

Molecular Epidemiology of Human Rhinovirus in 2 260 Children with Acute Lower Respiratory Tract Infection
-
摘要:
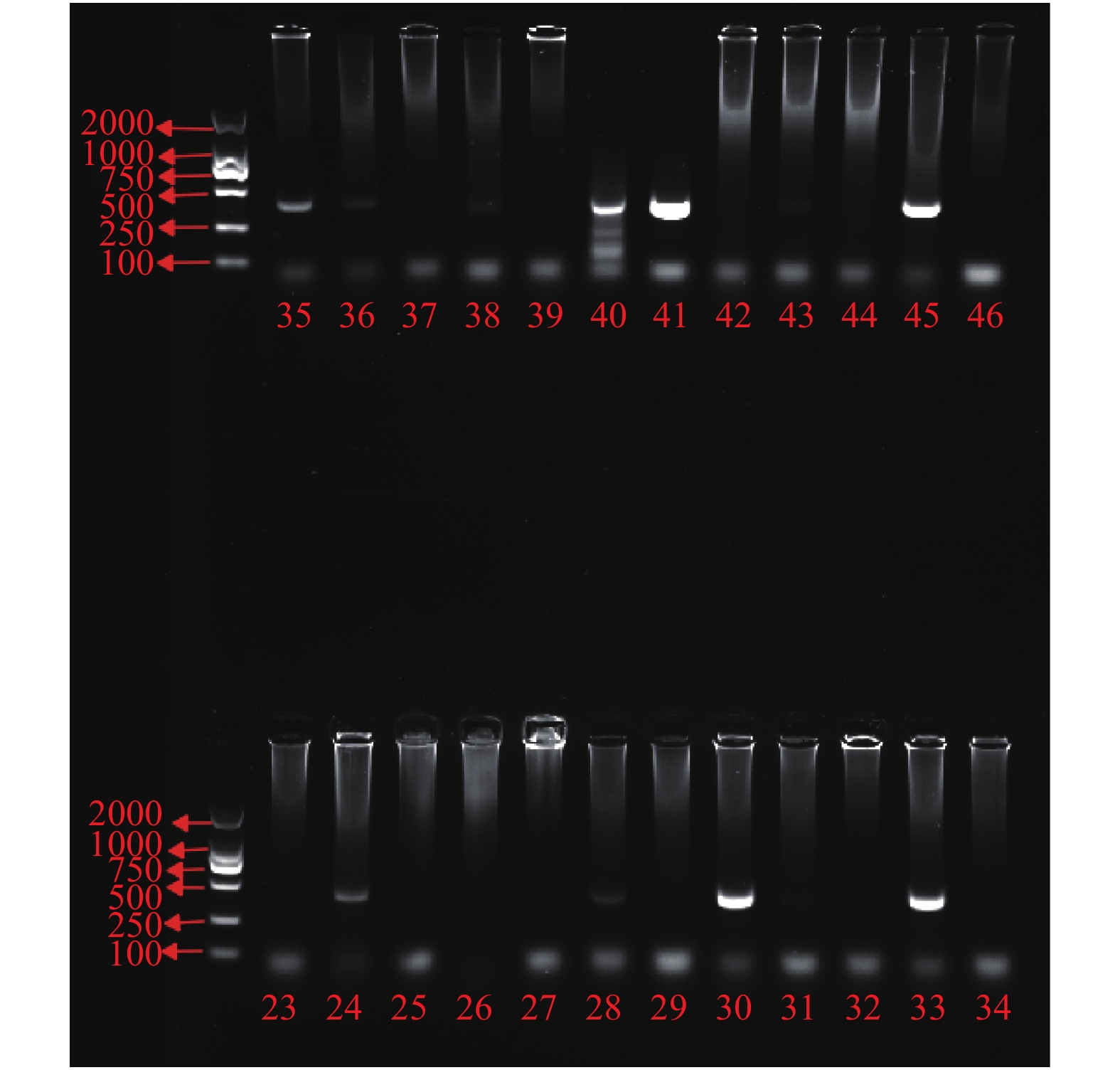
目的 了解昆明地区急性下呼吸道感染(acute lower respiratory tract infection,ALRTI)住院患儿人鼻病毒(human rhinovirus,HRV)感染的分子流行病学特征。 方法 选取2019年1月至2019年12月在昆明市儿童医院住院的ALRTI患儿共2260例作为研究对象,利用逆转录聚合酶链式反应(RT-PCR)对其鼻咽抽吸物或痰液进行HRV检测,随机选取40份HRV检测阳性标本扩增VP4/VP2基因片段,并对扩增产物进行测序分型。 结果 ALRTI患儿HRV检出率为6.50%(147/2260)。不同年龄段ALRTI患儿HRV检出率不存在差异(χ2 = 3.240,P = 0.356)。不同季节ALRTI患儿HRV检出率存在差异,夏季最高,其次为秋季(χ2 = 37.674,P < 0.05)。随机检测的40份阳性标本中,23份为HRV-A型,5份为HRV-B型,12份为HRV-C型。HRV检测阳性与HRV检测阴性患儿的临床表现在发热、咳嗽方面,差异无统计学意义( P > 0.05),但在喘息方面,差异有统计学意义( P < 0.05)。 结论 HRV是昆明地区急性下呼吸道感染的病原体之一,流行季节在夏秋季,以HRV-A型为主,感染HRV患儿更容易出现喘息。 Abstract:Objective To investigate the molecular epidemiological characteristics of human rhinovirus (HRV) infection in hospitalized children with acute lower respiratory tract infection (ALRTI) in Kunming. Methods A total of 2260 children with ALRTI who were hospitalized in Kunming children's Hospital from January 2019 to December 2019 were selected. HRV was detected by reverse transcription polymerase chain reaction (RT-PCR) in nasopharyngeal aspirates or sputum. 40 HRV positive samples were randomly selected to amplify VP4 / VP2 gene fragment, and the amplified products were sequenced and their types were identified. Results The positive rate of HRV was 6.50% (147 / 2260). There was no significant difference in HRV positive rate among different age groups (χ2 = 3.240, P = 0.356). The positive rate of HRV in children with ALRTI was significantly different in different seasons, the peak is in summer, followed by autumn (χ2 = 37.674, P < 0.05). Among the 40 positive samples, 23 were HRV-A, 5 were HRV-B and 12 were HRV-C. There was no significant difference in fever and cough between HRV positive and HRV negative children ( P > 0.05), but there was significant difference in wheezing ( P < 0.05). Conclusion HRV is one of the pathogens of acute lower respiratory tract infection in Kunming area. The epidemic season is summer and autumn and HRV-A is the main type. Children infected with HRV are more likely to have wheezing. -
Key words:
- Rhinovirus /
- Respiratory tract infection /
- Children /
- Epidemiology
-
表 1 不同年龄ALRTI患儿HRV检出情况[n(%)]
Table 1. HRV detection in children with ALRTI in different age groups [n(%)]
年龄(岁) < 1 1~2 3~5 ≥6 χ2 P RV检测结果 阳性 72(6.704) 40(6.885) 25(7.143) 10(3.922) 3.24 0.356 阴性 1002(93.296) 541(93.115) 325(92.857) 245(96.078) 合计 1074(100.000) 581(100.000) 350(100.000) 255(100.000)  下载: 导出CSV
下载: 导出CSV
表 2 不同季节ALRTI患儿HRV检出情况[n(%)]
Table 2. HRV detection in children with ALRTI in different seasons[n(%)]
季节 春(3月~5月) 夏(6月~8月) 秋(9月~11月) 冬(12月~2月) χ2 P RV检测结果 阳性 33(5.622) 56(10.000) 49(8.673) 9(1.642) 37.674 P < 0.001 阴性 554(94.378) 504(90.000) 516(91.327) 539(98.358) 合计 587(100.000) 560(100.000) 565(100.000) 548(100.000)
下载: 导出CSV
表 3 HRV检测阳性与HRV检测阴性患儿的临床表现比较[n(%)]
Table 3. Comparison of clinical manifestations of children with positive HRV test and negative HRV test [n(%)]
临床表现 HRV检测 合计 P 阳性 阴性 发热 有 62(42.177) 704(33.318) 766(33.894) 0.301 无 85(57.823) 1409(66.682) 1494(66.106) 咳嗽 有 20(13.605) 331(15.665) 351(15.531) 0.712 无 127(86.395) 1782(84.335) 1 909(84.469) 喘息 有 23(15.646) 104(4.922) 127(5.619) 0.030 无 124(84.354) 2 009(95.078) 2133(94.381)
下载: 导出CSV
-
[1] Royston L,Tapparel C. Rhinoviruses and Respiratory Enteroviruses:Not as Simple as ABC[J]. Viruses,2016,8(1):E16. doi: 10.3390/v8010016 [2] 江载芳, 申昆玲, 沈颖. 诸福棠实用儿科学[M]. 第8版, 北京: 人民卫生出版社, 2015: 1247-1253. [3] Wisdom A,Leitch E C,Gaunt E,et al. Screening respiratory samples for detection of human rhinoviruses (HRVs) and enteroviruses:Comprehensive VP4-VP2 typing reveals high incidence and genetic diversity of HRV species C[J]. J Clin Microbiol,2009,47(12):3958-3967. doi: 10.1128/JCM.00993-09 [4] Harvala H,Simmonds P. Human parechoviruses:Biology,Epidemiology and clinical significance[J]. J Clin Virol,2009,45(1):1-9. doi: 10.1016/j.jcv.2009.03.009 [5] Costa L F,Queiróz D A,Lopes da Silveira H,et al. Human rhinovirus and disease severity in children[J]. Pediatrics,2014,133(2):e312-321. doi: 10.1542/peds.2013-2216 [6] Hartiala M,Lahti E,Forsström V,et al. Characteristics of hospitalized rhinovirus-associated community-acquired pneumonia in children,finland,2003-2014[J]. Front Med (Lausanne),2019,6:235. doi: 10.3389/fmed.2019.00235 [7] Spichak T V,Yatsyshina S B,Кatosova L К,et al. Is the role of rhinoviruses as causative agents of pediatric community-acquired pneumonia over-estimated?[J]. Eur J Pediatr,2016,175(12):1951-1958. doi: 10.1007/s00431-016-2791-x [8] Liu G S,Li H,Zhao S C,et al. Viral and bacterial etiology of acute febrile respiratory syndrome among patients in qinghai,China[J]. Biomed Environ Sci,2019,32(6):438-445. [9] Zhao Y,Lu R,Shen J,et al. Comparison of viral and epidemiological profiles of hospitalized children with severe acute respiratory infection in Beijing and Shanghai,China[J]. BMC Infect Dis,2019,19(1):729. doi: 10.1186/s12879-019-4385-5 [10] 赵梦川,吴勇,黄迎彬,等. 河北省重症肺炎患儿非细菌性呼吸道病原学研究[J].河北医药,2020,42(5):774-778. doi: 10.3969/j.issn.1002-7386.2020.05.033 [11] Freymuth F,Vabret A,Dina J,et al. Bronchiolitis viruses[J]. Arch Pediatr,2010,17(8):1192-201. doi: 10.1016/j.arcped.2010.05.006 [12] Miller E K,Lu X,Erdman D D,et al. Rhinovirus-associated hospitalizations in young children[J]. J Infect Dis,2007,195(6):773-781. doi: 10.1086/511821 [13] Wang W,Cavailler P,Ren P,et al. Molecular monitoring of causative viruses in child acute respiratory infection in endemo-epidemic situations in Shanghai[J]. J Clin Virol,2010,49(3):211-218. doi: 10.1016/j.jcv.2010.08.005 [14] Jin Y,Yuan X H,Xie Z P,et al. Prevalence and clinical characterization of a newly identified human rhinovirus C species in children with acute respiratory tract infections[J]. J Clin Microbiol,2009,47(9):2895-900. doi: 10.1128/JCM.00745-09 [15] Lu Q B,Wo Y,Wang L Y,et al. Molecular epidemiology of human rhinovirus in children with acute respiratory diseases in Chongqing,China[J]. Sci Rep,2014,4:6686. [16] Piralla A,Baldanti F,Gerna G. Phylogenetic patterns of human respiratory picornavirus species,including the newly identified group C rhinoviruses,during a 1-year surveillance of a hospitalized patient population in Italy[J]. J Clin Microbiol,2011,49(1):373-376. doi: 10.1128/JCM.01814-10 [17] Erkkola R,Turunen R,Risnen K,et al. Rhinovirus C is associated with severe wheezing and febrile respiratory illness in young children[J]. Pediatr Infect Dis J,2020,39(4):283-286. doi: 10.1097/INF.0000000000002570 [18] Psarras S,Volonaki E,Skevaki C L,et al. Vascular endothelial growth factor-mediated induction of angiogenesis by human rhinoviruses[J]. J Allergy Clin Immunol,2006,117(2):291-297. doi: 10.1016/j.jaci.2005.11.005 [19] Brownlee J W,Turner R B. New developments in the epidemiology and clinical spectrum of rhinovirus infections[J]. Curr Opin Pediatr,2008,20(1):67-71. doi: 10.1097/MOP.0b013e3282f41cb6 -

 点击查看大图
点击查看大图
图(1) / 表(3)
计量
- 文章访问数: 4380
- HTML全文浏览量: 2564
- PDF下载量: 49
- 被引次数: 0
