

Clinical Study on Characteristics of Kawasaki Disease in Yunnan Province
-
摘要:
目的 探讨川崎病(Kawasaki disease,KD)在云南儿童间的发病和临床特征。 方法 回顾性分析云南省第三人民医院2013年1月至2018年12月间入院的163例川崎患者的资料,分析其临床特征与淋巴细胞亚群特点。 结果 患者年龄跨度较大(0~8岁),其中0~2岁患者占59.51%,患者出现结膜充血、口唇皲裂、皮疹、血沉(ESR)增快,C反应蛋白(CRP)升高、血小板增多,白细胞增高。此外患者还出现四肢末端改变、颈部淋巴结肿大、肛周皮肤潮红、卡巴症、贫血、中性粒细胞异常、WBC小于4 000等症状。心脏彩超结果显示,川崎病人心脏出现内膜不光滑、左右冠状动脉有扩张的症状。93.66%的川崎病患者CD19+升高,其他淋巴细胞亚群也出现变化,并且CD3+CD8+和CD3+CD4+与患者年龄相关(相关系数 > 0.2)。 结论 2岁以下儿童为易感群体,且患者急性期存在显著的免疫学紊乱,结合川崎病表征、血液指标、心脏彩超以及淋巴细胞亚群变化来进行诊断将更加科学合理。 Abstract:Objective To investigate the incidence and clinical features of Kawasaki disease(KD)among children in Yunnan province. Methods A total of 163 patients with Kawasaki disease were studied retrospectively. All of them were treated in the Third People's Hospital of Yunnan Province in Kunming from January 2013 to December 2018. The clinical features and lymphocyte subpopulations in the patients with Kawasaki disease were analyzed. Results 59.51% of the patients were 0~2 years old. Patients had conjunctival congestion, chapped lips, rash, abnormal erythrocyte sedimentation rate(ESR), elevated C-reactive protein(CRP), platelet count greater than 500, and white blood cell(WBC)greater than 10 000. In addition, extremity changes, cervical lymphadenopathy, perianal skin flushing, kappa disease, anemia, neutrophil abnormalities, and WBC less than 4000 were also detected in patients with Kawasaki disease. The results of color Doppler ultrasound showed that the intima of Kawasaki patients was not smooth and the left and right coronary arteries were dilated. CD19+ was increased in 93.66% of Kawasaki disease patients, and other lymphocyte subsets were also changed. CD3+CD8+ and CD3+CD4+ were significantly correlated with age(Pearson Correlation Coefficicient > 0.2). Conclusion Children under 2 years old are susceptible groups, and there are significant immunologic disorders in acute phase in the patients with Kawasaki disease. It is more scientific and reasonable to diagnose Kawasaki disease by combining the characteristics of Kawasaki disease, blood parameters, cardiac color Doppler ultrasound and lymphocyte subsets. -
Key words:
- Kawasaki disease /
- Clinical features /
- Lymphocyte subsets /
- Age relation
-

图 1 川崎病人的临床表现(n = 163)
A:川崎病人各年龄段比例;B:川崎病人外表征比例;C:川崎病人血检验指标比例;D:川崎病人心脏彩超异常比例。
Figure 1. Clinical features of the patients with Kawasaki disease(n = 163)

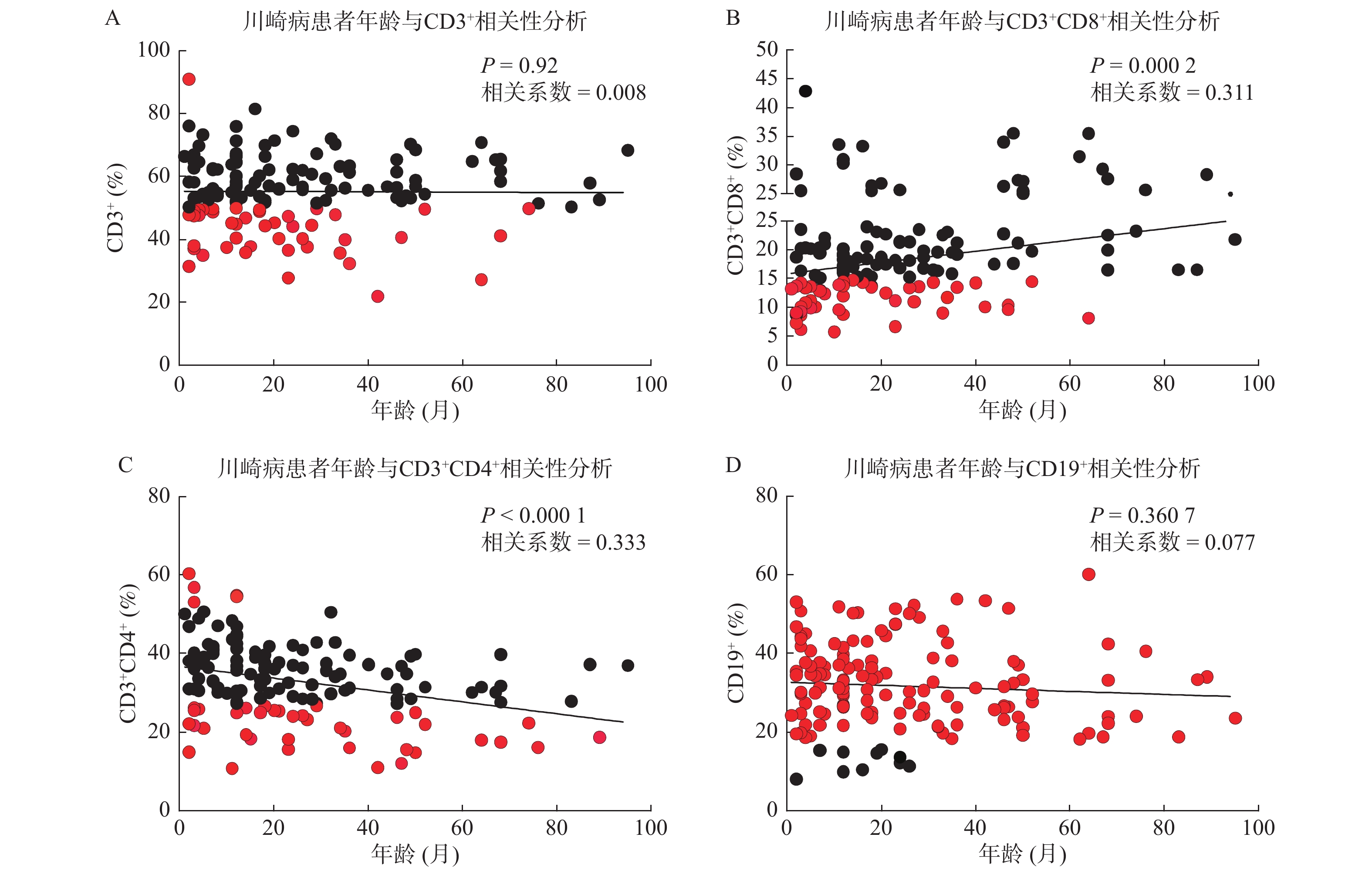
图 2 川崎病患者急性期淋巴细胞亚群与年龄相关性分析
A:川崎病患者年龄与CD3+相关性分析;B:川崎病患者年龄与CD3+CD8+相关性分析;C:川崎病患者年龄与CD3+CD4+相关性分析;D:川崎病患者年龄与CD19+相关性分析;n = 142;每个圆点代表一个个体,黑色圆点为正常范围内的检测值,红色圆点为异常检测值。Pearson相关系数 < 0.2为极弱相关或无相关,Pearson相关系数在0.2~0.4间为弱相关。
Figure 2. Correlation analysis of lymphocyte subsets and age in the patients with Kawasaki disease
表 1 川崎病人急性期淋巴细胞亚群的变化
Table 1. Changes of lymphocyte subpopulation in the patients with Kawasaki disease
检测项目 检出数(n) 检出率(%) CD3+ 正常范围 50%~84% 101 71.13 异常范围 < 50% 40 28.17 > 84% 1 0.70 CD3+CD8+ 正常范围 15%~44% 91 64.79 异常范围 < 15% 50 35.21 > 44% 0 0.00 CD3+CD4+ 正常范围 27%~51% 103 72.53 异常范围 < 27% 33 23.24 > 51% 6 4.23 CD16+CD56+ 正常范围 7%~40% 104 73.24 异常范围 < 7% 38 26.76 > 40% 0 0.00 CD19+ 正常范围 5%~18% 9 6.34 异常范围 < 5% 0 0.00 > 18% 133 93.66 CD4+/CD8+ 正常范围 0.7~2.8 111 78.17 异常范围 < 0.7 3 2.11 > 2.8 28 19.72  下载: 导出CSV
下载: 导出CSV
-
[1] Kawasaki T. Pediatric acute febrile mucocutaneous lymph node syndrome with characteristic desquamation of fingers and toes:my clinical observation of fifty cases[J]. Pediatr Infect Dis J,2002,21(11):1-38. [2] Denby K J,Clark D E,Markham L W. Management of Kawasaki disease in adults[J]. Heart,2017,103(22):1760-1769. doi: 10.1136/heartjnl-2017-311774 [3] Dimitriades V R,Brown A G,Gedalia A. Kawasaki disease:pathophysiology,clinical manifestations,and management[J]. Curr Rheumatol Rep,2014,16(6):423. doi: 10.1007/s11926-014-0423-x [4] Kuwabara M,Yashiro M,Kotani K,et al. Cardiac lesions and initial laboratory data in Kawasaki disease:a nationwide survey in Japan[J]. J Epidemiol,2015,25(3):189-193. doi: 10.2188/jea.JE20140128 [5] Gamez L B,Moribe I,Cisneros M,et al. Kawasaki disease shock syndrome:Unique and severe subtype of Kawasaki disease[J]. Pediatr Int,2018,60(9):781-790. doi: 10.1111/ped.13614 [6] Lee K Y,Rhim J W,Kang J H. Kawasaki disease:laboratory findings and an immunopathogenesis on the premise of a “protein homeostasis system”[J]. Yonsei Med J,2012,53(2):262-275. doi: 10.3349/ymj.2012.53.2.262 [7] Hara T,Nakashima Y,Sakai Y,et al. Kawasaki disease:a matter of innate immunity[J]. Clin Exp Immunol,2016,186(2):134-143. doi: 10.1111/cei.12832 [8] Newburger J W,Takahashi M,Gerber M A,et al. Diagnosis,treatment,and long-term management of Kawasaki disease:a statement for health professionals from the Committee on Rheumatic Fever,Endocarditis and Kawasaki Disease,Council on Cardiovascular Disease in the Young,American Heart Association[J]. Circulation,2004,110(17):2747-2771. doi: 10.1161/01.CIR.0000145143.19711.78 [9] Rife E,Gedalia A. Kawasaki Disease:an Update[J]. Curr Rheumatol Rep,2020,22(75):1-10. [10] Phuong L K,Bonetto C,Buttery J,et al. Kawasaki disease and immunisation:A systematic review[J]. Vaccine,2017,35(14):1770-1779. doi: 10.1016/j.vaccine.2016.09.033 [11] Maric L S,Knezovic I,Papic N,et al. Risk factors for coronary artery abnormalities in children with Kawasaki disease:a 10-year experience[J]. Rheumatol Int,2015,35(28):1053-1058. [12] Ghelani S J,Sable C,Wiedermann B L,et al. Increased incidence of incomplete Kawasaki disease at a pediatric hospital after publication of the 2004 American Heart Association guidelines[J]. Pediatr Cardiol,2012,33(4):1097-1103. [13] Anne H R,Susan C B,David A,et al. A protein epitope targeted by the antibody response to kawasaki disease[J]. J Pediat Inf Dis Soc,2020,222(1):158-168. [14] Ramphul K,Mejias S G. Kawasaki disease:a comprehensive review[J]. Arch Med Sci Atheroscler Dis,2018,3(1):e41-e45. doi: 10.5114/amsad.2018.74522 [15] Makino N,Nakamura Y,Yashiro M,et al. Descriptive epidemiology of Kawasaki disease in Japan,2011–2012:from the results of the 22nd nationwide survey[J]. J Epidemiol,2015,25(3):239-245. doi: 10.2188/jea.JE20140089 [16] Singh S,Gupta M,Bansal A,et al. A comparison of the clinical profile of Kawasaki disease in children from Northern India above and below 5 years of age[J]. Clin Exp Rheumatol,2007,25(4):654-657. [17] Tsuchida S,Yamanaka T,Tsuchida R,et al. Epidemiology of infant Kawasaki disease with a report of the youngest neonatal case ever reported in Japan[J]. Acta Paediatr,1996,85(8):995-997. doi: 10.1111/j.1651-2227.1996.tb14201.x [18] Mitchell S,Francis J,Burgner D. Kawasaki disease in the neonatal period[J]. J Pediat Inf Dis-ger,2011,6(4):265-267. [19] Salgado A P,Ashouri N,Berry E K,et al. High risk of coronary artery aneurysms in infants younger than 6 months of age with Kawasaki disease[J]. J Pediatr,2017,185(1):112-116. [20] Ogura M,Inoue T,Yamaki J,et al. Mitochondrial reactive oxygen species suppress humoral immune response through reduction of CD19 expression in B cells in mice[J]. Eur J Immunol,2017,47(2):406-418. doi: 10.1002/eji.201646342 [21] Brown T J,Crawford S E,Cornwall M L,et al. CD8 T lymphocytes and macrophages infiltrate coronary artery aneurysms in acute Kawasaki disease[J]. J Infect Dis,2001,184(1):940-943. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 4057
- HTML全文浏览量: 2460
- PDF下载量: 9
- 被引次数: 0
