. Efficacy,safety and acceptability of orthokeratology on slowing axial elongation in myopic children by meta-analysis[J]. Curr Eye Res,2015,41(5):600-608. [18] Tu E Y,Joslin C E. Recent outbreaks of atypical contact lens-related keratitis: What have we learned?[J]. AM J 0phthalmol,2010,150(5):602-608. doi: 10.1016/j.ajo.2010.06.045 [19] Lee S, Won Y, Lim D. Major complications of overnight orthokeratology lens for myopic correction ann optom contact lens[J]. Ann Optom Contact Lens, 2022, 21(1): 1-7.Lee S,Won Y,Lim D. Major complications of overnight orthokeratology lens for myopic correction ann optom contact lens[J]. Ann Optom Contact Lens,2022,21(1):1-7. [20] Sankaridurg P,Weng R,Tran H,et al. Spectacle lenses with highly aspherical lenslets for slowing myopia: A randomized,double-blind,cross-over clinical trial: Parts of these data were presented as a poster at the annual research in vision and ophthalmology meeting,2022[J]. AM J Ophthalmol,2022,247(1):18-24. [21] Bao J,Huang Y,Li X,et al. Spectacle lenses with aspherical lenslets for myopia control vs single-vision spectacle lenses: A randomized clinical trial[J]. JAMA Ophthalmol,2022,140(5):472-478. doi: 10.1001/jamaophthalmol.2022.0401 [22] Yang J L,Li D L,Chen J,et al. Effect modification of time spent outdoors on the association between early childhood overweight and myopia: A one-year follow-up study[J]. J Public Health-Uk,2024,46(1):107-115. doi: 10.1093/pubmed/fdae006 -




 下载:
下载:













</td>
<td class="table_top_border table_bottom_border2" align="center" valign="middle"><i>n</i>(男/女)</td>
<td class="table_top_border table_bottom_border2" align="center" valign="middle">基线眼轴(mm)</td>
<td class="table_top_border table_bottom_border2" align="center" valign="middle">基线屈光度(D)</td>
</tr>
</thead>
<tbody>
<tr>
<td align="left" valign="middle">对照组</td>
<td align="left" valign="middle">11.36±1.53</td>
<td align="left" valign="middle">52(26/26)</td>
<td align="left" valign="middle">24.22±0.81</td>
<td align="left" valign="middle">−2.01±0.68</td>
</tr>
<tr>
<td align="left" valign="middle">实验组</td>
<td align="left" valign="middle">10.70±1.67</td>
<td align="left" valign="middle">78(43/35)</td>
<td align="left" valign="middle">24.33±0.79</td>
<td align="left" valign="middle">−1.90±0.67</td>
</tr>
<tr>
<td align="left" valign="middle"><i>χ</i><sup>2</sup><i>/t</i></td>
<td align="left" valign="middle">−3.202</td>
<td align="left" valign="middle">0.646</td>
<td align="left" valign="middle">1.068</td>
<td align="left" valign="middle">1.247</td>
</tr>
<tr>
<td class="table_bottom_border" align="left" valign="middle"><i>P</i></td>
<td class="table_bottom_border" align="left" valign="middle">0.002<sup>*</sup></td>
<td class="table_bottom_border" align="left" valign="middle">0.422</td>
<td class="table_bottom_border" align="left" valign="middle">0.286</td>
<td class="table_bottom_border" align="left" valign="middle">0.214</td>
</tr>
</tbody>
<tfoot>
<tr>
<td colspan="5" align="left" valign="middle"> <sup>*</sup><i>P</i> <0.05。</td>
</tr>
</tfoot>
</table></div></foreignObject></svg>)
