

Clinical Characteristics of Acute Ischemic Stroke Based on Multiple Imaging Evaluation
-
摘要:
目的 分析联合多重影像评估的急性缺血性脑卒中临床特征。 方法 联合多重影像评估首都医科大学宣武医院2014年1月至2018年12月收治的8441例急性缺血性脑卒中的发生占比、动脉血管病理改变、梗塞责任血管以及梗死机制。 结果 (1)男性发生占比高于女性(74.7% vs 25.3%; P < 0.001)而发病年龄则小于女性[(58.83±12.56)岁 vs (63.37±13.27)岁; P < 0.0001],50~69岁为急性缺血性脑卒中发病高峰期(57.87%);(2)高血压、糖尿病和高脂血症为急性缺血性脑卒中主要危险因素,高血压为最常见危险因素(28.65%);(3)动脉粥样硬化(62.9%)是急性缺血性脑卒中动脉管壁最主要病理改变,也是最常见病因;39.2%的患者存在大脑中动脉狭窄闭塞;(4)67.49%的急性缺血性脑卒中发生于颅内动脉,前循环急性缺血性脑卒中发生率(58.33%)高于后循环(33.47%),差异有统计学意义( P < 0.0001);(5)动脉到动脉栓塞、局灶穿枝动脉闭塞,低灌注栓子清除障碍是急性缺血性脑卒中常见发病机制,其中动脉到动脉栓塞为主要发病机制。 结论 多重影像评估的大样本的急性缺血性脑卒中的发病年龄、不同性别发病占比、动脉血管病理改变、责任血管发生率以及急性缺血性脑卒中发生机制对指导临床急性缺血性脑卒中的急救、二级预防、早期筛查及预防具有一定的指导作用。 Abstract:Objective To analyze the clinical characteristics of acute ischemic stroke combined with multiple imaging assessment. Methods Multiple images were combined to evaluate the incidence, arterial pathological changes, the responsible vessels for infarction, and infarct mechanism of 8441 acute ischemic strokes admitted to Xuanwu Hospital of Capital Medical University from 2014 to 2018. Results (1) The incidence of males was higher than that of females (74.7% vs 25.3%; P < 0.001) and the age of onset was smaller than females (58.83±12.56 years vs 63.37±13.27 years; P < 0.0001), 50-69 years old was the peak period of acute ischemic stroke (57.87%); (2) Hypertension, diabetes and hyperlipidemia are the main risk factors for acute ischemic stroke, and hypertension is the most common risk factor (28.65%); (3) Atherosclerosis (62.9%) is the most important pathological change and the most common cause of the arterial wall in acute ischemic stroke; 39.2% of patients have middle cerebral artery stenosis and occlusion; (4) 67.49% of acute ischemia strokeoccurs in the intracranial artery. The incidence of the anterior circulation (58.33%) is higher than that in the posterior circulation (33.47%), and the difference is statistically significant ( P < 0.0001); (5) Arterial-to-arterial embolism , local penetrating arterial occlusion and hypoperfusion impaired emboli clearance are common mechanism of acute ischemic stroke, of which arterial-to-arterial embolism is the main mechanism. Conclusion The age of onset of acute ischemic stroke, the proportion of different sexes, the pathological changes of arteries, the incidence of responsible blood vessels, and the mechanism of acute ischemic stroke of a large sample of acute ischemic stroke evaluated by multiple images can guide clinical acute ischemic stroke First aid, secondary prevention, early screening and prevention of stroke have a certain guiding role. -
Key words:
- Image /
- Acute ischemic stroke /
- Clinical characteristics
-

图 1 不同年龄段急性缺血性脑卒中发病占比(%)
Figure 1. The proportion of acute ischemic stroke in different age groups (%)

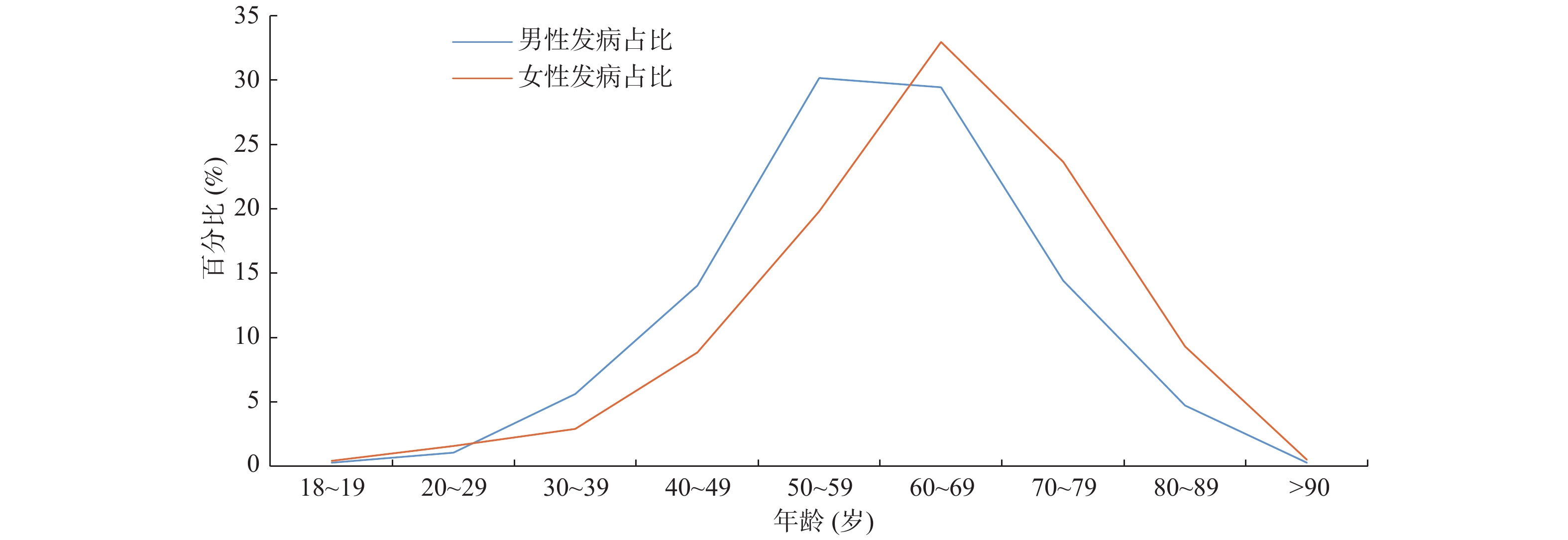
图 2 男女不同年龄段急性缺血性脑卒中发病占比
Figure 2. The proportion of acute ischemic stroke in men and women of different ages

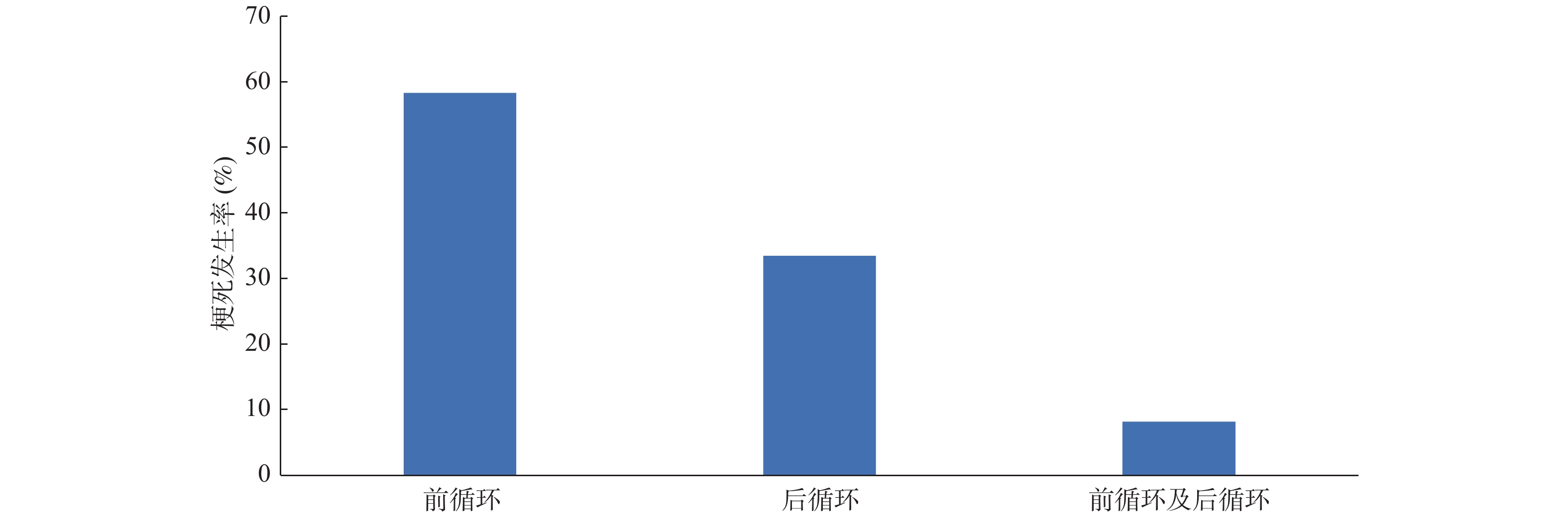
图 3 前循环与后循环的急性缺血性脑卒中发生率(%)
Figure 3. The incidence of acute ischemic stroke in anterior circulation and posterior circulation (%)

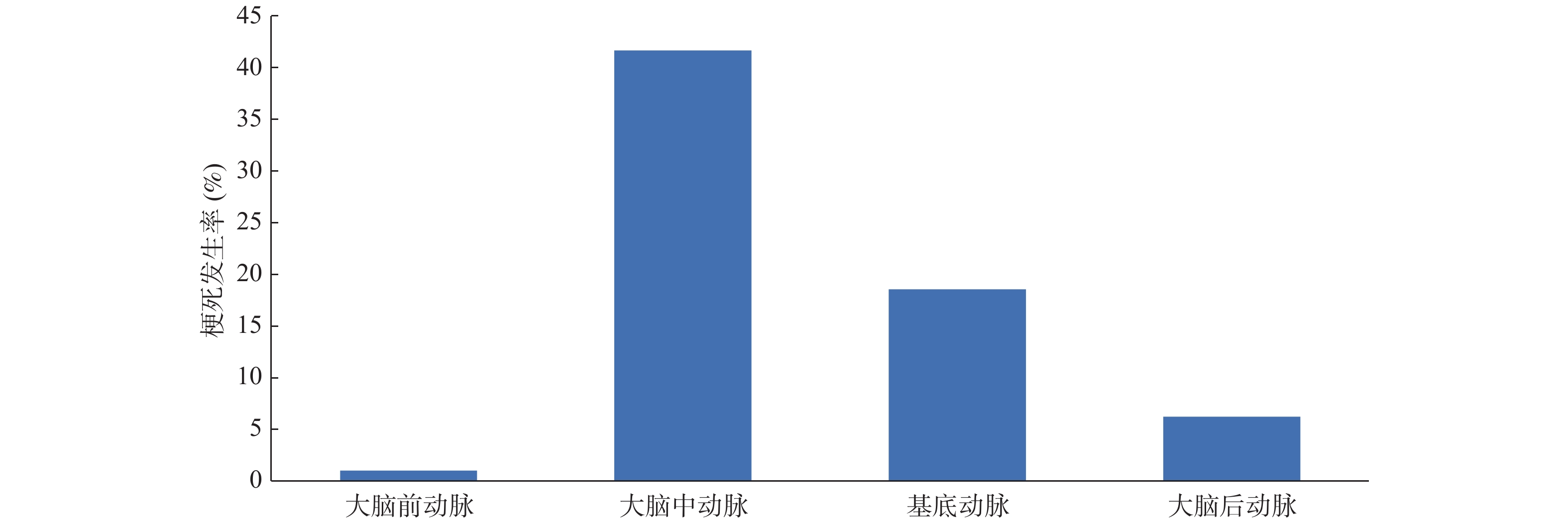
图 4 急性缺血性脑卒中颅内动脉发生率(%)
Figure 4. The incidence of intracranial artery in acute ischemic stroke (%)
表 1 急性缺血性脑卒中发病占比[n(%)]
Table 1. The proportion of acute ischemic stroke [n(%)]
年龄(岁) 总计 男性例数 女性例数 P 18~19 26(0.30) 17(0.27) 9(0.42) 0.265 20~29 100(1.18) 66(1.05) 34(1.59) 0.049* 30~39 417(4.94) 355(5.63) 62(2.90) 0.000* 40~49 1074(12.72) 885(14.03) 189(8.85) 0.000* 50~59 2325(27.54) 1902(30.17) 423(19.80) 0.000* 60~69 2560(30.35) 1856(29.44) 704(32.96) 0.002* 70~79 1413(16.74) 908(14.40) 505(23.65) 0.000* 80~89 497(5.89) 298(4.72) 199(9.32) 0.000* >90 29(0.34) 18(0.29) 11(0.51) 0.134 合计 8441(100.0) 6305(100.0) 2136(100.0) 男性与女性不同年龄段急性缺血性脑卒中发病占比的比较,*P<0.05。  下载: 导出CSV
下载: 导出CSV
表 2 危险因素[n(%)]
Table 2. Risk factors [n(%)]
危险因素 病例数 高血压 2419(28.65) 高脂血症 948(11.23) 糖尿病 934(11.06) 脑卒中史 788(9.33) 高同型半胱氨酸血症 297(3.52) 心脏因素 心房纤颤 193(2.32) 风心病 30(0.35) 心肌病 15(0.18) 卵圆孔未闭 45(0.53) 房间隔缺损 12(0.14) 糖耐量异常 29(0.34) 睡眠呼吸暂停综合症 9(0.11) 动脉夹层 133(1.6)
下载: 导出CSV
表 3 头颅多重影像的评估率[n(%)]
Table 3. The evaluation rate of multiple images of head [n(%)]
评估内容 病例数 血管影像学 头颈部CDU+TCCD 8435(99.93) 头颈部动脉CTA 5987(70.92) 全脑DSA 3082(36.57) 颅内动脉HR-MRI 343(4.06) 颅内动脉MRA 153(1.81) 结构影像学 头颅MRI+DWI 5812(68.85) 头颅CT平扫 1604(19.00) 功能影像学 头颅CTP 389(4.61) 头颅PWI 39(0.46) 头颅PET-CT 17(0.20)
下载: 导出CSV
表 4 多重影像评估的动脉壁病理改变[n(%)]
Table 4. The pathological changes of arterial wall assessed by multiple images [n(%)]
动脉壁病理改变 病例数 动脉硬化发生率 5306(62.86) 粥样硬化斑块 粥样斑块 4148(49.14) 溃疡斑块 195(2.31) 其它病理改变 壁内血肿 62(0.73) 附壁血栓 6(0.07) 动脉炎 8(0.09) 动脉蹼 3(0.04)
下载: 导出CSV
表 5 多重影像评估的动脉管腔病理改变[n(%)]
Table 5. The pathological changes of arterial lumen assessed by multiple images [n(%)]
动脉系统 病例数 前循环 颈总动脉狭窄闭塞 736(8.7) 颈内动脉狭窄闭塞 2437(28.9) 大脑中动脉狭窄闭塞 3313(39.2) 大脑前动脉狭窄闭塞 751(8.9) 后循环 椎动脉狭窄闭塞 2155(25.5) 基底动脉狭窄闭塞 1836(21.7) 大脑后动脉狭窄闭塞 2347(27.8) 椎动脉纤细 1186(14.0) 颅内交通支开放 1053(12.4)
下载: 导出CSV
表 6 DWI评估的急性缺血性脑卒中责任血管[n(%)]
Table 6. The responsible vessels of acute ischemic stroke assessed by DWI [n(%)]
责任血管 病例数 前循环 4924(58.33) 颈内动脉 553(6.56) 大脑前动脉 87(1.03) 大脑中动脉 4284(41.67) 后循环 2825(33.47) 椎动脉 732(8.67) 基底动脉 1567(18.56) 大脑后动脉 526(6.23) 前循环与后循环 692(8.20) 合计 8441(100)
下载: 导出CSV
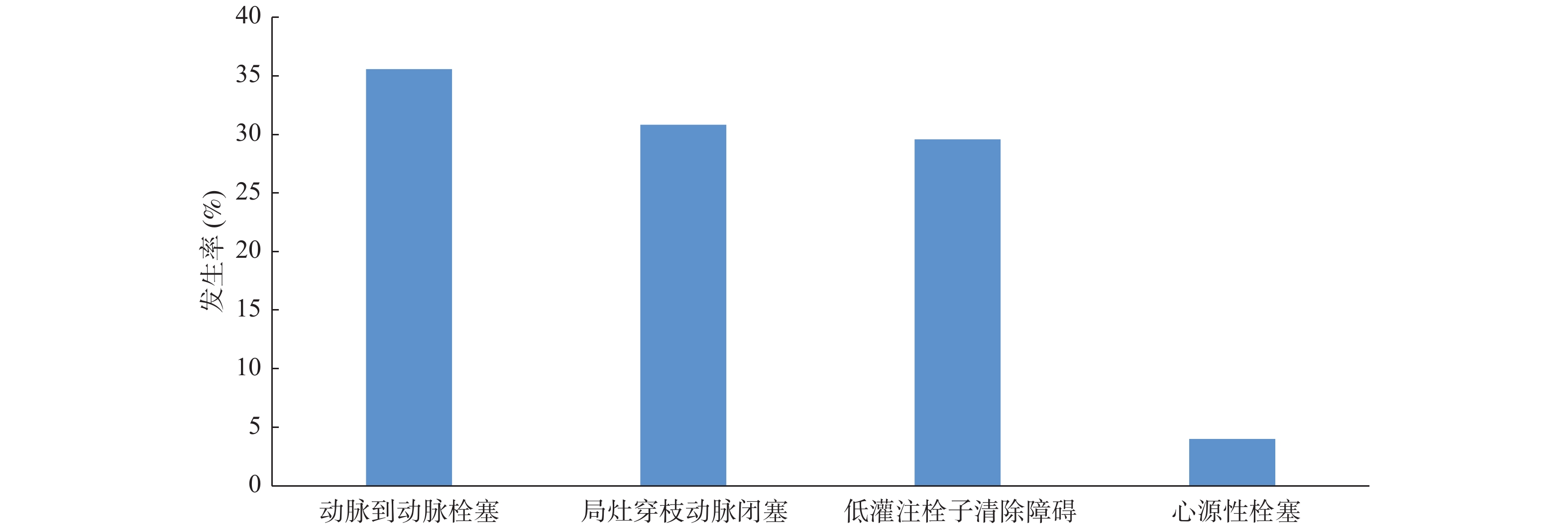
表 7 急性缺血性脑卒中发生机制[n(%)]
Table 7. The pathogenesis of acute ischemic stroke [n(%)]
发病机制 病例数 动脉到动脉栓塞 3002(35.57) 局灶穿枝动脉闭塞 2601(30.81) 低灌注栓子清除障碍 2498(29.59) 心源性栓塞 340(4.02) 合计 8441(100)
下载: 导出CSV
-
[1] 中华医学会神经病学分会,中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志,2015,48:246-257. [2] Guidelines for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack 2014-Aguideline for healthcare professionals from the American heart association/American stroke association[J]. Stroke, 2014, 45(7): 2160-2236. [3] 国家卫生计生委脑卒中防治工程委员会. 中国脑卒中血管超声检查指导规范[J]. 中华医学超声杂志,2015,12(8):599-610. [4] Mahmud M B,William D H,Adam D H,et al. Multicontrast High-Resolution Vessel Wall Magnetic Resonance Imaging and Its Value in Differentiating Intracranial Vasculopathic Processes[J]. Stroke,2015,46(6):1567-1573. doi: 10.1161/STROKEAHA.115.009037 [5] Saam T,Ferguson M S,Yarnykh V L,et al. Quantitative Evaluation of Carotid Plaque is (CICAS) Study[J]. Stroke,2014,45:234-239. [6] Bos D,Rijk M J M,Geeraedts T E A,et al. Intracranial Carotid Artery Atherosclerosis- Prevalence and Risk Factors in the General Population[J]. Stroke,2012,43(7):1878-1884. doi: 10.1161/STROKEAHA.111.648667 [7] Marquering H A,Nederkoorn P J,Bleeker L,et al. Intracranial carotid artery disease in patients with recent neurological symptoms:high prevalence on CTA[J]. Neuroradiology,2013,55(2):179-185. [8] Hua Y,Meng X F,Jia L Y,et al. Color Doppler imaging evaluation of proximal vertebral artery stenosis[J]. AJR Am J Roentgenol,2009,193(5):1434-1438. doi: 10.2214/AJR.09.2624 [9] H J M Barnett,D W Taylor,R B Haynes,et al. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis[J]. N Engl J Med,1991,325(7):445-453. doi: 10.1056/NEJM199108153250701 [10] Bash S,Villablanca J P,Jahan R,et al. Intracranial Vascular Stenosis and Occlusive Disease:Evaluation with CT Angiography,MR Angiography,and Digital Subtraction Angiography[J]. AJNR Am J Neuroradiol,2005,26(5):1012-1021. [11] Babo M,Marchis G M D,Sarikaya H,et al. Differences and Similarities Between Spontaneous Dissections of the Internal Carotid Artery and the Vertebral Artery (Revision 2)[J]. Stroke,2013,44(6):1537-1542. doi: 10.1161/STROKEAHA.113.001057 [12] 牛婧雯,徐蔚海. 脑动脉夹层影像学诊断[J]. 中国实用内科杂志,2014,34(5):447-449. [13] Mandell D M,Matouk C C,Farb R I,et al. Vessel Wall MRI to Differentiate Between Reversible Cerebral Vasoconstriction Syndrome and Central Nervous System Vasculitis-Preliminary Results[J]. Stroke,2012,43(3):860-862. doi: 10.1161/STROKEAHA.111.626184 [14] Tatu L,Moulin T,Bogousslavsky J,et al. Arterial territories of the human brain:Cerebral hemispheres[J]. Neurology,1998,50(1):1699-1708. [15] Kim D E,Park J H,Schellingerhout D,et al. Mapping the Supratentorial Cerebral Arterial Territories Using 1160 Large Artery Infarcts[J]. JAMA Neurol,2019,76(1):8. doi: 10.1001/jamaneurol [16] Wu F,Song H,Ma Q,et al. Hyperintense Plaque on Intracranial Vessel Wall Magnetic Resonance Imaging as a Predictor of Artery-to-Artery Embolic Infarction[J]. Stroke,2018,49(4):905-911. doi: 10.1161/STROKEAHA.117.020046 [17] Gao S,Wang Y J,Xu A D,et al. Chinese ischemic stroke subclassification[J]. Frontiers in Neurology,2011,2(6):1-4. [18] Isabelle M M,Jean-Claude B. The Pathophysiology of Watershed Infarction in Internal Carotid Artery Disease Review of Cerebral Perfusion Studies[J]. Stroke,2005,36(3):567-577. doi: 10.1161/01.STR.0000155727.82242.e1 [19] Wong K S,Gao S,Chan Y L,et al. Mechanisms of Acute Cerebral Infarctions in Patients with Middle Cerebral Artery Stenosis:A Diffusion-Weighted Imaging and Microemboli Monitoring Study[J]. Ann Neurol,2002,52(1):74-81. doi: 10.1002/ana.10250 [20] Kim J S,Nah H W,Park S M,et al. Risk Factors and Stroke Mechanisms in Atherosclerotic Stroke:Intracranial Compared With Extracranial and Anterior Compared With Posterior Circulation Disease[J]. Stroke,2012,43(12):3313-3318. doi: 10.1161/STROKEAHA.112.658500 [21] Feng X,Chan K L,Lan L,et al. Stroke Mechanisms in Symptomatic Intracranial Atherosclerotic Disease-Classification and Clinical Implications[J]. Stroke,2019,50(10):2692-2699. doi: 10.1161/STROKEAHA.119.025732 [22] W W,Jiang B,Sun H,et al. Prevalence,Incidence,and Mortality of Stroke in China. Results from a Nationwide Population-Based Survey[J]. Circulation,2017,135(8):759-771. doi: 10.1161/CIRCULATIONAHA.116.025250 [23] Liu M,Wu B,Wang W Z,et al. Stroke in China:epidemiology,prevention,and management strategies[J]. Lancet Neurol,2007,6(5):456-464. doi: 10.1016/S1474-4422(07)70004-2 [24] Wu S,Wu B,Liu M,et al. Stroke in China:advances and challenges in epidemiology,prevention,and management[J]. Lancet Neurol,2019,18(4):394-405. doi: 10.1016/S1474-4422(18)30500-3 [25] 胡盛寿,高润霖,刘力生,等. 《中国心血管病报告2018》概要[J]. 中国循环杂志,2019,34(3):209-219. [26] Marini C,Santis F,Sacco S,et al. Contribution of Atrial Fibrillation to Incidence and Outcome of Ischemic Stroke. Results From a Population-Based Study[J]. Stroke,2005,36(6):1115-1119. doi: 10.1161/01.STR.0000166053.83476.4a [27] Johnson K G,Johnson D C. Frequency of Sleep Apnea in Stroke and TIA Patients:A Meta-analysis[J]. J Clin Sleep Med,2010,6(2):131-137. doi: 10.5664/jcsm.27760 [28] Putaala J,Metso A J,Metso T M,et al. Analysis of 1008 Consecutive Patients Aged 15 to 49 With First-Ever Ischemic Stroke. The Helsinki Young Stroke Registry[J]. Stroke,2009,40(4):1195-1203. doi: 10.1161/STROKEAHA.108.529883 [29] Tsivgoulis G,Vadikolias K,Heliopoulos I,et al. Prevalence of Symptomatic Intracranial Atherosclerosis in Caucasians:A Prospective,Multicenter,Transcranial Doppler Study[J]. Stroke,2014,45(3):663-669. doi: 10.1111/j.1552-6569.2012.00707.x [30] Hoshino T,Sissani L,Labreuche J,et al. Prevalence of Systemic Atherosclerosis Burdens and Overlapping Stroke Etiologies and Their Associations With Long-term Vascular Prognosis in Stroke With Intracranial Atherosclerotic Disease[J]. JAMA Neurol,2018,75(2):203-211. doi: 10.1001/jamaneurol.2017.3960 [31] Chen H B,Hong H,Shihui Xing S H,et al. Intracranial versus Extracranial Symptomatic Carotid Atherosclerosis in Chinese Patients:Risk Factors,Stroke Mechanisms,and Long-Term Prognosis[J]. Journal of Stroke and Cerebrovascular Diseases,2015,24(11):2632-2639. doi: 10.1016/j.jstrokecerebrovasdis.2015.07.019 [32] Wang Y, Zhao X, Liu L, et al. Prevalence and outcomes of symptomatic intracranial large artery stenoses and occlusions in China-the Chinese intracranial atheroscleros [33] Gorelick P B,Wong K S,Bae H J,et al. Large Artery Intracranial Occlusive Disease-A Large Worldwide Burden but a Relatively Neglected Frontier[J]. Stroke,2008,39(8):2396-2399. doi: 10.1161/STROKEAHA.107.505776 [34] Hua Y,Jia L,Xing Y,et al. Distribution Pattern of Atherosclerotic Stenosis in Chinese Patients with Stroke:A Multicenter Registry Study[J]. Aging and Disease,2019,10(11):62-70. doi: 10.14336/AD.2018.0602 [35] Kim J T,Yoo S H,Kwon J H,et al. Subtyping of Ischemic Stroke Based on Vascular Imaging:Analysis of 1,167 Acute,Consecutive Patients[J]. J Clin Neurol,2006,2(4):225-230. doi: 10.3988/jcn.2006.2.4.225 [36] Leng X,Lan L,Ip H L,et al. Hemodynamics and Stroke Risk in Intracranial Atherosclerotic Disease[J]. Ann Neurol,2019,85(5):752-764. doi: 10.1002/ana.25456 [37] Lee D K,Kim J S,Kwon S U,et al. Lesion Patterns and Stroke Mechanism in Atherosclerotic Middle Cerebral Artery Disease:Early Diffusion-Weighted Imaging Study[J]. Stroke,2005,36(12):2583-2588. doi: 10.1161/01.STR.0000189999.19948.14 -

 点击查看大图
点击查看大图

计量
- 文章访问数: 3961
- HTML全文浏览量: 2627
- PDF下载量: 27
- 被引次数: 0
