

Application of Coronary Computed Tomography Angiography in Overweight Patients: Comparison of Automated Tube Voltage Selection Versus 100 kVp Tube Voltage
-
摘要:
目的 在自动管电压选择(automated tube voltage selection,APSCM)与定向100 KVp管电压两种情况下,比较超重患者冠状动脉计算机体层血管造影(coronary computed tomography angiography,CCTA)的图像质量和辐射剂量。 方法 选取115位体重指数(BMI)在25~30 kg / m2 之间,并且体重低于90 kg的患者在第二代双源CT扫描仪上进行CCTA检查,所有检查均采用前瞻性心电门控及大螺距(3.4)模式。所有患者被随机分为A、B两组:A组75例,采用APSCM技术进行检查;B组40例,接受固定100 kVp管电压检查。测量CT衰减和图像噪声,并计算信噪比(signal-to-noise ratio,SNR)和对比噪声比(contrast-to-noise ratio,CNR)。对两组图像质量及辐射剂量进行比较。 结果 A组中,1例(1.3%)、51例(68%)和23例(30.7%)患者的管电压自动选择为80 kVp、100 kVp、120 kVp,平均CT衰减和图像噪声显著低于B组(P < 0.001)。A组的平均CNR高于B组,平均SNR较低( P < 0.05)。两组的主观图像质量得分无显著差异( P > 0.05),B组的辐射剂量比A组低22.2%( P = 0.004)。 结论 对于BMI高于25 kg / m2、低于30 kg / m2,且体重低于90 kg的患者,与使用APSCM的CCTA相比,100 kVp CCTA可以降低辐射剂量而不影响图像质量。 Abstract:Objective To compare the image quality and radiation dose of automated tube voltage selection (APSCM) and 100 kVp coronary computed tomography angiography (CCTA) in overweight patients. Methods A total of 115 patients with a body mass index (BMI) higher than 25 kg/m2 and less than 30 kg/m2 and body weight lower than 90 kg underwent high-pitch prospectively ECG-triggered CCTA on a second-generation dual-source CT scanner. All patients were classified into two groups: Group A, 75 patients were examined with APSCM; Group B, 40 patients with a fixed tube voltage of 100 kVp. The attenuation and image noise were measured and signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were calculated. Image quality was evaluated and radiation dose was recorded. Results In Group A, 80 kVp, 100 kVp and 120 kVp were automatically selected in 1 (1.3%), 51 (68.0%) and 23 (30.7%) patients, respectively. The mean CT attenuations and image noise in APSCM group were significantly lower than those in Group B (all P < 0.001). Group A showed a higher mean CNR but a lower mean SNR (all P < 0.05) than Group B. The subjective image quality scores have no significant difference between the two groups (all P < 0.05). The radiation dose in Group B was 22.2% lower than in Group A ( P = 0.004). Conclusion In patients with BMI higher than 25 kg/m2 and less than 30 kg/m2, 100 kVp CCTA allows lower radiation dose without compromising image quality when compared with CCTA using APSCM. -
Key words:
- Computed tomography /
- Angiography /
- Coronary artery /
- Tube potential /
- Radiation dose
-

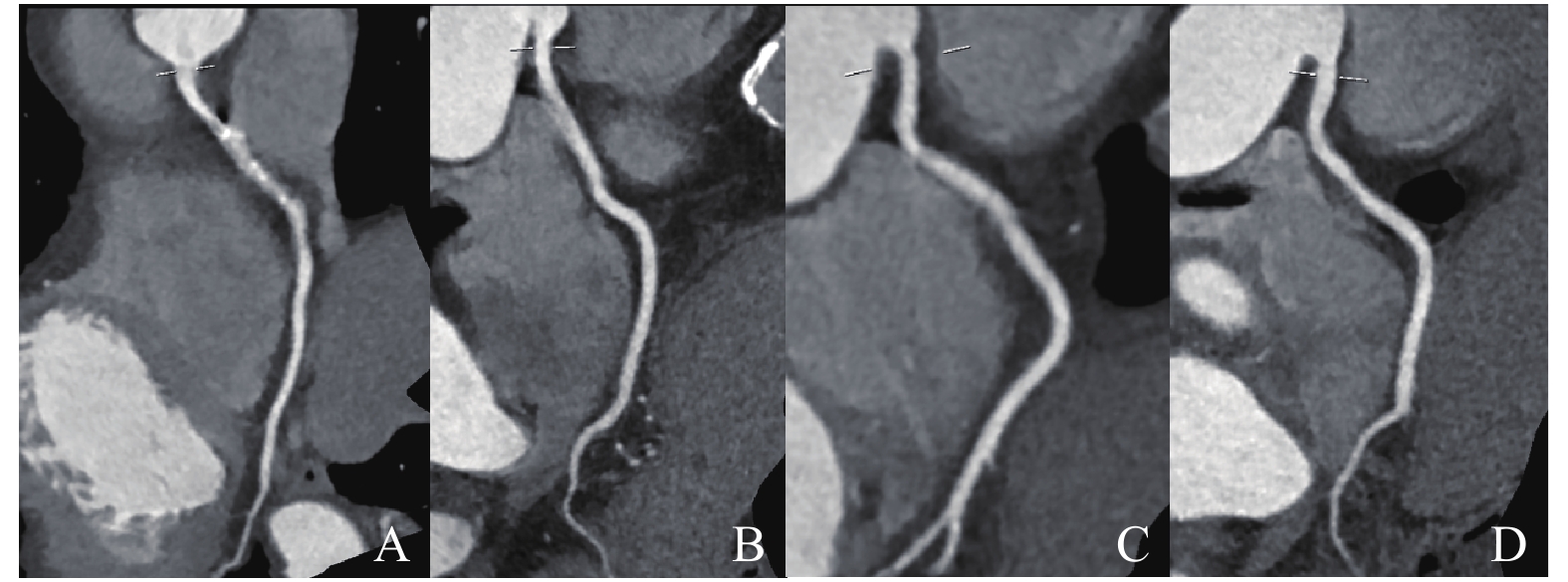
图 1 100 kVp CCTA组和APSCM CCTA组的曲面重组(CPR)图像质量对比
A:100 kVp CCTA组;B:APSCM CCTA组;C:100 kVp CCTA组;D:APSCM CCTA组。
Figure 1. Comparison of curved planar reformations (CPR)image quality between 100 kVP CCTA group and APSCM CCTA group

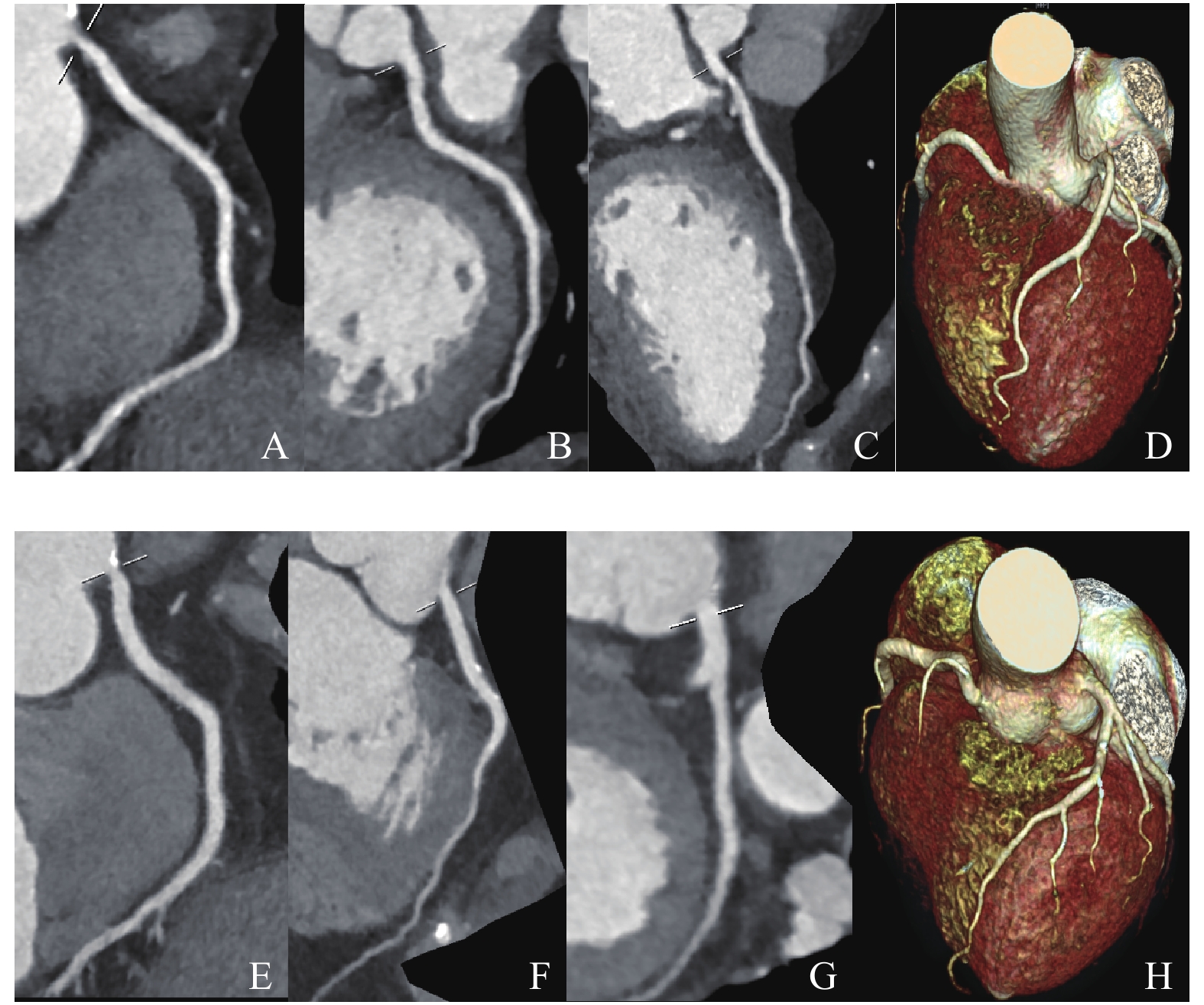
图 2 100 kVp组和APSCM组的CT图像示例
A:100 kVp CCTA组;B:100 kVp CCTA组;C:100 kVp CCTA组;D:100 kVp CCTA组;E:APSCM CCTA组;F:APSCM CCTA组;G:APSCM CCTA组;H:APSCM CCTA组。
Figure 2. Examples of CT images from the 100 kVp group and the APSCM group
表 1 两组CCTA的客观图像质量比较(
$\bar x \pm s $ )Table 1. Objective image quality evaluation of CCTA in the two groups (
$\bar x \pm s $ )位置 APSCM组 100 kVp组 t P RCA CT(HU) 426.0 ± 95.0 504.0 ± 71.0 −4.527 < 0.001* SNR 28.2 ± 16.4 33.7 ± 18.0 −1.761 0.038* CNR 31.4 ± 5.5 27.2 ± 5.8 3.841 < 0.001* LMA CT(HU) 431.0 ± 105.0 505.0 ± 83.0 −3.915 < 0.001* SNR 36.0 ± 21.0 43.4 ± 23.6 −2.282 0.005* CNR 31.5 ± 5.3 27.3 ± 6.0 3.924 < 0.001* LAD CT(HU) 422.0 ± 88.0 488.0 ± 88.0 −3.842 < 0.001* SNR 31.1 ± 31.0 38.7 ± 30.3 −1.660 0.053* CNR 31.1 ± 4.6 26.5 ± 6.0 4.631 < 0.001* LCX CT(HU) 428.0 ± 95.0 501.0 ± 97.0 −3.895 < 0.001* SNR 30.5 ± 24.8 38.3 ± 15.4 −1.705 0.001* CNR 31.6 ± 5.2 27.3 ± 7.3 3.652 0.002* 平均 CT(HU) 426.0 ± 88.0 500.0 ± 78.0 −4.432 < 0.001* SNR 31.4 ± 15.2 39.8 ± 13.1 −2.976 0.004* CNR 31.4 ± 4.5 27.0 ± 6.1 4.349 < 0.001* 图像噪声(HU) 17.0 ± 3.0 22.0 ± 4.0 −8.410 < 0.001* 注:*P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 两组冠状动脉的主观图像质量评分比较(
$\bar x \pm s $ )Table 2. Subjective image quality scores of coronary arteries in the two groups (
$\bar x \pm s $ )血管 100 kVp组 80 kVp组 U P RCA 3.5 ± 0.8 3.3 ± 1.0 1396.50 0.488 LMA 3.9 ± 0.3 3.9 ± 0.3 1450.00 0.528 LAD 3.5 ± 0.7 3.3 ± 0.8 1287.50 0.162 LCX 3.4 ± 0.7 3.1 ± 0.8 1242.00 0.096 平均 3.6 ± 0.4 3.4 ± 0.6 1277.00 0.181
下载: 导出CSV
表 3 两组辐射剂量比较(
$ \bar x \pm s$ )Table 3. Radiation dose comparison between the two CCTA groups (
$\bar x \pm s $ )参数 APSCM组 100 kVp组 t P CTDI (mGy) 4.3 ± 1.6 3.3 ± 0.3 3.909 0.046* DLP (mGy×cm) 74.5 ± 27.6 58.3 ± 7.2 3.651 0.040* ED (mSv) 1.0 ± 0.4 0.8 ± 0.1 3.651 0.040* SSDE (mGy) 5.4 ± 1.8 4.2 ± 0.4 3.909 0.004* 注:*P < 0.05;CTDIvol = CT容积剂量指数;DLP = 剂量长度乘积;ED = 有效剂量;SSDE = 体型特异性剂量估计。
下载: 导出CSV
-
[1] BamiK,Premaratne M,Lamba J,et al. Appropriate use criteria for cardiac computed tomography:impact on diagnostic utility[J]. Journal of Computer Assisted Tomography,2017,41(5):1. [2] Richards C E,Dorman S,John P,et al. Low-radiation and high image quality coronary computed tomography angiography in "real-world" unselected patients[J]. World J Radiol,2018,10(10):135-142. doi: 10.4329/wjr.v10.i10.135 [3] Bosch de Basea M,Pearce M S,Kesminiene A,et al. EPI-CT:design,challenges and epidemiological methods of an international study on cancer risk after paediatric and young adult CT[J]. Journal of Radiological Protection,2015,35(3):611-628. doi: 10.1088/0952-4746/35/3/611 [4] Mccollough C H. Computed tomography technology-and dose-in the 21st century[J]. Health Physics,2019,116(2):157-162. doi: 10.1097/HP.0000000000000997 [5] Abbara S,Blanke P,Maroules C D,et al. SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography:A report of the society of Cardiovascular Computed Tomography Guidelines Committee:Endorsed by the North American Society for Cardiovascular Imaging (NASCI)[J]. J Cardiovasc Comput Tomogr,2016,10(6):435-449. [6] Hecht H S,Cronin P,Blaha M J,et al. 2016 SCCT/STR guidelines for coronary artery calcium scoring of noncontrast noncardiac chest CT scans:A report of the Society of Cardiovascular Computed Tomography and Society of Thoracic Radiology[J]. J Cardiovasc Comput Tomogr,2017,11(1):74-84. [7] Den Harder A M,Willemink M J,de Jong P A,et al. New horizons in cardiac CT[J]. Clin Radiol,2016,71(8):758-767. doi: 10.1016/j.crad.2016.01.022 [8] Lee H S,Suh Y J,Han K,et al. Effectiveness of automatic tube potential selection with tube current modulation in coronary CT angiography for obese patients:Comparison with a body mass index-based protocol using the propensity score matching method[J]. PLoS One,2018,3(1):e0190584. [9] Zhao P,Hou Y,Liu Q,et al. Radiation dose reduction in cardiovascular CT angiography with iterative reconstruction (AIDR 3D) in a swine model:A model of paediatric cardiac imaging[J]. Clin Radiol,2016,71(7):716. [10] Örgel A,Bier G,Hennersdorf F,et al. Image quality of CT angiography of supra-aortic arteries:comparison between advanced modelled iterative reconstruction (ADMIRE),sinogram affirmed iterative reconstruction (SAFIRE) and filtered back projection (FBP) in one patients' group[J]. Clin Neuroradiol,2020,30(1):101-107. doi: 10.1007/s00062-018-0740-y [11] Andreini D,Pontone G,Mushtaq S,et al. Image quality and radiation dose of coronary CT angiography performed with whole-heart coverage CT scanner with intra-cycle motion correction algorithm in patients with atrial fibrillation[J]. Eur Radiol,2018,28(4):1383-1392. doi: 10.1007/s00330-017-5131-2 [12] Mousavi Gazafroudi S S,Tavakkoli M B,Moradi M,et al. Coronary CT angiography by modifying tube voltage and contrast medium concentration:Evaluation of image quality and radiation dose[J]. Echocardiography,2019,36(7):1391-1396. doi: 10.1111/echo.14410 [13] Atwi N E,Smith D L,Flores C D,et al. Dual-energy CT in the obese:a preliminary retrospective review to evaluate quality and feasibility of the single-source dual-detector implementation[J]. AbdomRadiol (NY),2019,44(2):783-789. [14] Symons R,Choi Y,Cork T E,et al. Optimized energy of spectral coronary CT angiography for coronary plaque detection and quantification[J]. J Cardiovasc Comput Tomogr,2018,12(2):108-114. [15] Austen W G,Edwards J E,Frye R L,et al. A reporting system on patients evaluated for coronary artery disease:report of the ad hoc committee for grading of coronary artery disease,council on cardiovascular surgery,American Heart Association[J]. Circulation,1975,51(Suppl4):5-40. [16] Lee S H,Cho J H,Kim H E,et al. Effect of coronary artery calcification score by lifestyle and correlation with coronary artery stenosis by multidetector computed tomography[J]. J Comput Assist Tomogr,2017,41(2):236-241. doi: 10.1097/RCT.0000000000000497 [17] Dorbala S,Blankstein R,Skali H,et al. Approaches to reducing radiation dose from radionuclide myocardial perfusion imaging[J]. J Nucl Med,2015,56(4):592-599. doi: 10.2967/jnumed.112.115097 [18] Kawashima H,Ichikawa K,Hanaoka S,et al. Relationship between size-specific dose estimates and image quality in computed tomography depending on patient size[J]. J Appl Clin Med Phys,2018,19(4):246-251. doi: 10.1002/acm2.12340 [19] Lee J W,Kim C W,Lee H C,et al. High-definition computed tomography for coronary artery stents:image quality and radiation doses for low voltage (100 kVp) and standard voltage (120 kVp) ECG-triggered scanning[J]. Int J Cardiovasc Imaging,2015,31(Suppl1):39-49. [20] Lee H S,Suh Y J,Han K,et al. Effectiveness of automatic tube potential selection with tube current modulation in coronary CT angiography for obese patients:Comparison with a body mass index-based protocol using the propensity score matching method[J]. PLoS One,2018,13(1):e0190584. doi: 10.1371/journal.pone.0190584 [21] Li M,Feng S,Wu N,et al. Scout-based automated tube potential selection technique (kV assist) in enhanced chest computed tomography:Effects on radiation exposure and image quality[J]. J Comput Assist Tomogr,2017,41(3):442-445. doi: 10.1097/RCT.0000000000000523 -







 点击查看大图
点击查看大图
计量
- 文章访问数: 2648
- HTML全文浏览量: 1966
- PDF下载量: 43
- 被引次数: 0
