

Clinical Investigation of Vitamin D and Calcium Supplement’ Effect on the Occurrence of Cardiovascular and Cerebrovascular Diseases in POP Patients
-
摘要:
目的 探究维生素D(vitamin D,VD)及钙剂(calcium,Ca)补充对高血压或冠心病POP人群心脑血管类疾病发生的影响。 方法 将2018年10月至2019年9月在溧阳市人民医院心血管内科诊断为高血压伴原发性骨质疏松症(primary osteoporosis,POP)或冠心病伴POP并符合纳入标准的317例患者纳入研究,分为高血压组224例、冠心病组93例;并根据VD缺乏程度各自分为VD缺乏组(25(OH)D≤20 ng/mL)和极度缺乏组(25(OH)D≤10 ng/mL)。予VD缺乏组碳酸钙D3(钙尔奇D)1片,每天1次;予VD极度缺乏组碳酸钙D3(钙尔奇D)2片,每天1次。连续补充18个月。期间嘱患者记录心绞痛(包括心肌梗死)、动脉粥样硬化(除冠脉外新发)、下肢静脉血栓、脑梗发生并迫使其就医的发作次数和就医时的25(OH)D和血Ca水平,并记录各组发生心脑血管类疾病发生和未发生的总人数。比较各组内以上指标的差异。 结果 POP高血压组:VD极度缺乏组(19.0%)比VD缺乏组(7.5%)发生心脑血管类疾病的比例较高,P = 0.018;2组VD及Ca呈现显著正相关,P < 0.001。与VD缺乏组比较,VD极度缺乏组发生心绞痛时的血Ca及VD水平均较高,P < 0.05。POP冠心病组:VD极度缺乏组(86.2%)比VD缺乏组(62.7%)发生心血管类疾病的比例较高,P = 0.030;2组VD及Ca呈现显著的正相关,P < 0.001。与VD缺乏组比较,VD极度缺乏组发生心绞痛时的血Ca及VD水平均较高,P < 0.05和P < 0.01;发生动脉粥样硬化时血Ca水平较高,P < 0.05,而VD有升高趋势。 结论 对于高血压伴POP并VD极度缺乏的患者来说,适度增加VD并减少Ca补充较为适宜;而对于对应的冠心病患者来说,应当谨慎(一定程度减少)补充VD及Ca剂。 Abstract:Objective To investigate the vitamin D (VD) and calcium supplement’effect on the occurrence of cardiovascular and cerebrovascular diseases in Primary osteoporosis (POP) patients accompanied with hypertension or coronary heart disease. Methods From October 2018 to September 2019, the 317 cases diagnosed as hypertension or coronary heart disease accompanied with primary osteoporosis diagnosis and complying with inclusion criteria in Cardiovascular department of Liyang Municipal People’s Hospital were recruited, divided into hypertension and coronary heart disease groups, with 224 and 93 participants in each group. Then participants in each group were again divided into VD deficiency (25(OH)D≤20 ng/mL) and severe deficiency (25(OH)D≤10 ng/mL) groups, treated with one Calcium carbonate D3 pill and two pills per day, respectively. Treatment lasts for 18 months, during which the participants should recorded the occurrence times of angina pectoris (including myocardial infarction), atherosclerosis (newly occurrence except for coronary), lower limbs’ venous thrombosis and cerebral infarction, which forced the participant to turn to hospital, as well as the VD and Ca concentrations examined during the periods. The occurrence and non-occurrence proportion and VD and Ca concentrations between the two groups among the corresponding group were compared. Results POP hypertension groups: The incidents proportion of heart, cerebral and vessels diseases in VD severe deficiency group (19.0%) was higher than that (7.5%) of VD deficiency group, P = 0.018. There was an obviously positive correlation between VD and Ca, P < 0.001. Compared with VD deficiency group, the VD and Ca levels of VD severe deficiency group at the occurrence of angina pectoris were higher, P < 0.05. POP coronary heart disease groups: The incidents proportion of heart, cerebral and vessels diseases in VD severe deficiency group (86.2%) was higher than that (62.7%) of VD deficiency group, P = 0.030. There was an obviously positive correlation between VD and Ca, P < 0.001. Compared with VD deficiency group, the VD and Ca levels of VD severe deficiency group at the occurrence of angina pectoris were higher, P < 0.05 and P < 0.01, respectively. When suffering from atherosclerosis, the Ca level of participants in VD severe deficiency group was higher than that in VD deficiency group, P < 0.05, with a increasing trend of VD level. Conclusion Properly added VD and decreased Ca supplement might be suitable for hypertension accompanied with POP patients with VD severe deficiency. For coronary heart disease accompanied with POP patients with VD severe deficiency, decreased VD and Ca supplement may be more fit. -
Key words:
- Vitamin D /
- Calcium /
- Primary osteoporosis /
- Cardiovascular diseases
-
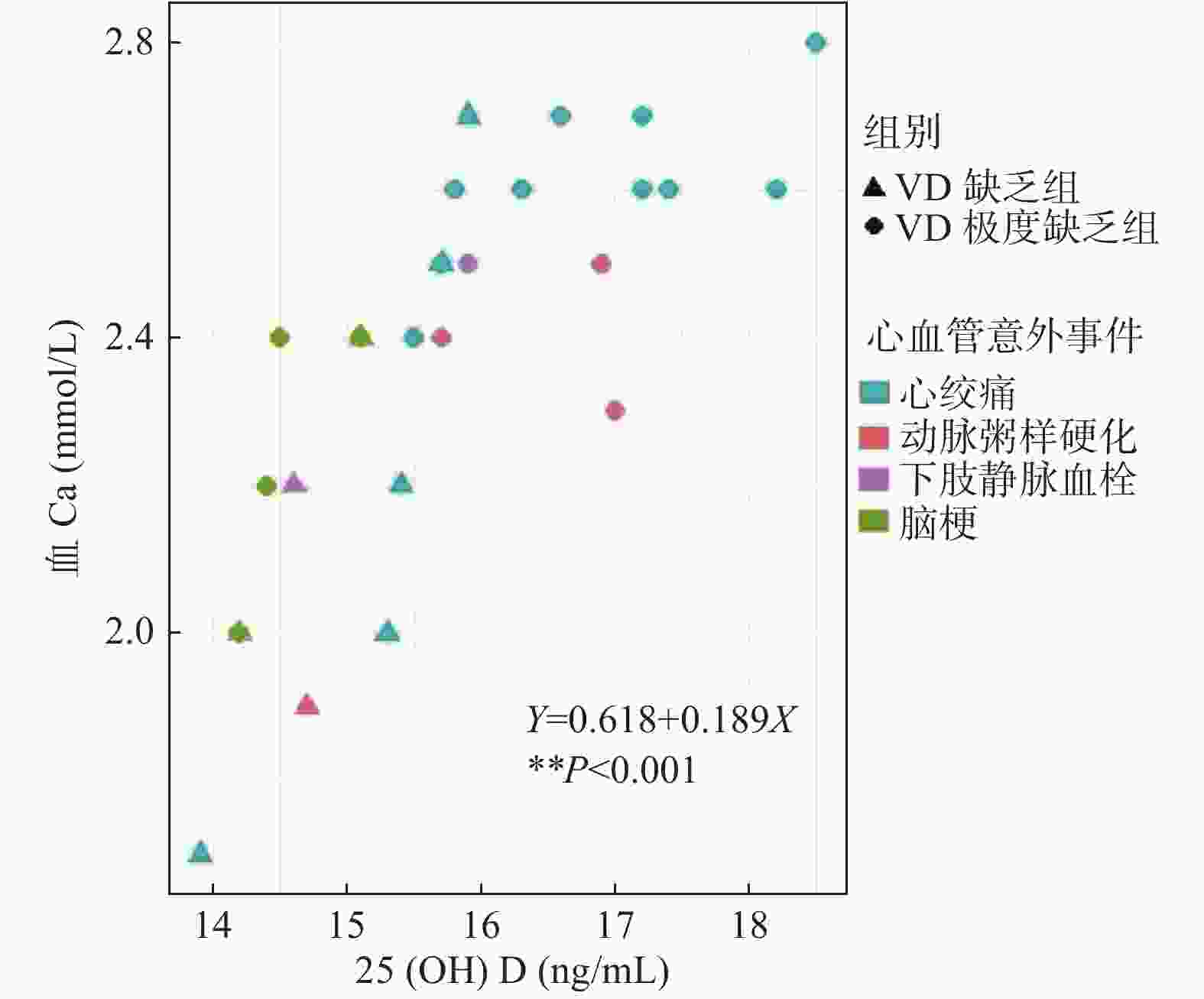
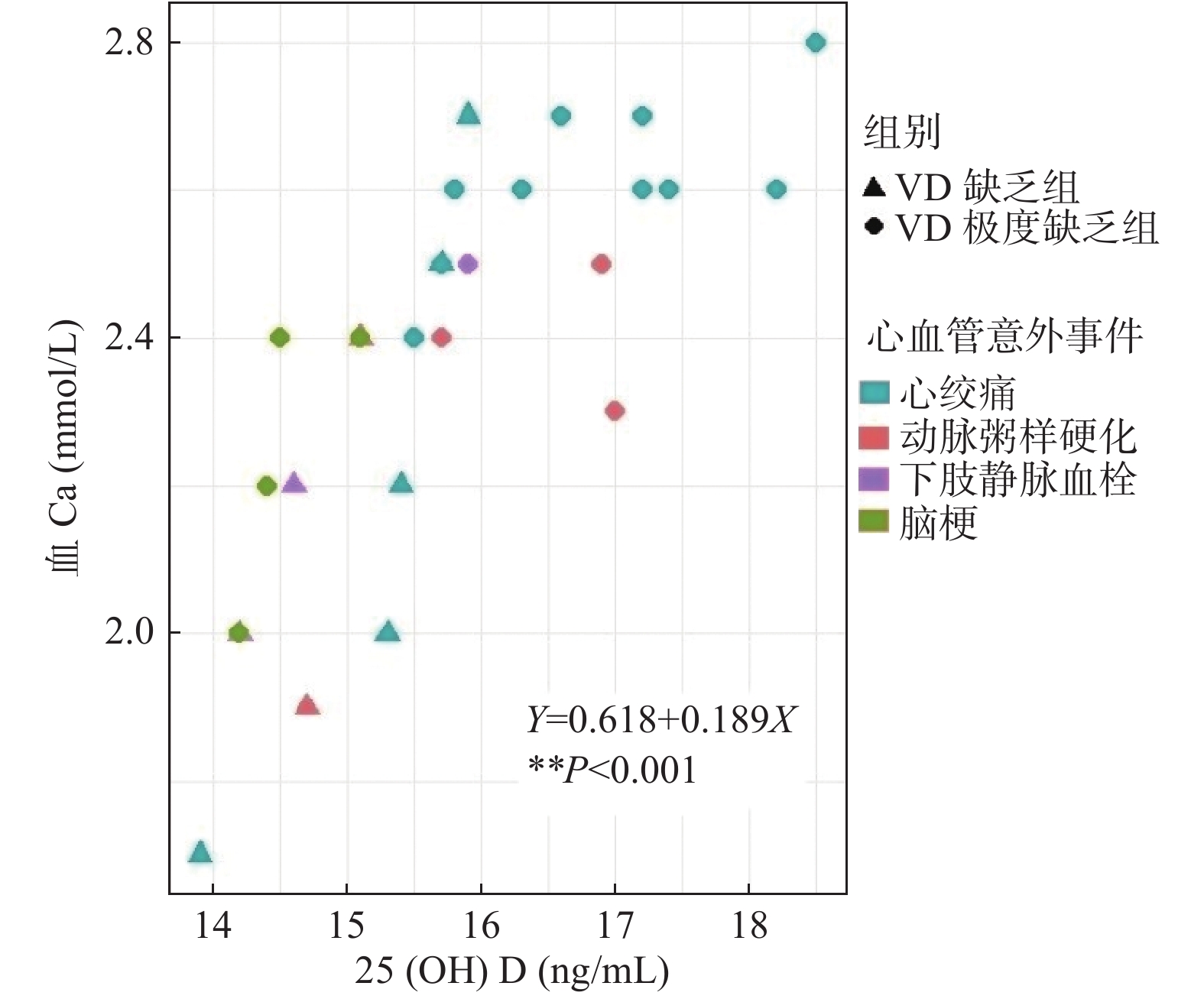
图 1 高血压组发生心脑血管疾病时 VD 对血 Ca 水平的影响
Figure 1. The serum calcium and VD levels of participants in the two groups of hypertension group at the occurrence of heart,cerebral and vessel diseases
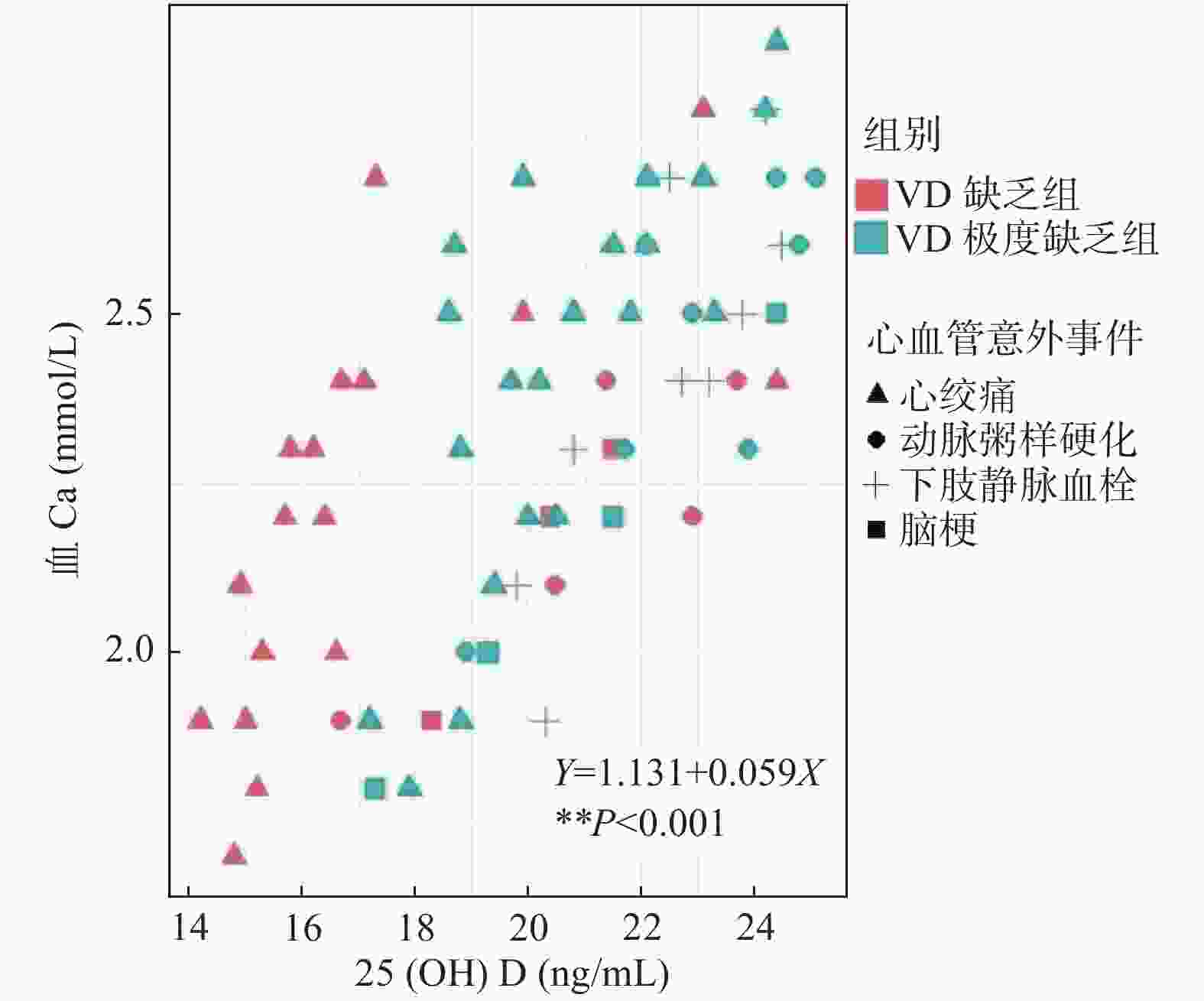
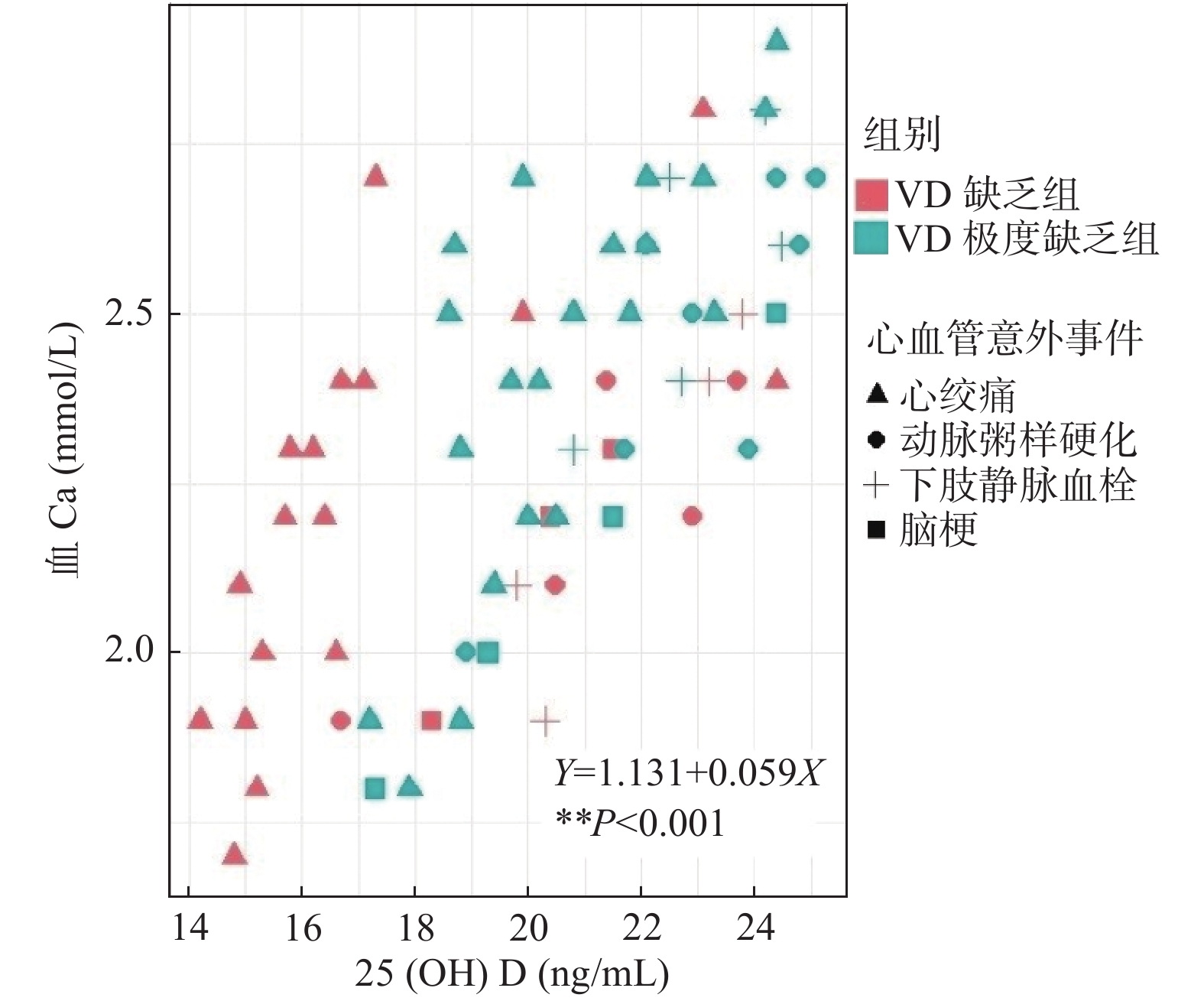
图 2 冠心病组发生心脑血管疾病时VD对血Ca水平的影响
Figure 2. The effects of VD on serum calcium levels in the coronary heart disease group at the occurrences of heart,cerebral and vessel diseases
表 1 高血压组、冠心病组中VD缺乏及VD极度缺乏组一般资料比较(
$\bar x \pm s $ )Table 1. The common resource comparison between the two groups thus VD deficiency and VD severe deficiency groups of the hypertension group and coronary heart disease group (
$\bar x \pm s $ )项目 高血压组(224例) 冠心病组(93例) VD缺乏组122例 VD极度缺乏组102例 VD缺乏组52例 VD极度缺乏组41例 年龄(岁) 63.2 ± 8.9 64.5 ± 9.2 63.5 ± 8.8 63.7 ± 9.5 性别(男/女) 21/31 17/24 52/70 39/63 BMI(kg/m2) 23.5 ± 1.7 23.8 ± 1.8 23.2 ± 1.7 22.6 ± 1.8* 病程(岁) 4.2 ± 2.1 5.1 ± 2.2* 3.1 ± 1.7 3.5 ± 1.5 心功能分级#(n) 正常45;Ⅰ级5;
Ⅱ级2正常:38;Ⅰ级3 Ⅰ级75;Ⅱ级34;
Ⅲ级11;Ⅳ级2Ⅰ级66;Ⅱ级28
Ⅲ级7;Ⅳ级125(OH)D(ng/mL) 14.7 ± 3.9 7.2 ± 2.5** 15.2 ± 4.0 7.3 ± 2.6** 血Ca(mmol/L) 2.1 ± 1.2 1.9 ± 1.0 2.2 ± 1.2 1.9 ± 1.0* 白蛋白(g/L) 45.3 ± 7.3 42.5 ± 7.6 45.7 ± 8.1 43.2 ± 7.9* 注:#入组时检测血压并参照《中国高血压病防治指南2010》[6](2010年修订版)获得高血压分级;根据纽约心脏学会(NYHA)[7]制订的心功能分级标准评定心功能;与同组VD缺乏组比较,*P < 0.05,**P < 0.01。  下载: 导出CSV
下载: 导出CSV
表 2 随访期间高血压组中VD缺乏及VD极度缺乏组发生心脑血管类疾病次数比较[n(%)]
Table 2. The occurrence times comparison of heart,cerebral and vessel diseases between the two groups thus VD deficiency and VD severe deficiency groups of the hypertension group during the follow-up period [n(%)]
组别 n 心血管意外事件(n) 发生
(人)未发生
(人)χ2 P 心绞痛
(次)动脉粥样
硬化(次)下肢静脉
血栓(次)脑梗
(次)VD缺乏组 107 6 2 2 0 8(7.5) 99(92.5) 5.557 0.018 VD极度缺乏组 79 11 3 1 4 15(19.0) 64(81.0) 采用皮尔逊χ2检验。
下载: 导出CSV
表 3 发生心脑血管类疾病时高血压组中VD缺乏及VD极度缺乏组血Ca及VD水平比较
Table 3. The serum calcium and VD levels comparison between the two groups thus VD deficiency and VD severe deficiency groups of the hypertension group at the occurrences of heart,cerebral and vessel diseases
指标 心绞痛(次) 动脉粥样硬化(次) 下肢静脉血栓(次) VD缺乏组
(6)VD极度缺乏组
(11)VD缺乏组
(2)VD极度缺乏组(3) VD缺乏组(2) VD极度缺乏组(1) 血Ca(ng/mL) 2.1(1.7,2.5) 2.6(2.5,2.7)* 2.23# 2.4# 2.1# 2.5# VD(mmol/L) 15.4(13.9,15.8) 16.6(15.8,17.4)* 14.9# 16.53# 14.4# 15.0# 注:与VD缺乏组比较,*P < 0.05。#由于样本较少,采用均数或者具体值表示。
下载: 导出CSV
表 4 随访期间冠心病组中VD缺乏及VD极度缺乏组发生心脑血管类疾病次数比较[n(%)]
Table 4. The occurrence times comparison of heart,cerebral and vessel diseases between the two groups thus VD deficiency and VD severe deficiency groups of the coronary heart disease group during the follow-up period [n(%)]
组别 n 心血管意外事件(n) 发生(例) 未发生(例) χ2 P 心绞痛
(次)动脉粥样
硬化(次)下肢静脉
血栓(次)脑梗
(次)VD缺乏组 43 17 6 4 3 27(62.7) 16(37.1) 4.734 0.030 VD极度缺乏组 29 21 8 5 4 25(86.2) 4(13.8) 采用皮尔逊χ2检验。
下载: 导出CSV
表 5 发生心脑血管类疾病时冠心病组中VD缺乏及VD极度缺乏组血Ca水及VD水平比较
Table 5. The serum calcium and VD levels comparison between the two groups thus VD deficiency and VD severe deficiency groups of the coronary heart disease group at the occurrences of heart,cerebral and vessel diseases
指标 心绞痛 动脉粥样硬化(次) 下肢静脉血栓(次) 脑梗 VD缺乏组
(n = 17)VD极度
缺乏组(n = 21)VD缺乏组
(n = 6)VD极度
缺乏组(n = 8)VD缺乏组
(n = 4)VD极度
缺乏组(n = 5)VD缺乏组
(n = 3)VD极度
缺乏组(n = 4)血Ca(ng/mL) 2.2(1.9,2.4) 2.5*(2.2,2.7) 2.1(1.9,2.4) 2.5*(2.3,2.7) 2.3(2.0,2.5) 2.6(2.4,2.8) 2.1# 2.6(2.4,2.8) VD(mmol/L) 16.2(15.1,17.2) 20.3**(18.8,22.1) 20.9(17.2,23.1) 23.4(21.8,24.7) 21.8(19.9,23.6) 23.0(21.7,24.4) 20.0# 20.6(17.8,23.6) 与VD缺乏组比较,*P < 0.05;#采用均数表示。
下载: 导出CSV
-
[1] 中华医学会骨质疏松和骨矿盐疾病分会. 原发性骨质疏松症诊疗指南(2017)[J]. 中国骨质疏松杂志,2019,25(3):281-308. doi: 10.3969/j.issn.1006-7108.2019.03.001 [2] Weaver C M,Alexander D D,Boushey C J,et al. Calcium plus vitamin D supplementation and risk of fractures:an updated meta-analysis from the National Osteoporosis Foundation[J]. Osteoporos Int,2016,27(1):367-376. doi: 10.1007/s00198-015-3386-5 [3] Bolland M J,Barber P A,Doughty R N,et al. Vascular events in healthy older women receiving calcium supplementation:randomised controlled trial[J]. BMJ,2008,336(7638):262-266. doi: 10.1136/bmj.39440.525752.BE [4] Wang L,Manson J E,Song Y,et al. Systematic review:Vitamin D and calcium supplementation in prevention of cardiovascular events[J]. Ann Intern Med,2010,152(5):315-323. doi: 10.7326/0003-4819-152-5-201003020-00010 [5] Li C,Chen P,Duan X,et al. Bioavailable 25(OH)D but Not Total 25(OH)D Is an Independent Determinant for Bone Mineral Density in Chinese Postmenopausal Women[J]. E Bio Medicine,2017,15(10):184-192. [6] 中国高血压防治指南修定委员会. 中国高血压防治指南2010[J]. 中华心血管病杂志,2011,39(7):579-616. [7] Giustino G,Lindenfeld J,Abraham W T,et al. NYHA Functional Classification and Outcomes After Transcatheter Mitral Valve Repair in Heart Failure:The COAPT Trial[J]. JACC Cardiovasc Interv,2020,13(20):2317-2328. doi: 10.1016/j.jcin.2020.06.058 [8] 赵慧,刘红,王冬雪,等. 高密度脂蛋白组分中血浆淀粉样蛋白A与载脂蛋白A-Ⅰ比值在冠心病诊断中的价值[J]. 中国循环杂志,2015,30(3):211-215. doi: 10.3969/j.issn.1000-3614.2015.03.004 [9] 中华医学会骨质疏松和骨矿盐疾病分会. 原发性骨质疏松症诊疗指南(2017)[J]. 中华骨质疏松和骨矿盐疾病杂志,2017,10(5):413-443. doi: 10.3969/j.issn.1674-2591.2017.05.002 [10] 中华医学会骨质疏松和骨矿盐疾病分会. 原发性骨质疏松症诊疗指南(2017)[J]. 中国全科医学,2017,20(32):3963-3982. doi: 10.3969/j.issn.1007-9572.2017.00.118 [11] 中华医学会心血管病学分会中华心血管病杂志编辑委员会. 不稳定性心绞痛和非 ST 段抬高心肌梗死诊断与治疗指南[J]. 中华心血管病杂志,2007,35:295-304. [12] 中华医学会心血管病分会,中华心血管杂志编辑委员会. 慢性稳定性心绞痛诊断与治疗指南[J]. 中华心血管病杂志,2007,35(3):195-206. [13] Lian X L,Zhang Y P,Li X,et al. Exploration on the relationship between the elderly osteoporosis and cardiovascular disease risk factors[J]. Eur Rev Med Pharmacol Sci,2017,21(19):4386-4390. [14] Chen Q,Zhang Y,Ding D,et al. Associations between serum calcium,phosphorus and mortality among patients with coronary heart disease[J]. Eur J Nutr,2018,57(7):2457-2467. doi: 10.1007/s00394-017-1518-8 [15] Aslam A,Ahmad J,Baghdadi M A,et al. Chemopreventive effects of vitamin D and its analogue,paricalcitol,in combination with 5-fluorouracil against colorectal cancer:The role of calcium signalling molecules[J]. Biochim Biophys Acta Mol Basis Dis,2021,1867(3):166040. doi: 10.1016/j.bbadis.2020.166040 [16] Liu Y,Peng W,Li Y,et al. Vitamin D Deficiency Harms Patients with Coronary Heart Disease by Enhancing Inflammation[J]. Med Sci Monit,2018,24:9376-9384. doi: 10.12659/MSM.911615 [17] Cakal S,Çakal B,Karaca O. Association of vitamin D deficiency with arterial stiffness in newly diagnosed hypertension[J]. Blood Press Monit,2021,26(2):113-117. doi: 10.1097/MBP.0000000000000497 -



 点击查看大图
点击查看大图
计量
- 文章访问数: 3821
- HTML全文浏览量: 2467
- PDF下载量: 26
- 被引次数: 0
