

Application of Ultrasound-Targeted Microbubble Destruction with IL-6 Monoclonal Antibody in Rabbit Myocardial Ischemia-Reperfusion Injury
-
摘要:
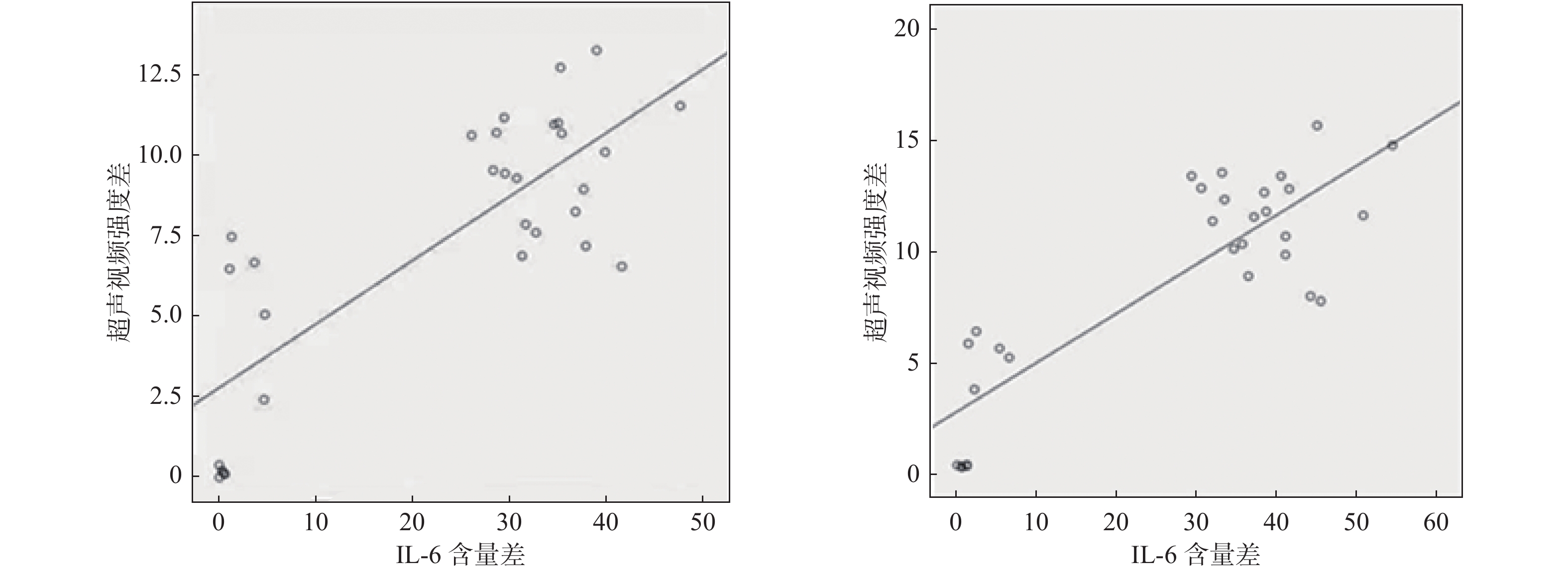
目的 探讨携IL-6单克隆抗体超声靶向微泡破坏技术(ultrasound-targeted microbubble destruction,UTMD)联合不同超声辐照强度在心肌缺血再灌注损伤(myocardial ischemia-reperfusion injury,MI/RI)中的应用价值。 方法 将大耳兔90只随机分为3组:A组(15只)关胸对照组、B组(15只)开胸对照组、C组(60只)缺血/再灌注组,其中C组又根据再灌注时间(30 min、60 min、120 min、180 min)分成T1、T2、T3、T4时段,各组再分为U0组(未经超声辐照)、U1组(0.5 w/cm2强度)、U2组(0.75 w/cm2强度)。将冠状动脉左前降支阻断30 min,解除阻断后得到MI/RI损伤模型,经耳缘静脉注射携IL-6单抗靶向造影剂,随后进行超声辐照。应用QLAB10.5软件分析辐照前、后再灌注损伤区心肌的视频强度,得到视频强度差值(video intensity difference,VID)。ELISA检测辐照前、后心肌组织中IL-6含量。 结果 T1-T4时段U2组VID值较U1组高(P < 0.05),各时段U2组和U1组VID值两两比较,差异无统计学意义(P > 0.05)。ELISA结果显示:超声辐照后,T1-T4时段,U2组IL-6含量比U1组低(P < 0.05);VID值和心肌组织内IL-6水平差值呈正相(rU1 = 0.745,rU2 = 0.734,P < 0.05);HE染色显示,U2组与U1组比较,炎性细胞浸润减少,心肌细胞损伤减轻。 结论 携IL-6单克隆抗体靶向微泡破坏技术联合超声辐照能有效缓解MI/RI的炎症反应,且在不损伤心肌的前提下,干预越早,辐照强度越强,减轻炎症反应的效果越佳。 -
关键词:
- 心肌缺血再灌注损伤 /
- 心肌声学造影 /
- 超声靶向微泡破坏技术 /
- IL-6单克隆抗体
Abstract:Objective To explore the application value of Ultrasound Targeted Microbubble Destruction (UTMD) with IL-6 monoclonal antibody combined with different ultrasonic irradiation intensity in myocardial ischemia-reperfusion injury (MI/RI). Methods Ninety rabbits were randomly divided into 3 groups, including 15 rabbits in the thoracotomy control group (group A), 15 rabbits in the thoracotomy control group (group B), and 60 rabbits in the R/I group (group C, divided into T1-T4 periods, reperfusion for 30 min, 60 min, 120 min, and 180 min). Each group was further divided into group U0 (without ultrasonic irradiation), group U1 (0.5 w/cm2 intensity), group U2 (0.75 w/cm2 intensity). An animal model of MI/RI was obtained by blocking the left anterior descending branch of the coronary artery for 30 min and then releasing it from reperfusion. The targeted contrast agent containing IL-6 was injected through ear vein, and then ultrasound irradiation was performed. QLAB10.5 software to analyze the video intensity of myocardium in reperfusion injury area before and after irradiation, and the ultrasonic video intensity difference (VID) was calculated. The content of IL-6 in the myocardium of each group before and after irradiation was detected by ELISA. Results The VID value of U2 group was higher than that of U1 group during T1-T4 (P < 0.05). The values of U2 and U1 VID in theT1-T4 period were compared in pairs within the group, the difference was not statistically significant (P > 0.05). ELISA analysis of rabbit myocardial tissue showed that the content of IL-6 in U2 group was lower than that in U1 group during T1-T4 period after ultrasonic irradiation (P < 0.05). The difference of IL-6 content between U1 group and U2group during T1-T4 was compared in pairs within the group, the difference was not statistically significant (P > 0.05). The difference of IL-6 content in myocardial tissue was positively correlated with the mean difference of ultrasonic video intensity (rU1 = 0.745, rU2 = 0.734). Conclusion IL-6 monoclonal antibody microbubbles combined with UTMD can effectively alleviate MI/RI inflammatory response, in addition, under the premise of no damage to the myocardium, the earlier the intervention, the stronger the radiation intensity, the better the effect of reducing the inflammatory response. -

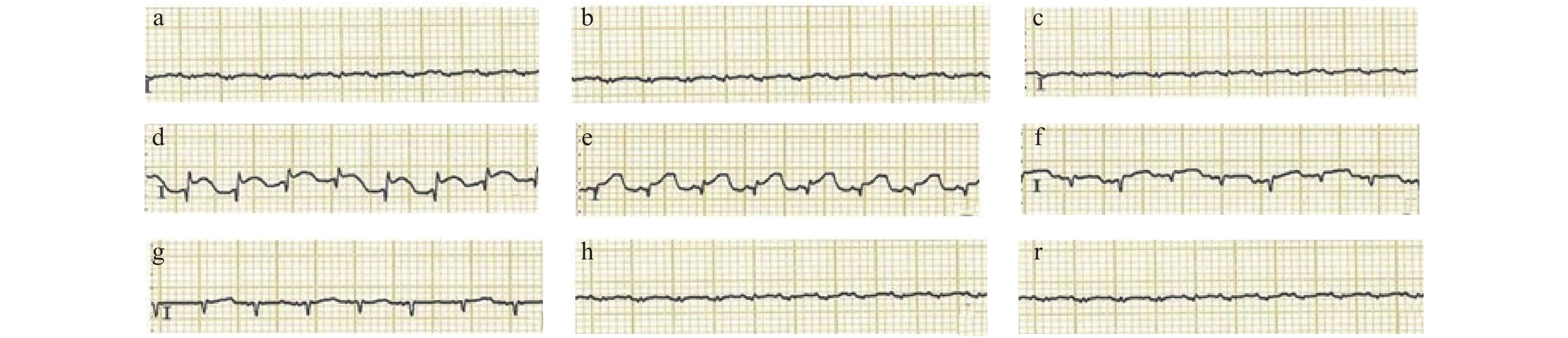
图 1 各组兔心电图表现
a:正常心电图;b:B组心电图;c:C组术中心电图;d:心梗30 min时心电图;e;再灌注30 min时心电图;f:再灌注45 min时心电图;g:再灌注60 min时心电图;h:再灌注120 min时心电图;r:再灌注180 min时心电图。
Figure 1. Electrocardiogram of rabbits in each group

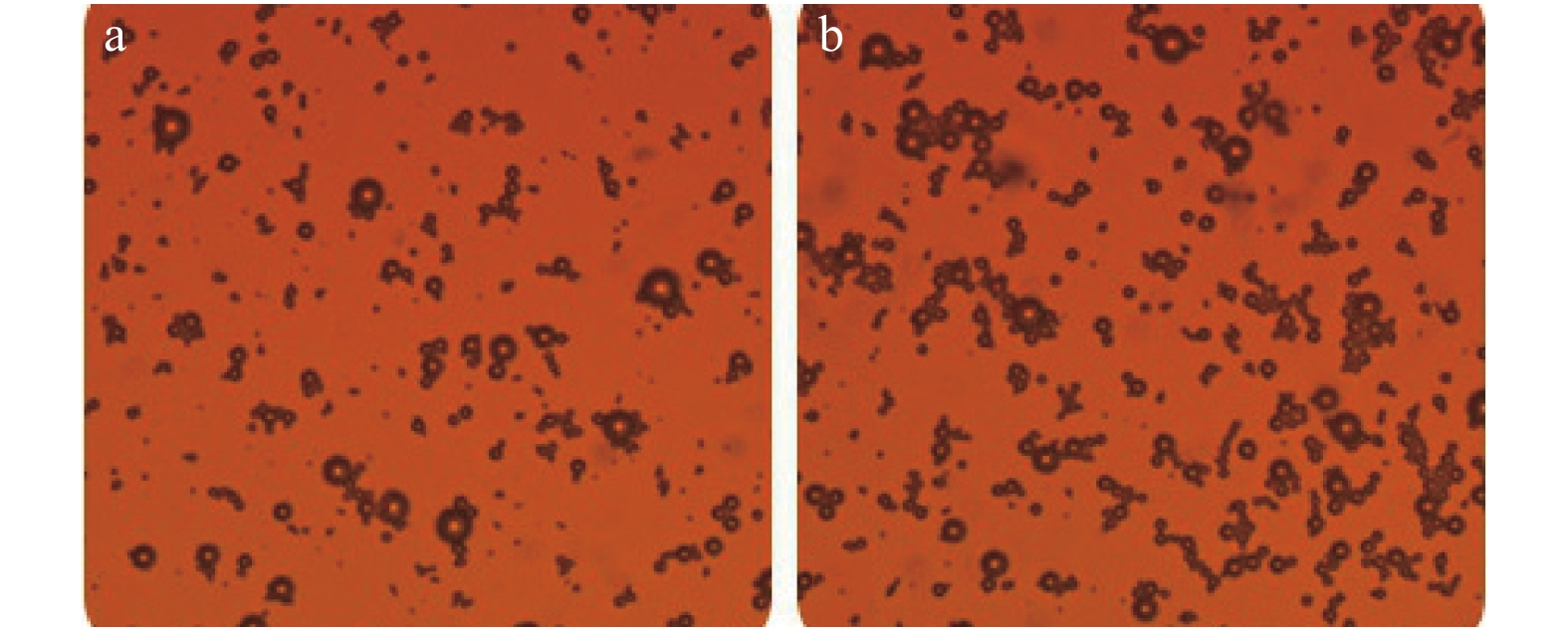
图 2 玻片凝集实验对靶向微气泡的检验
a:凝集反应(-);b:凝集反应(+)。
Figure 2. Test of targeted microbubbles by glass slide agglutination experiment

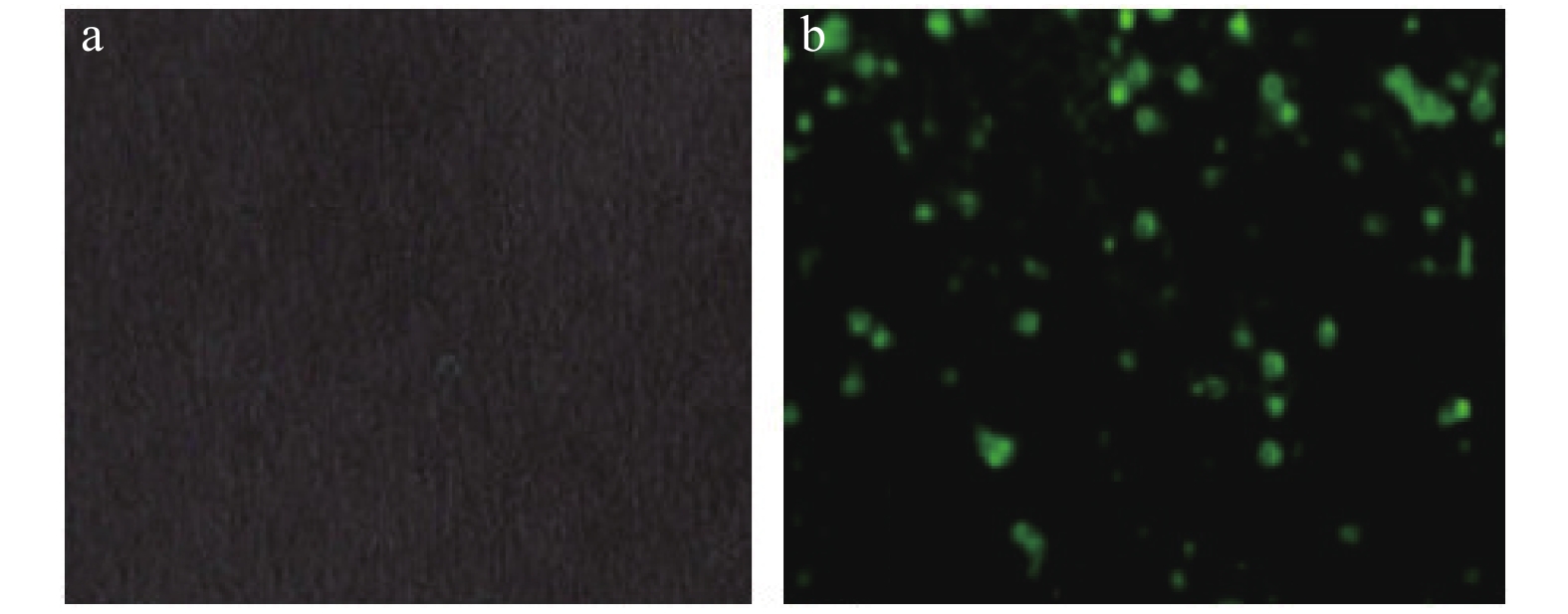
图 3 免疫荧光染色实验对靶向微气泡的检验
a:未见明显荧光显现;b:可见明显绿色荧光。
Figure 3. Detection of targeted microbubbles by immunofluorescence staining

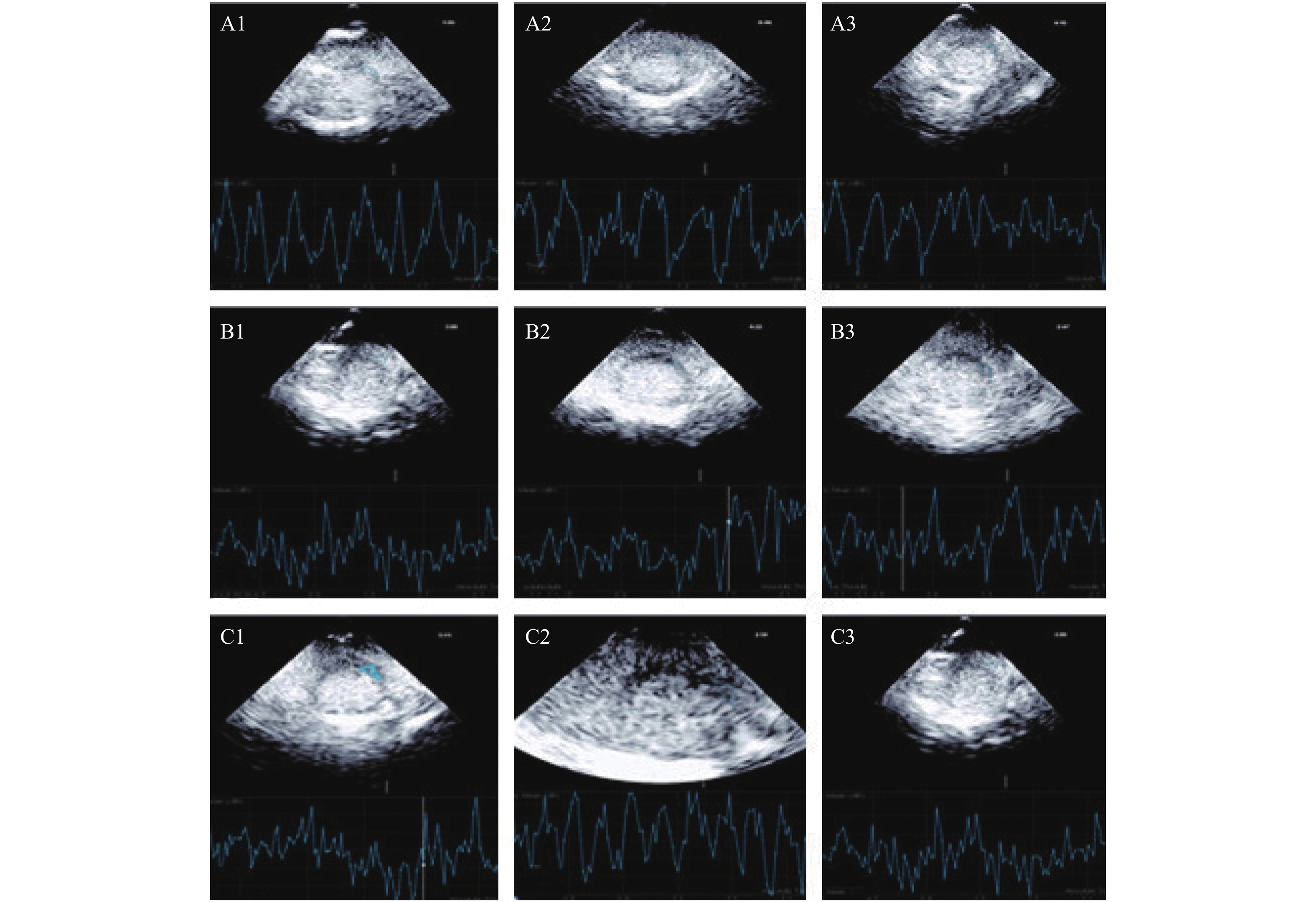
图 4 心肌组织超声辐照QLAB定量分析图
A1~A3:分别代表再灌注120 min:辐照前、0.5 w/cm2强度辐照后、0.75 w/cm2强度辐照后;B1~B3:分别代表开胸对照组:辐照前、0.5 w/cm2强度辐照后、0.75 w/cm2强度辐照后;C1~C3:分别代表关胸对照组:辐照前、0.5 w/cm2强度辐照后、0.75 w/cm2强度辐照后。
Figure 4. QLAB quantitative analysis of ultrasonic irradiation of myocardial tissue

图 5 VID值与心肌组织内IL-6水平差值的相关性分析
Figure 5. Correlation analysis of the difference between VID value and IL-6 level in myocardial tissue

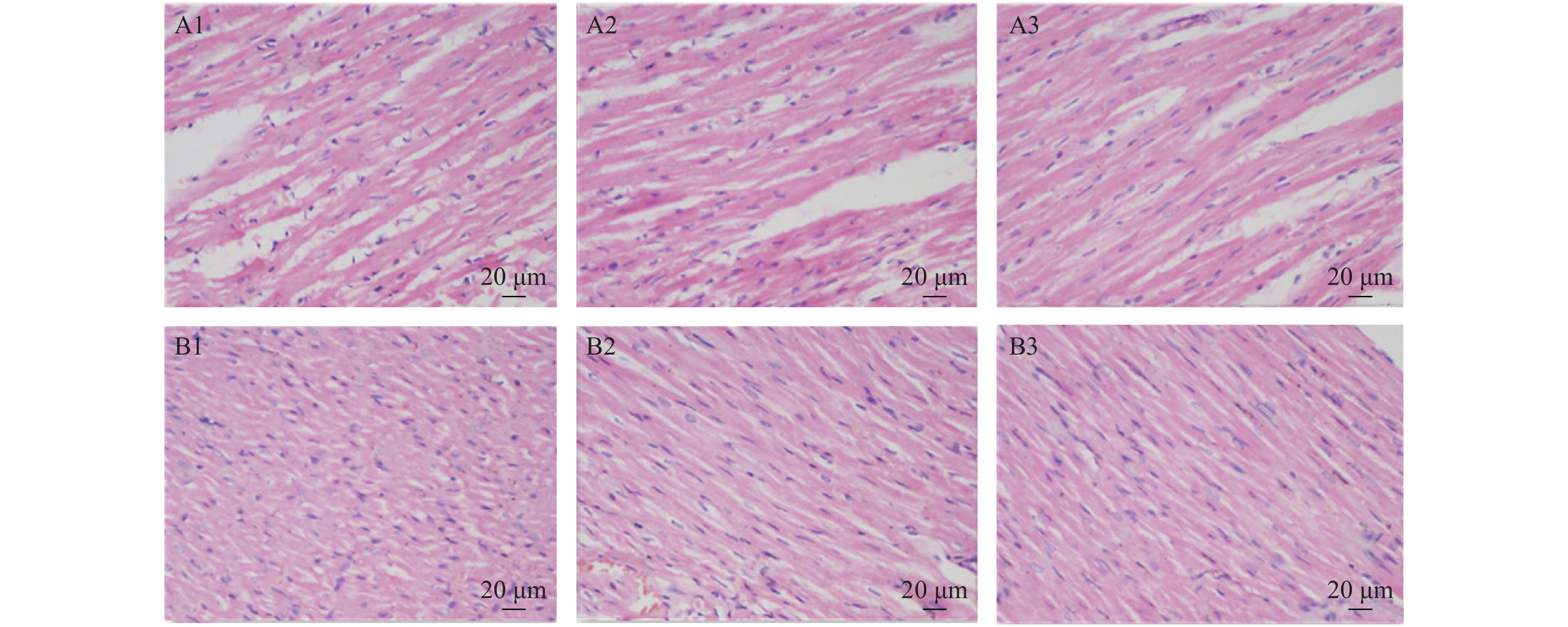
图 6 开胸对照组及再灌注120 min组兔心肌组织病理结果(×400)
A1~A3:为开胸对照组:未经超声辐照、0.5 w/cm2强度辐照后、0.75 w/cm2强度辐照后;B1~B3:为再灌注120 min组:未经超声辐照、0.5 w/cm2强度辐照后、0.75 w/cm2强度辐照后。
Figure 6. Pathological results of rabbit myocardial tissue in the control group after thoracotomy and the group after 120 min of reperfusion (× 400)
表 1 各组兔超声辐照前后视频强度差值[dB,(
$\bar x\pm s$ )]Table 1. Video intensity difference of each group before and after ultrasonic irradiation [dB,(
$\bar x\pm s$ )]分组 n A组 B组 C组 T1(30 min) T2(60 min) T3(120 min) T4(180 min) U1 30 0.15 ± 0.14 5.18 ± 2.83 9.33 ± 1.14 9.32 ± 1.65 10.31 ± 2.75 9.64 ± 1.51 U2 30 0.33 ± 0.04 5.28 ± 1.13 10.99 ± 1.79* 12.05 ± 1.34* 12.34 ± 3.13* 11.61 ± 2.46* 与U1组比较,*P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 不同时段各组兔心肌组织内IL-6水平[pg/mL,(
$\bar x\pm s$ )]Table 2. IL-6 level in myocardial tissue of rabbits in different time periods [pg/mL,(
$\bar x\pm s$ )]分组 n A组 B组 C组 T1(30 min) T2(60 min) T3(120 min) T4(180 min) U0 30 13.01 ± 2.02* 14.85 ± 2.18* 38.76 ± 5.01△▲ 54.29 ± 4.86△▲ 79.88 ± 4.02△▲ 75.25 ± 3.23△▲ U1 30 12.75 ± 2.73* 11.24 ± 2.58* 15.25 ± 2.64△ 28.02 ± 4.74△ 39.25 ± 3.31△ 36.58 ± 2.89△ U2 30 12.00 ± 2.13* 11.01 ± 2.07* 10.47 ± 1.85 25.24 ± 3.51 35.39 ± 2.31 32.36 ± 2.91 与C组比较,*P < 0.05;与U2组比较,△P < 0.05;与U1组比较,▲P < 0.05。
下载: 导出CSV
-
[1] Gurewich V. Thrombolysis. a critical first-line therapy with an unfulfilled potential[J]. Am J Med,2016,129(6):573-575. doi: 10.1016/j.amjmed.2015.11.033 [2] Bedenis R,Lethaby S,Maxwell H,et al. antiplateletagents for preventing thrombosis after peripheral arterial bypass surgery[J]. Cochrane Database Syst Rev,2015(2):CD000535. [3] Al-Lamee R,Davies J,Malik I S. What is the role of coronary angioplasty and stenting in stable angina[J]. BMJ,2016,352(1):i205. [4] Xue J,Ge H,Lin Z,et al. The role of dendritic cells regulated by HMGB1/TLR4 signalling pathway in myocardial ischaemia reperfusion injury[J]. J Cell Mol Med,2019,23(4):2849-2862. doi: 10.1111/jcmm.14192 [5] Lin L,Wu X D,Davey A K,et al. The anti-inflammatory effect of baicalin on hypoxia/reoxygenation and TNF-alpha induced injury in cultural rat cardiomyocytes[J]. Phytother Res,2010,24(3):429-37. doi: 10.1002/ptr.3003 [6] Kosmala W,Przewlocka-Kosmala M,Mazurek W. Proinflammatory cytokines and myocardial viability in patients after acute myocardial infarction[J]. Int J Cardiol,2005,101(3):449-456. doi: 10.1016/j.ijcard.2004.03.067 [7] Wilkowska A,Pikuła M,Rynkiewicza,et al. Increased plasma proinflammatory cytokine concentrations after myocardial infarction and the presence of depression during next 6-months[J]. PsychiatrPol,2015,49(3):455-464. [8] Kleveland O,Kunszt G,Bratlie M,et al. Effect of a single dose of the interleukin-6 receptor antagonist tocilizumab on inflammation and troponin T release in patients with non-ST-elevation myocardial infarction:a double-blind,randomized,placebo-controlled phase 2 trial[J]. Eur Heart J,2016,37(30):2406-2413. doi: 10.1093/eurheartj/ehw171 [9] Wei G,GuanY,Yin Y,et al. anti-inflammatory effect of protocatechuic aldehyde on myocardial ischemia/reperfusion injury in vivo and in vitro[J]. Inflammation,2013,36(3):592-602. doi: 10.1007/s10753-012-9581-z [10] Song S,Shen Z,Chen L,et al. Explorations of high-intensity therapeutic ultrasound and microbubble-mediated gene delivery in mouse liver[J]. Gene Ther,2011,18(10):1006-1014. doi: 10.1038/gt.2011.34 [11] Ritschel Vibeke N,SeljeflotIngebjørg,Arnesen Harald,et al. IL-6 signalling in patients with acute ST-elevation myocardial infarction[J]. Results Immunol,2014,4(1):8-13. [12] 邹吉丽,尹照萍,张利群,等. 大鼠心肌缺血再灌注早期心肌及血清中IL-6、TNF-α的表达[J]. 中国医科大学学报,2013,42(9):830-833. doi: 10.3969/j.issn.0258-4646.2013.09.016 [13] Wu H,Xie D,Yang Y,et al. Ultrasound-targeted microbubble destruction-mediated miR-206 overexpression promotes apoptosis and inhibits metastasis of hepatocellular carcinoma cells via targeting PPIB[J]. Technol Cancer Res Treat,2020,19. [14] Sun W,Zhao P,ZhouY,et al. Ultrasound targeted microbubble destruction assisted exosomal delivery of miR-21 protects the heart from chemotherapy associated cardiotoxicity[J]. Biochem Biophys Res Commun,2020,532(1):60-67. doi: 10.1016/j.bbrc.2020.05.044 [15] 宋立秋,杜国庆,郑雅朦,等. 超声靶向微泡爆破介导GDF11基因促老年小鼠缺血心肌保护[J]. 中国循环杂志,2017,32(z1):203. doi: 10.3969/j.issn.1000-3614.2017.z1.521 [16] Kukielka G L,Youker K A,Hawkins H K,et al. Regulation of ICAM-1 and IL-6 in myocardial ischemia:Effect of Reperfusion[J]. Ann N Y Acad Sci,1994,723(1):258-70. doi: 10.1111/j.1749-6632.1994.tb36732.x [17] 孙月,朱桂敏,杨莉红,等. 超声微泡破坏技术不同辐照强度对兔心肌的生物学效应研究[J]. 中国超声医学杂志,2019,35(2):171-174. doi: 10.3969/j.issn.1002-0101.2019.02.026 -





 点击查看大图
点击查看大图
计量
- 文章访问数: 2911
- HTML全文浏览量: 2157
- PDF下载量: 28
- 被引次数: 0
