

Clinical Features and Morphological Risk Factors of Ruptured and Hemorrhage of Posterior Communicating Artery Aneurysm
-
摘要:
目的 分析颅内后交通动脉瘤破裂出血的临床特征和形态学危险因素,以期为后交通动脉瘤的临床诊治提供决策依据。 方法 对昆明医科大学第一附属医院神经外二科2016年1月至2020年12月诊断为后交通动脉瘤的72例患者的临床资料进行回顾性分析。统计患者的临床资料和动脉瘤形态学参数,根据是否并发蛛网膜下腔出血分为破裂组和未破裂组,使用SPSS软件进行统计学分析,分析与后交通动脉瘤破裂有关的危险因素。 结果 2组患者在基础特征如性别、年龄、吸烟史的比较,差异无统计学意义(P > 0.05),而在高血压、动脉瘤的最大直径小于5 mm、入射角 > 90°、子囊和泡样突起、形态是否规则的、瘤顶朝向的比较,差异有统计学意义(P < 0.05)。多因素分析表明,高血压(OR:5.82,95%CI:1.23~27.51)、射角大于90°(OR:7.88,95%CI:1.27~48.59)、子囊和泡样突起(OR:11.92,95%CI:2.06~68.76)是后交通动脉瘤破裂的独立危险因素。 结论 高血压史、最大直径小于5 mm、入射角大于 90°、子囊和动脉瘤泡样突起、瘤顶朝向后外下方是后交通动脉瘤破裂的危险因素裂。 Abstract:Objective To analyze the clinical features and morphological risk factors of rupture and hemorrhage of posterior communicating artery aneurysm in the brain, in order to provide decision-making basis for the clinical diagnosis and treatment of posterior communicating artery aneurysm. Methods The clinical data of 72 patients diagnosed with posterior communicating aneurysm from January 2016 to December 2020 in the Second Department of Neurosurgery, First Affiliated Hospital of Kunming Medical University were retrospectively analyzed. The clinical data and aneurysm morphological parameters of the patients were collected. According to whether subarachnoid hemorrhage was complicated, they were divided into ruptured group and unruptured group. SPSS software was used for statistical analysis to analyze the risk factors related to the rupture of posterior communicating aneurysm. Results There was no statistically significant difference (P > 0.05) between the two groups in the comparison of basic characteristics such as gender, age, and smoking history, while there was a statistically significant difference (P < 0.05) in the comparison of hypertension, maximum diameter of the aneurysm less than 5 mm, Inflow angle more than 90°, daughter sacs and bleb, whether the morphology was regular or not, and the orientation of the apex of the aneurysm. Multifactorial analysis showed that hypertension (OR: 5.82, 95% CI : 1.23-27.51), Inflow angle > 90° (OR: 7.88, 95% CI: 1.27-48.59), and daughter sacs and bleb (OR: 11.92, 95% CI: 2.06-68.76) were independent risk factors for posterior communicating aneurysm rupture. Conclusion A history of hypertension, a maximum diameter smaller than 5 mm, an Inflow angle greater than 90°, daughter sacs and bleb ,dome of the aneurysm directed to posterior-outer-inferior were risk factors for posterior communicating aneurysm rupture. Conclusion A history of hypertension, a maximum diameter smaller than 5 mm, an Inflow angle greater than 90°, daughter sacs and bleb ,dome of the aneurysm directed to posterior-outer-inferior were risk factors for posterior communicating aneurysm rupture. -

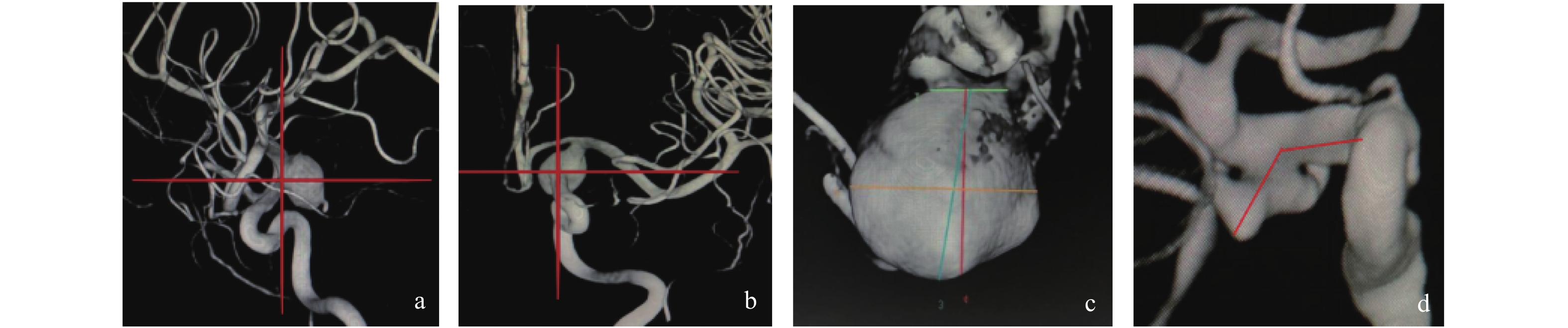
图 1 动脉瘤参数测量
a-b :所示以后交通动脉与颈内动脉交点为原点建立的参考系;c:绿色线为动脉瘤颈,橙色线为动脉瘤宽度,蓝色线为动脉瘤最大直径,红色线为动脉瘤高度;d:为动脉瘤流入角。
Figure 1. Measurement of aneurysm parameters

图 2 后交通动脉瘤的几何形态
a:瘤壁表面光滑且类球形的规则动脉瘤;b:瘤壁表面光滑的类条状不规则动脉瘤;c:分叶状不规则动脉瘤;d:瘤壁表面有多个泡样突起的不规则球形动脉瘤;e:瘤壁表面有一带蒂子囊且类球形的规则动脉瘤;f:瘤壁表面有一个泡样突起且类球形的规则动脉瘤。
Figure 2. Geometry of posterior communicating aneurysm
表 1 高血压与动脉瘤破裂的关系[n(%)]
Table 1. The relationship between hypertension and ruptured aneurysm [n(%)]
分组 未破裂组 破裂组 χ2 P 女性 20(40.0) 30(60.0) 0.632 0.043 男性 11(50.0) 11(50.0) 年龄小于60岁 17(39.5) 26(60.5) 0.43 0.836 年龄大于60岁 14(48.3) 15(51.7) 无吸烟史 27(46.6) 31(53.4) 1.487 0.223 有吸烟史 4(28.5) 10(71.5) 无高血压史 15(65.2) 8(34.8) 有高血压史 16(32.7) 33(67.3) 6.77 0.009* *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 动脉瘤最大直径与动脉瘤破裂的关系[
$ \bar x \pm s $ ,n(%)]Table 2. The relationship between the maximum diameter of aneurysm and rupture of aneurysm [
$ \bar x \pm s $ ,n(%)]分组 未破裂组 破裂组 t/χ2 P 最大直径(mm) 7.65 ± 4.31 4.92 ± 2.37 3.173 0.030* 最大直径分组 9.687 0.008* 大于7 mm 16(69.6) 7(30.4) 5~7 mm 4(30.8) 9(69.2) 小于5 mm 11(30.6) 25(69.4) 9.687 0.008* *P < 0.05。
下载: 导出CSV
表 3 动脉瘤纵横与动脉瘤破裂的关系[
$ \bar x \pm s $ ,n(%)]Table 3. The relationship between aneurysm aspect and aneurysm rupture [
$ \bar x \pm s $ ,n(%)]分组 未破裂组 破裂组 t/χ2 P AR 1.63 ± 0.93 1.34 ± 0.64 1.58 0.110 AR是否大于1.4 1.01 0.310 否 16(38.1) 26(61.9) 是 15(50) 15(50) *P < 0.05。
下载: 导出CSV
表 4 动脉瘤颈的宽度与动脉瘤破裂的关系[
$ \bar x \pm s $ ,n(%)]Table 4. The relationship between the width of aneurysm neck and the rupture of aneurysm [
$ \bar x \pm s $ ,n(%)]分组 未破裂组 破裂组 t/χ2 P 瘤颈宽度(mm) 5.00 ± 2.51 3.85 ± 1.49 2.273 0.020* 体颈比 1.19 ± 0.43 1.25 ± 0.45 0.577 0.560 瘤颈是否大约4 mm 4.09 0.040* 否 13(32.5) 27(67.5) 4.09 0.040* 是 18(56.3) 14(43.8) *P < 0.05。
下载: 导出CSV
表 5 动脉入射角与动脉瘤破裂的关系[
$ \bar x \pm s $ ,n(%)]Table 5. The relationship between arterial incidence angle and aneurysm rupture[
$ \bar x \pm s $ ,n(%)]分组 未破裂组 破裂组 t/χ2 P 动脉瘤入射角 104.78 ± 29.69 114.97 ± 15.15 1.747 0.080 是否大于90° 6.969 0.008* 否 12(75.0) 4(25.0) 是 19(33.9) 37(66.1) 6.969 0.008* *P < 0.05。
下载: 导出CSV
表 6 动脉瘤几何形态与破裂出血的关系[n(%)]
Table 6. The relationship between aneurysm geometry and rupture and bleeding [n(%)]
分组 未破裂组 破裂组 χ2 P 动脉瘤形态 3.88 0.040* 规则 17(56.7) 13(43.3) 不规则 14(33.3) 28(66.7) 3.88 0.040* 子囊和泡样突起 无 20(66.7) 10(33.3) 有 11(26.2) 31(73.8) 11.694 0.001* *P < 0.05。
下载: 导出CSV
表 7 动脉瘤顶的方向与破裂出血的关系[n(%)]
Table 7. The relationship between the direction of the top of aneurysm and rupture [n(%)]
分组 未破裂组 破裂组 χ2 P 后内下 10(66.7) 5(33.3) 后外下 11(26.8) 30(73.2) 12.239 0.007 * 后内上 7(77.8) 2(22.2) 后外上 3(42.9) 4(57.1) *P < 0.05。
下载: 导出CSV
表 8 后交通动脉瘤破裂的多因素分析
Table 8. Multi-factor analysis of posterior communicating artery aneurysm rupture
危险因素 比较 OR 95%CI P 高血压病史 有 5.82 1.23~27.51 0.020* 无子囊和泡样突起 有 11.92 2.06~68.76 0.006* 入射角是否大于90° 是 7.88 1.27~48.59 0.020* 瘤顶指向 后内下 - - 0.016* 后外下 8.51 1.085~66.84 0.042* 后内上 0.251 0.02~3.20 0.288 后外上 2.389 0.084~68.07 0.610 动脉瘤最大径 大于7 mm - - 0.030* 5~7 mm 1.019 0.11~9.38 0.987 小于5 mm 10.95 1.76~67.82 0.010* *P < 0.05。
下载: 导出CSV
-
[1] Golshani K,Ferrell A,Zomorodi A,et al. A review of the management of posterior communicating artery aneurysms in the modern era[J]. Surg Neurol Int,2010,22(1):88. [2] Clarke G,Mendelow A D,Mitchell P. Predicting the risk of rupture of intracranial aneurysms based on anatomical location[J]. Acta Neurochirurgica,2005,147(3):259-263. doi: 10.1007/s00701-004-0473-3 [3] Engelhardt J,Berge J,Cuny E,et al. Oculomotor nerve palsy induced by internal carotid artery aneurysm:Prognostic factors for recovery[J]. Acta Neurochirurgica,2015,157(7):1103-1111. doi: 10.1007/s00701-015-2440-6 [4] Gelabert-glnzalez M,Iglesias-pais M,Fernández-villa J. Acute subdural haematoma due to ruptured intracranial aneurysms[J]. Neurosurgical Review,2004,27(4):259-262. [5] He W,Gandhi C D,Quinn J,et al. True aneurysms of the posterior communicating artery:A systematic review and meta-analysis of individual patient data[J]. World Neurosurgery,2011,75(1):64-72. doi: 10.1016/j.wneu.2010.09.012 [6] De Rooij N K,Velthuis B K,Algra A,et al. Configuration of the circle of willis,direction of flow,and shape of the aneurysm as risk factors for rupture of intracranial aneurysms[J]. J Neurol,2009,256(1):45-50. doi: 10.1007/s00415-009-0028-x [7] Morita A,Kirino T,Hashi K,et al. The natural course of unruptured cerebral aneurysms in a Japanese cohort[J]. N Engl J Med,2012,366(26):2474-2482. doi: 10.1056/NEJMoa1113260 [8] Knekt P,Reunanen A,Aho K,et al. Risk factors for subarachnoid hemorrhage in a longitudinal population study[J]. Journal of Clinical Epidemiology,1991,44(9):933-939. doi: 10.1016/0895-4356(91)90056-F [9] Solanki C,Pandey P,Rao K V. Predictors of aneurysmal rebleed before definitive surgical or endovascular management[J]. Acta Neurochirurgica,2016,158(6):1037-1044. doi: 10.1007/s00701-016-2784-6 [10] Qian Z,Kang H,Tang K,et al. Assessment of risk of aneurysmal rupture in patients with normotensives,Controlled hypertension,and uncontrolled hypertension[J]. Journal of Stroke and Cerebrovascular Diseases:The Official Journal of National Stroke Association,2016,25(7):1746-1752. doi: 10.1016/j.jstrokecerebrovasdis.2016.03.027 [11] Müller T B,Vik A,Romundstad P R,Sandvei M S. Risk factors for unruptured intracranial aneurysms and subarachnoid hemorrhage in a prospective population-based study[J]. Stroke ,2019,50(10):2952-2955. doi: 10.1161/STROKEAHA.119.025951 [12] Etminan N,Chang H S,Hackenberg K,et al. Worldwide incidence of aneurysmal subarachnoid hemorrhage according to region,Time period,Blood pressure,and smoking prevalence in the population:A systematic review and meta-analysis[J]. JAMA Neurol,2019,76(5):588-597. doi: 10.1001/jamaneurol.2019.0006 [13] Chang H S. Simulation of the natural history of cerebral aneurysms based on data from the international study of unruptured intracranial aneurysms[J]. J Neurosurge,2006,104(2):188-194. doi: 10.3171/jns.2006.104.2.188 [14] Etminan N,Dreier R,Buchholz B A,et al. Age of collagen in intracranial saccular aneurysms[J]. Stroke,2014,45(6):1757-1763. doi: 10.1161/STROKEAHA.114.005461 [15] Debrun G M,Aletich V A,Kehtli P,et al. Selection of cerebral aneurysms for treatment using guglielmi detachable coils:The preliminary University of Illinois at chicago experience[J]. Neurosurgery,1998,43(6):1281-1295. [16] Forget T R,JR. ,Benitez R,Veznedaroglu E,et al. A review of size and location of ruptured intracranial aneurysms[J]. Neurosurgery,2001,49(6):1322-1325. doi: 10.1097/00006123-200112000-00006 [17] Ujiie H,Tamano Y,Sasaki K,et al. Is the aspect ratio a reliable index for predicting the rupture of a saccular aneurysm?[J]. Neurosurgery,2001,48(3):495-502. doi: 10.1097/00006123-200103000-00007 [18] Meng H,Wang Z,Hoi Y,et al. Complex hemodynamics at the apex of an arterial bifurcation induces vascular remodeling resembling cerebral aneurysm initiation[J]. Stroke,2007,38(6):1924-1931. doi: 10.1161/STROKEAHA.106.481234 [19] Bjorkman J,Frosen J,Tahtinen O,et al. Irregular shape identifies ruptured intracranial aneurysm in subarachnoid hemorrhage patients with multiple aneurysms[J]. Stroke,2017,48(7):1986-1989. doi: 10.1161/STROKEAHA.117.017147 [20] Zhang J,Can A,Lai P M R,et al. Age and morphology of posterior communicating artery aneurysms[J]. Scientific Reports,2020,10(1):11545-11545. doi: 10.1038/s41598-020-68276-9 [21] Beck J,Rohde S,E L Beltagy M,et al. Difference in configuration of ruptured and unruptured intracranial aneurysms determined by biplanar digital subtraction angiography[J]. Acta Neurochirurgica,2003,145(10):861-865. doi: 10.1007/s00701-003-0124-0 [22] Xu Z,Kim B S,L K S,et al. Morphological and clinical risk factors for the rupture of posterior communicating artery aneurysms:Significance of fetal-type posterior cerebral artery[J]. Neurol Sci,2019,40(11):2377-2382. doi: 10.1007/s10072-019-03991-4 -










 点击查看大图
点击查看大图
计量
- 文章访问数: 3456
- HTML全文浏览量: 2024
- PDF下载量: 38
- 被引次数: 0
