

Changes and Clinical Significance of Serum Cys C, β 2-MG, MCP-1 and Ang Ⅱ Levels in Patients with Chronic Renal Failure
-
摘要:
目的 探讨慢性肾功能衰竭(CRF)患者血清膀胱抑素C(Cys C)、β2-微球蛋白(β2-MG)、单核细胞趋化蛋白-1(MCP-1)、血管紧张素Ⅱ(AngⅡ)水平变化,分析其与CRF患者预后的关系。 方法 选择2017年1月至2019年1月深圳市南山区蛇口人民医院肾内科收治的68例CRF患者(CRF组)和50例健康体检者(对照组),检测血清Cys C 、β2-MG、MCP-1、ANG Ⅱ水平,比较组间差异。以CRF患者随访期间发生全因死亡为终点事件,分析Cys C 、β2-MG、MCP-1、ANG Ⅱ与CRF患者预后的关系。 结果 随访中位时间18(13~25)个月,23例死亡(死亡组),50例存活(存活组)。死亡组血清CysC、β2-MG、MCP-1、ANG Ⅱ水平均高于存活组和对照组,差异有统计学意义(P < 0.05)。CRF患者血清CysC、β2-MG、MCP-1、ANG Ⅱ水平随着慢性肾脏疾病(CKD)分级增加而升高,差异有统计学意义(P < 0.05),血清CysC、β2-MG、MCP-1、ANG Ⅱ水平与肾小球滤过率(eGFR)均呈负相关(r = −0.435、−0.406、−0.621、−0.594,P < 0.05),与尿白蛋白/肌酐比值(ACR)呈正相关(r = 0.406、0.435、0.562、0.503,P < 0.05)。ROC分析结果显示CysC、β2-MG、MCP-1、ANG Ⅱ预测CRF患者预后的曲线下面积(AUC)分别为0.681(95%CI:0.551~0.811)、0.649(95%CI:0.510~0.789)、0.917(95%CI:0.852~0.981)、0.838(95%CI:0.733~0.942)。Kaplan-Meier生存分析结果显示高水平CysC、β2-MG、MCP-1、ANG Ⅱ组患者生存时间短于低水平CysC、β2-MG、MCP-1、ANG Ⅱ组,差异有统计学意义(P < 0.05)。多因素COX风险回归分析高水平CysC、β2-MG、MCP-1、ANG Ⅱ是CRF全因死亡的独立危险因素(P < 0.001)。 结论 血清CysC、β2-MG、MCP-1、ANG Ⅱ水平与CRF患者肾损伤程度和不良预后密切相关,可作为CRF预后评估的辅助指标。 Abstract:Objective To investigate the changes of serum cystatin C(Cys C), β 2-microglobulin(β 2-MG), monocyte chemoattractant protein-1(MCP-1)and angiotension Ⅱ(ANG Ⅱ)levels in patients with chronic renal failure(CRF), and analyze the relationship between them and the prognosis of CRF patients. Methods From January 2017 to January 2019, 68 CRF patients(CRF group)and 50 healthy people(control group)were selected from the nephrology department of our hospital. The levels of Cys C, β 2-MG, MCP-1 and ANG Ⅱ in serum were measured, and the differences between the two groups were compared. The end point was all-cause death, the relationship between Cys C, β 2-MG, MCP-1, ANG Ⅱ and the prognosis of CRF patients was analyzed. Results The median follow-up time was 18(13-25)months, 23 cases died(death group), 50 cases survived(survival group). The serum levels of CysC, β 2-MG, MCP-1 and ANG Ⅱ in the death group were higher than those in the survival group and the control group(P < 0.05). The levels of CysC, β 2-MG, MCP-1 and ANG Ⅱ in CRF patients increased with the increase of CKD grading(P < 0.05). Serum CysC, β 2-MG, MCP-1, ANG Ⅱwere negatively correlated with estimated glomerular filtration rate(EGFR)(r = -0.435, -0.406, -0.621, -0.594, P < 0.05), and positively correlated with urinary albumin / creatinine ratio(ACR)(r = 0.406, 0.435, 0.562, 0.503, P < 0.05). ROC analysis showed that AUC of CysC, β 2-MG, MCP-1 and ANG Ⅱ were 0.681(95% CI: 0.551-0.811), 0.649(95% CI: 0.510-0.789), 0.917(95% CI: 0.852-0.981)and 0.838(95% CI: 0.733-0.942), respectively. Kaplan-Meier survival analysis showed that the survival time of high level CysC, β 2-MG, MCP-1, ANG Ⅱ group was shorter than that of low level CysC, β 2-MG, MCP-1, ANG Ⅱ group(P < 0.05). Multivariate Cox regression analysis showed high levels of CysC, β 2-MG, MCP-1 and ANG Ⅱ were independent risk factors for all-cause death of CRF(P < 0.001). Conclusion The serum levels of CysC, β 2-MG, MCP-1 and ANG Ⅱ are closely related to the degree of renal injury and poor prognosis in CRF patients, which can be used as an auxiliary index for the prognosis evaluation of CRF. -
Key words:
- Chronic renal failure /
- Cys C /
- β 2-MG /
- MCP-1 /
- ANG Ⅱ /
- All cause death
-

图 1 各参数预测CRF患者预后的ROC图
Figure 1. ROC diagram of each parameter predicting the prognosis of CRF patients

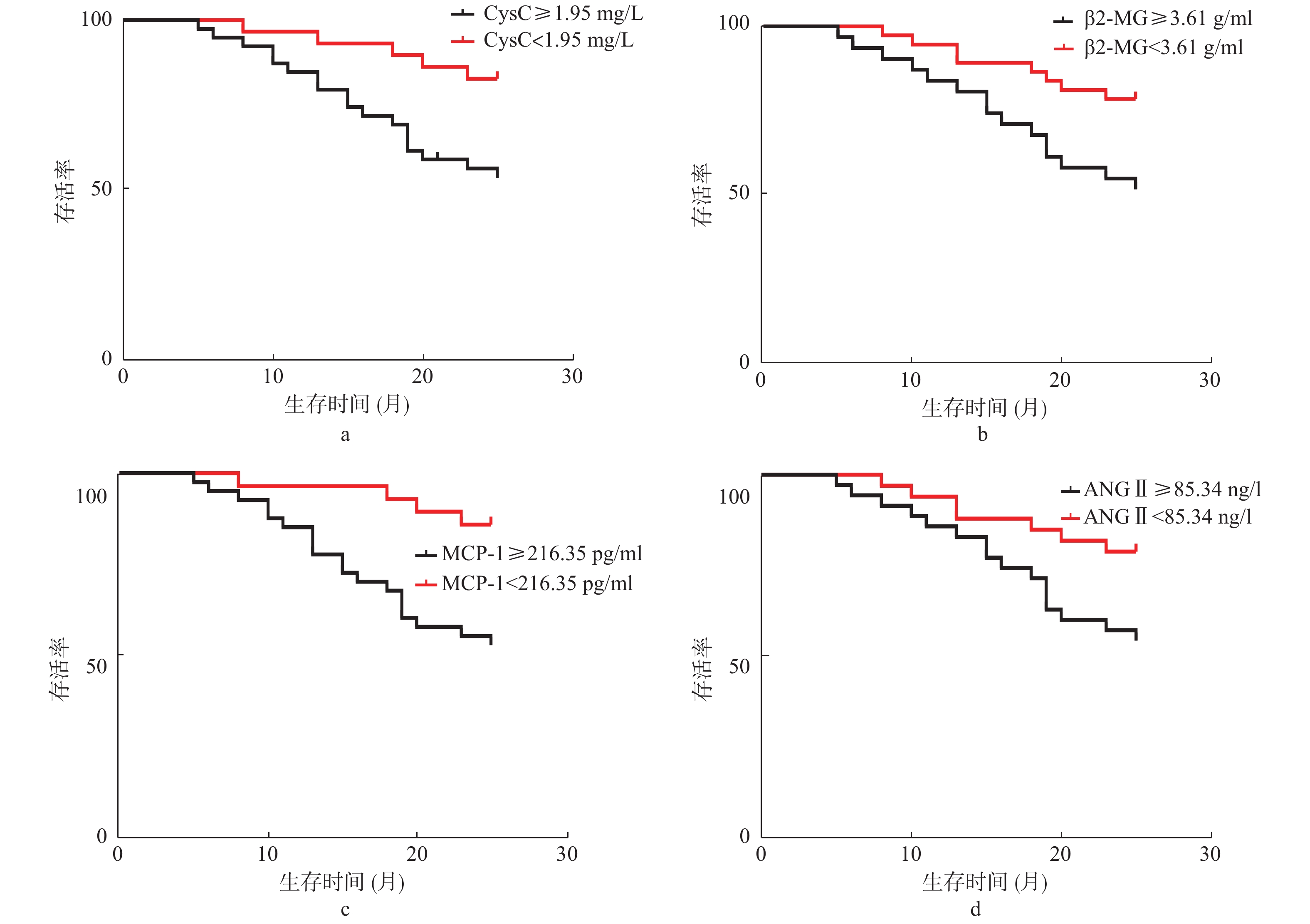
图 2 CRF患者生存曲线
a:不同CysC水平生存曲线;b:不同β2-MG水平生存曲线;c:不同MCP-1水平生存曲线;d:不同ANG Ⅱ水平生存曲线。
Figure 2. Survival curve of CRF patients
表 1 基线资料(
$\bar x\pm s $ )Table 1. Baseline data(
$\bar x\pm s $ )项目 死亡组(n = 23) 存活组(n = 45) 对照组(n = 50) F/t/χ2 P 性别[n(%)] 男 13(56.52) 29(64.44) 32(64.00) 0.470 0.791 女 10(43.48) 16(35.56) 18(36.00) 年龄(岁) 65.13 ± 4.18∆▲ 61.21 ± 5.49 60.35 ± 5.13 6.352 0.000 体质量(kg/m2) 25.50 ± 1.85 26.13 ± 2.31 25.31 ± 2.29 1.035 0.439 收缩压(mmHg) 145.16 ± 11.56∆▲ 135.13 ± 8.49∆ 120.32 ± 6.35 13.265 0.000 舒张压(mmHg) 76.23 ± 5.65∆ 77.14 ± 6.34∆ 53.26 ± 4.28 10.249 0.000 高血压[n(%)] 16(69.57)▲ 17(37.78) − 5.340 0.021 糖尿病[n(%)] 15(65.22)▲ 14(31.11) − 7.239 0.007 高血脂[n(%)] 10(43.48) 13(28.89) − 0.405 0.525 吸烟史[n(%)] 14(60.87)∆▲ 9(20.00) 8(16.00) 17.531 0.000 心肌梗死[n(%)] 13(56.52)▲ 11(24.44) − 6.858 0.009 脑卒中[n(%)] 6(26.09)▲ 3(6.67) − 4.999 0.025 TC(mmol/L) 5.47 ± 0.39∆ 5.12 ± 0.35∆ 4.03 ± 0.21 5.263 0.000 TG(mmol/L) 1.65 ± 0.71∆ 1.69 ± 0.81∆ 1.32 ± 0.36 4.235 0.003 HDL-C(mmol/L) 1.03 ± 0.46∆ 1.06 ± 0.43∆ 1.65 ± 0.13 6.359 0.000 LDL-C(mmol/L) 3.92 ± 0.65∆ 3.85 ± 0.51∆ 2.24 ± 0.28 4.523 0.001 CysC(mg/L) 2.43 ± 0.65∆▲ 1.09 ± 0.36∆ 0.73 ± 0.29 13.265 0.000 β2-MG(g/mL) 4.16 ± 0.65∆▲ 2.51 ± 0.45∆ 1.13 ± 0.29 21.352 0.000 MCP-1(pg/mL) 235.16 ± 35.26∆▲ 195.26 ± 32.56a 153.26 ± 20.46 17.598 0.000 AngⅡ(ng/L) 92.35 ± 13.26∆▲ 72.35 ± 9.35∆ 34.16 ± 5.23 26.351 0.000 eGFR[mL/(min·(1.73 m2)] 42.35 ± 6.59∆▲ 73.26 ± 12.64∆ 112.65 ± 15.37 53.264 0.000 ACR(mg/g) 305.26 ± 35.26∆b 165.26 ± 16.05∆ 3.26 ± 0.25 105.341 0.000 与对照组比较,∆P < 0.05;与存活组比较,▲P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 不同CKD分期CRF患者血清CysC、β2-MG、MCP-1、ANG Ⅱ水平差异(
$\bar x \pm s$ )Table 2. The difference of serum CysC,β2-MG,MCP-1,ANG Ⅱ levels in CRF patient in different CKD stage (
$\bar x \pm s $ )CKD分期 n CysC(mg/L) β2-MG(g/mLL) MCP-1(pg/mL) AngⅡ(ng/L) Ⅲ期 21 0.95 ± 0.25 2.13 ± 0.35 186.26 ± 18.52 63.25 ± 7.49 Ⅳ期 28 1.36 ± 0.43∆ 3.26 ± 0.59∆ 209.35 ± 24.16∆ 81.24 ± 10.25∆ Ⅴ期 19 2.45 ± 0.69∆▲ 3.82 ± 0.65∆▲ 232.74 ± 34.26∆▲ 95.67 ± 13.65∆▲ F 13.265 15.243 21.352 16.592 P 0.000 0.000 0.000 0.000 与Ⅲ期组比较,∆P < 0.05;与Ⅳ期组比较,▲P < 0.05。
下载: 导出CSV
表 3 生存分析资料及比较
Table 3. Survival analysis and comparison
指标 水平 血清检测水平 n 生存时间(月) Log-Rank (χ2,P) CysC 低水平 < 1.95 mg/L 29 25.13 ± 3.26 10.141, 0.000 高水平 ≥1.95 mg/L 39 18.35 ± 2.35 β2-MG 低水平 < 3.61 g/mL 37 24.13 ± 2.69 9.754, 0.002 高水平 ≥3.61 g/mL 31 18.34 ± 2.01 MCP-1 低水平 < 216.35 pg/mL 28 24.31 ± 2.69 12.554, 0.000 高水平 ≥216.35 pg/mL 40 17.34 ± 2.03 ANG Ⅱ 低水平 < 85.34 ng/L 33 25.03 ± 2.15 6.580, 0.010 高水平 ≥85.34 ng/L 35 18.34 ± 1.69
下载: 导出CSV
表 4 影响CRF患者预后的单因素和多因素COX风险回归模型
Table 4. Univariate and multivariate cox regression model of factors influencing the prognonsis of CRF patients
因素 单因素 多因素 RR 95%CI P值 RR 95%CI P值 收缩压 1.035 0.524~1.954 0.096 − − − 合并糖尿病 1.135 0.352~1.795 0.071 − − − 吸烟史 1.092 0.231~1.809 0.085 − − − 既往脑卒中 1.139 0.512~1.972 0.069 − − − ACR 1.126 0.633~2.251 0.057 − − − eGFR 1.625 1.035~16.254 0.002 − − − 既往心肌梗死 1.825 1.165~18.351 0.000 − − − 年龄 1.532 1.325~13.265 0.005 − − − 合并高血压 1.603 1.425~15.625 0.003 − − − CysC 1.998 1.324~20.112 0.000 1.824 1.325~18.245 0.000 β2-MG 1.856 0.625~1.824 0.000 1.623 1.135~13.265 0.000 MCP-1 2.056 1.325~10.254 0.000 2.016 1.854~25.352 0.000 ANG Ⅱ 1.936 1.542~15.342 0.000 1.822 1.354~19.547 0.000
下载: 导出CSV
-
[1] Eguchi M,Okumura K,Torigoe K,et al. Chronic renal failure as a possible risk factor for allergic reaction in therapeutic plasma exchange using fresh frozen plasma[J]. Ther Apher Dial,2019,23(3):261-265. doi: 10.1111/1744-9987.12823 [2] Mechler K,Liantonio J. Palliative care approach to chronic diseases:end stages of heart failure,chronic obstructive pulmonary disease,liver failure,and renal failure[J]. Prim Care,2019,46(3):415-432. doi: 10.1016/j.pop.2019.05.008 [3] 庞国菊,武玉晶,刘爽,等. 肝硬化继发急性肾损伤患者血清胱抑素C和中性粒细胞明胶酶相关脂质运载蛋白的水平及其诊断价值[J]. 中华肝脏病杂志,2019,27(1):65-67. doi: 10.3760/cma.j.issn.1007-3418.2019.01.015 [4] 阎双缓,何立芳,陈永良,等. HBV相关慢性肝炎、肝硬化和肝衰竭患者肾功能早期损伤指标观察[J]. 河北医药,2019,41(19):2979-2982. doi: 10.3969/j.issn.1002-7386.2019.19.026 [5] Gregg L P,Tio M C,Li X,et al. Association of monocyte chemoattractant protein-1 with death and atherosclerotic events in chronic kidney disease[J]. Am J Nephrol,2018,47(6):395-405. doi: 10.1159/000488806 [6] Franco M,Pérez-Méndez O,Kulthinee S,et al. Integration of purinergic and angiotensin II receptor function in renal vascular responses and renal injury in angiotensin II-dependent hypertension[J]. Purinergic Signal,2019,15(2):277-285. doi: 10.1007/s11302-019-09662-5 [7] 高翔,梅长林. 慢性肾脏病筛查诊断及防治指南[J]. 中国实用内科杂志,2017,37(1):28-34. [8] Kramer H,Toto R,Peshock R,et al. Association between chronic kidney disease and coronary artery calcification:the dallas heart study[J]. J Am Soc Nephrol,2005,16(2):507-513. doi: 10.1681/ASN.2004070610 [9] Levey A S,Bosch J P,Lewis J B,et al. A more accurate method to estimate glomerular filtration rate from serum creatinine:A new prediction equation. Modification of diet in renal disease study group[J]. Ann Intern Med,1999,130(6):461-470. doi: 10.7326/0003-4819-130-6-199903160-00002 [10] National Kidney F. K/doqi clinical practice guidelines for chronic kidney disease:Evaluation,classification,and stratification[J]. Am J Kidney Dis,2002,39(2 Suppl 1):S261-266. [11] Warram J H,Gearin G,Laffel L,et al. Effect of duration of typeⅠ diabetes on the prevalence of stages of diabetic nephropathy defined by urinary albumin/creatinine ratio[J]. J Am Soc Nephrol,1996,7(6):930-937. [12] 莫立仪. 红细胞分布宽度与血液透析患者心脑血管事件及死亡的相关性研究[D]. 广州: 南方医科大学硕士论文, 2016. [13] 段晓星,张国光,梦雅平. 慢性肾脏病住院死亡85例分析[J]. 内蒙古医学院学报,2009,31(2):101-104. [14] Mao W,Liu S,Wang K,et al. Cystatin C in evaluating renal function in ureteral calculi hydronephrosis in adults[J]. Kidney Blood Press Res,2020,45(1):109-121. doi: 10.1159/000504441 [15] Jiang Z,Tan Z,Meng F,et al. Curative effects of valsartan alone or combined with alpha-lipoic acid on inflammatory cytokines and renal function in early-stage diabetic kKidney disease[J]. J Coll Physicians Surg Pak,2019,29(10):1009-1011. doi: 10.29271/jcpsp.2019.10.1009 [16] Mulholland B S,Forwood M R,Morrison n a. monocyte chemoattractant protein-1 (mcp-1/ccl2) drives activation of bone remodelling and skeletal metastasis[J]. Curr Osteoporos Rep,2019,17(6):538-547. doi: 10.1007/s11914-019-00545-7 [17] 刘宇婷,孙维峰. 高尿酸血症患者血清脂联素、单核细胞趋化蛋白1水平变化及意义[J]. 山东医药,2017,57(21):5-8. doi: 10.3969/j.issn.1002-266X.2017.21.002 [18] 徐刚,王益群. 右美托咪啶对脓毒症急性肾损伤患者肾功能及血管紧张素Ⅱ表达的影响[J]. 中国医师杂志,2019,21(5):754-756. doi: 10.3760/cma.j.issn.1008-1372.2019.05.031 [19] Kang J S,Lee S J,Lee J H,et al. Angiotensin II-mediated MYH9 downregulation causes structural and functional podocyte injury in diabetic kidney disease[J]. Sci Rep,2019,9(1):7679. doi: 10.1038/s41598-019-44194-3 [20] 罗军,周晓萍,袁红伶,等. 慢性肾衰竭患者血清MCP-1、ANGⅡ水平变化[J]. 山东医药,2014,54(39):45-46. doi: 10.3969/j.issn.1002-266X.2014.39.016 [21] 江祥虎,钟志鹏. 慢性肾功能衰竭促进小鼠动静脉瘘内膜增生[J]. 基础医学与临床,2017,37(9):1293-1296. [22] Maciel R A,Rempel L C,Bosquetti B,et a1. p-cresol but not p-cresyl sulfate stimulate MCP-1 production via NF-kappaB p65 in human vascular smooth muscle cells[J]. J Bras Nefrol,2016,38(2):153-160. [23] Okamura K,Okuda T,Shirai K,et al. Positive correlation between blood pressure or heart rate and chymase-dependent angiotensin Ⅱ-forming activity in circulating mononuclear leukocytes measured by new ELISA[J]. Clin Exp Hypertens,2018,40(2):112-117. doi: 10.1080/10641963.2017.1339071 -





 点击查看大图
点击查看大图

计量
- 文章访问数: 3194
- HTML全文浏览量: 2272
- PDF下载量: 14
- 被引次数: 0
