

Comparative Analysis of Early Efficacy of Arthroscopy Combined with Open High Tibial Osteotomy in the Treatment of Knee Osteoarthritis
-
摘要:
目的 分析探讨关节镜结合开放胫骨高位截骨术(open wedge high tibial osteotomy,OWHTO)与单纯开放胫骨高位截骨术治疗膝关节骨关节炎的临床疗效。 方法 回顾性分析2018年1月至2020年1月骨科收治的因膝关节骨关节炎接受手术治疗的34例(39膝)患者的临床资料,根据手术方式分为2组,A组为关节镜联合OWHTO手术治疗的共17例,B组为单纯接受OWHTO手术治疗的共22例。比较2组临床疗效。 结果 (1)2组患者在术前HSS评分、VAS疼痛视觉模拟评分、膝关节活动度、Lysholm膝关节评分方面的差异均无显著差异,具有可比性;(2)2组患者术后3 d、1月的 HSS 和、VAS 评分、Lysholm膝关节评分有显著差异,A组高于B组,差异有统计学意义(P < 0.05);但2组术后3月、6月、12月的 HSS 和、VAS 评分、Lysholm膝关节评分无显著差异;2组患者术后3 d、1月、3月、6月、12月的膝关节活动度均无明显差异(P > 0.05)。 结论 关节镜联合开放胫骨高位截骨术相比较于单纯开放胫骨高位截骨术治疗膝关节骨关节炎早期在疼痛缓解方面能取得较为显著的效果,中远期临床疗效无明显差异。 Abstract:Objective To analyze the clinical effect of arthroscopy combined with open-wedge high Tibial osteotomy (OWHTO) and open-tibial high osteotomy alone in the treatment of knee osteoarthritis. Methods The clinical data of 34 patients (39 knees) who received surgery for osteoarthritis of the knee in our department from January 2018 to January 2020 were retrospectively analyzed. They were divided into two groups according to the surgical methods. Group A consisted of 17 patients who received arthroscopy combined with OWHTO surgery, and group B consisted of 22 patients who received OWHTO surgery alone. The clinical efficacy of the two groups was compared. Results (1) There were no significant differences in preoperative HSS score, VAS visual simulation score, knee range of motion and Lysholm knee score between the two groups, which makes the two groups comparable. (2) There were significant differences in HSS, VAS and Lysholm knee score between 2 groups 3 days and 1 month after surgery, and group A was higher than group B, with statistical significance (P < 0.05); however, there were no significant differences in HSS, VAS score, Lysholm knee score at 3 months, 6 months and 12 months postoperatively between the two groups. There was no significant difference in knee joint range of motion between the two groups 3 days, 1 month, 3 months, 6 months and 12 months after operation. Conclusion Arthroscopy combined with open tibial high osteotomy is more effective than open tibial high osteotomy alone in the treatment of early knee osteoarthritis in terms of pain relief, and there is no significant difference in the long-term clinical efficacy. -
Key words:
- Knee /
- Osteoarthritis /
- Osteotomy /
- Tibia /
- Knee arthroscopy
-
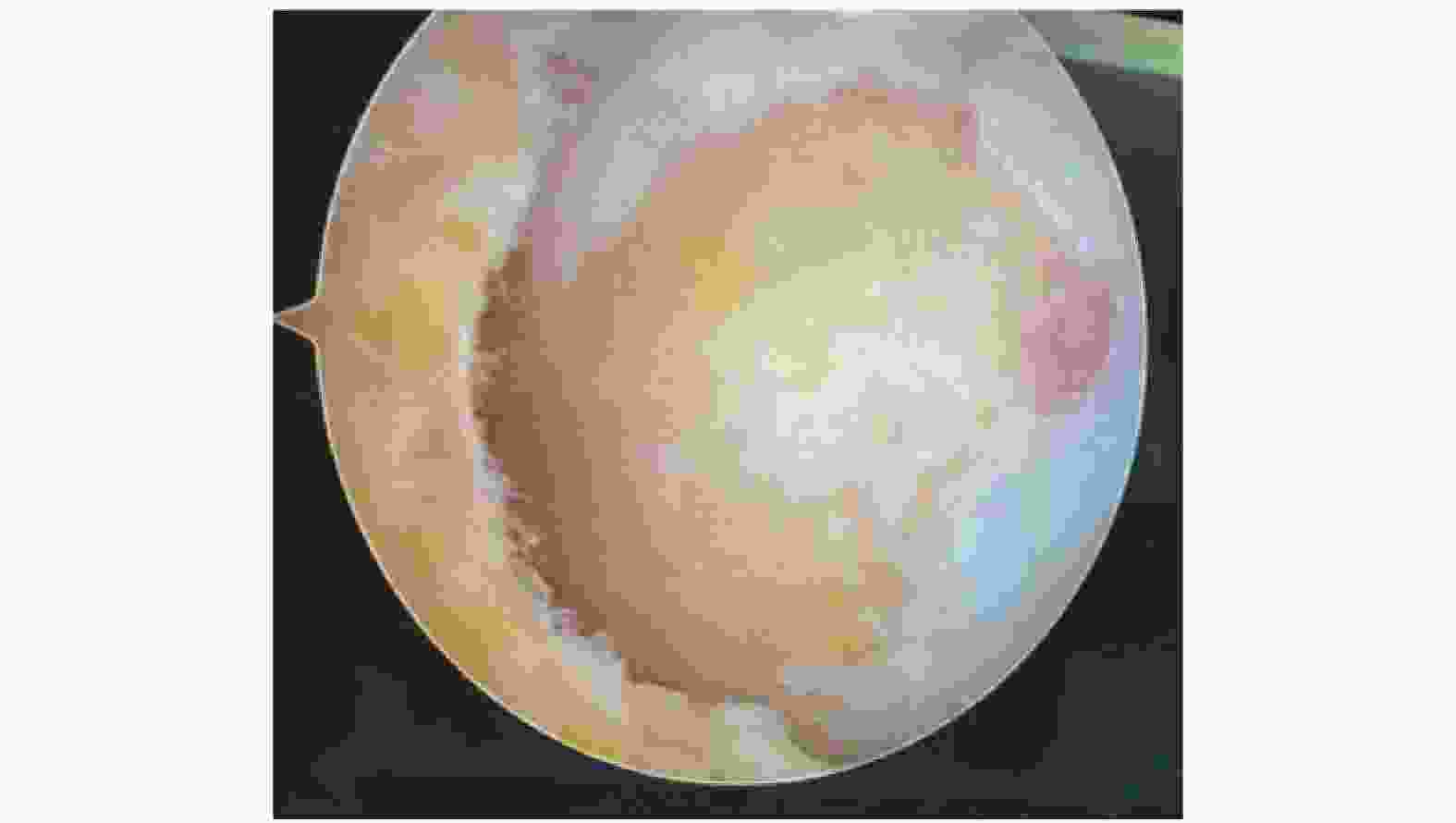
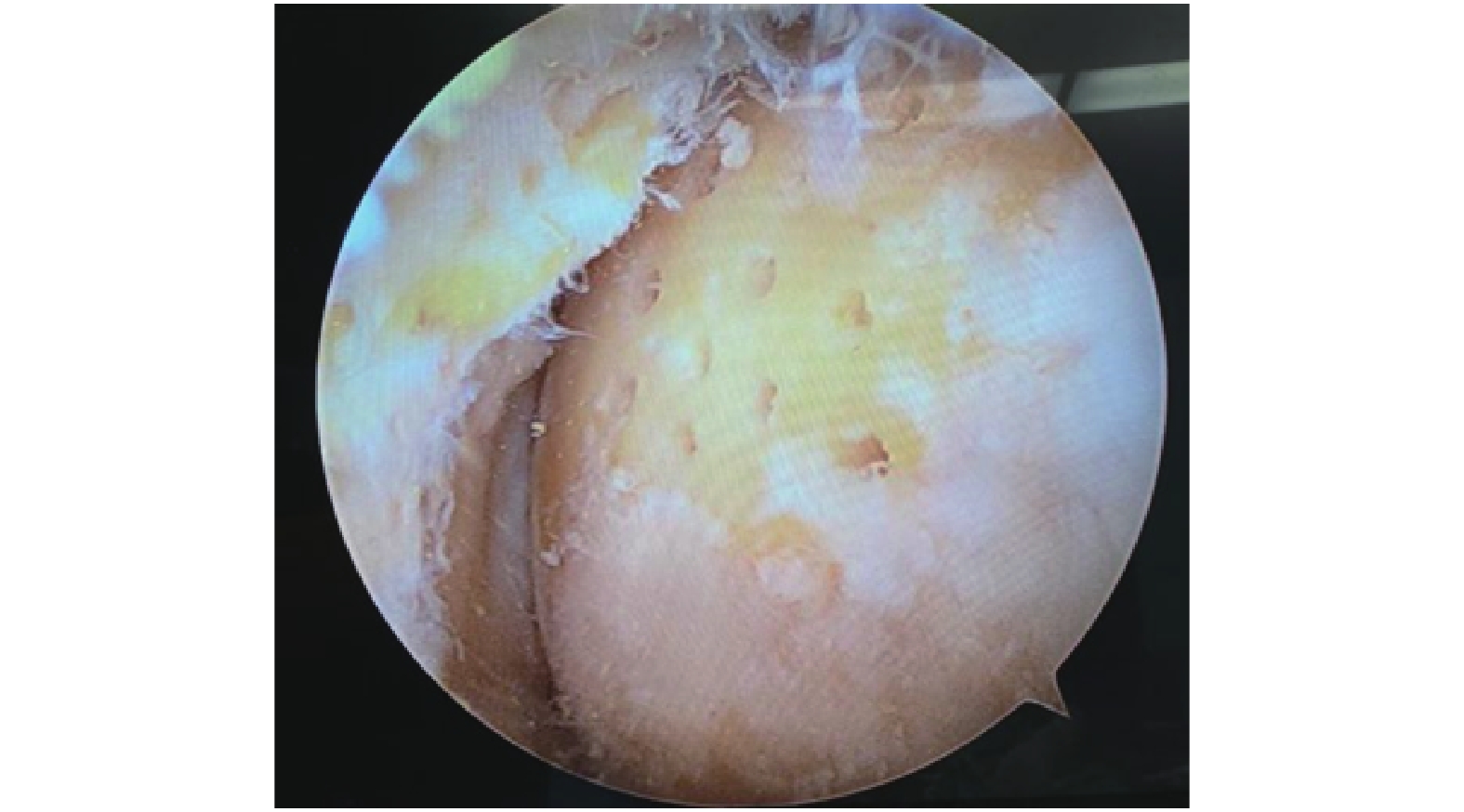
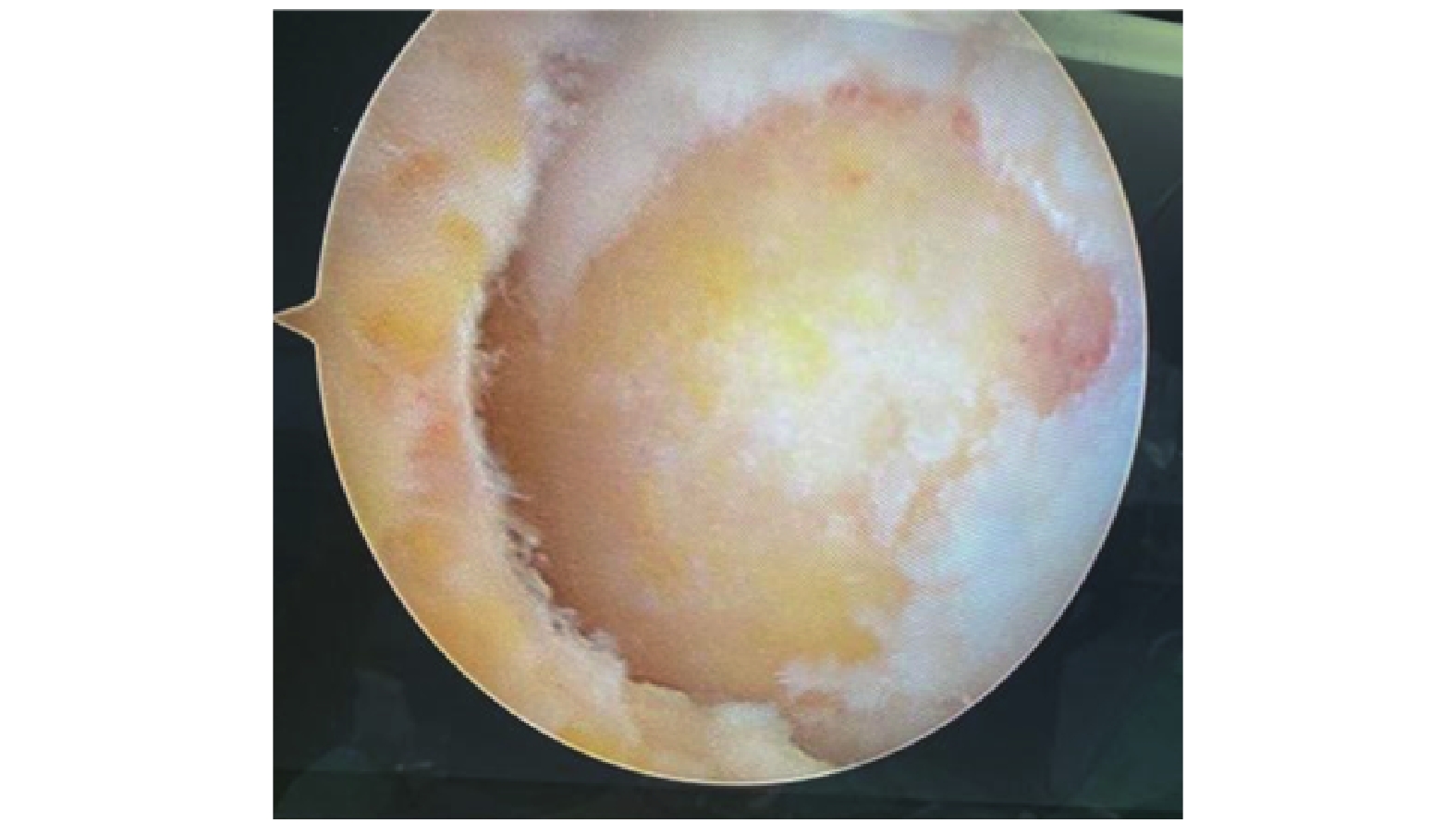
图 1 关节镜下见外侧股骨踝软骨磨损剥脱
Figure 1. The femoral condylar cartilage was worn and exfoliated under arthroscopy

图 3 术前双下肢全景摄影片见左下肢明显膝内翻畸形
Figure 3. Preoperative panoramic film of both lower limbs showed obvious varus deformity of the left lower limb

图 4 术后3 d复查双下肢全景摄影片见左下肢膝内翻畸形已经纠正
Figure 4. 3 d post-surgery panoramic film of both lower limbs showed that the varus deformity of the left lower limb had been corrected

图 5 术后3月复查双下肢全长片
Figure 5. Full-length radiographs of both lower limbs 3 months after surgery
表 1 术前膝关节评分(
$\bar x \pm s $ )Table 1. Preoperative knee scores (
$\bar x \pm s $ )术前膝关节评分 A组 B组 t P 术前VAS评分(分) 7.15 ± 1.10 7.27 ± 0.96 0.235 0.769 术前膝关节活动度(°) 99.32 ± 11.30 100.41 ± 12.21 0.318 0.657 术前HSS评分(分) 44.32 ± 6.94 44.11 ± 5.17 0.207 0.824 术前LYSHOLM评分(分) 45.28 ± 5.26 46.67 ± 6.48 0.196 0.859  下载: 导出CSV
下载: 导出CSV
表 2 术前及术后髋膝踝角[(
$\bar x \pm s $ )°]Table 2. Preoperative and Postoperative Hip-knee-ankle angle [(
$\bar x \pm s $ )°]髋膝踝角 A组 B组 t P 术前 171.28 ± 2.76 172.44 ± 3.62 0.339 0.515 术后 180.43 ± 2.81 181.49 ± 2.52 0.327 0.629 t 4.629 5.368 P < 0.001* < 0.001* *P < 0.05。
下载: 导出CSV
表 3 术后膝关节评分[(
$\bar x \pm s $ )分]Table 3. Postoperative knee score [(
$\bar x \pm s $ )score]术后恢复评分 A组 B组 t P VAS评分 术后3 d 3.28 ± 0.81 4.76 ± 0.95 3.469 < 0.001* 术后1月 2.38 ± 0.74 3.46 ± 0.80 2.926 0.003* 术后3月 1.68 ± 0.90 1.84 ± 1.03 0.228 0.795 术后6月 1.24 ± 0.65 1.37 ± 0.84 0.201 0.845 术后12月 1.12 ± 0.39 1.20 ± 0.46 0.192 0.896 HSS评分 术后3 d 80.63 ± 5.4 72.54 ± 6.7 3.318 < 0.001* 术后1月 86.14 ± 5.8 79.65 ± 6.9 2.673 0.006* 术后3月 88.23 ± 4.1 86.57 ± 4.6 0.267 0.713 术后6月 89.35 ± 3.5 87.64 ± 4.7 0.198 0.849 术后12月 90.53 ± 3.3 89.59 ± 3.1 0.182 0.898 LYSHOLM评分 术后3 d 79.42 ± 4.5 71.68 ± 5.9 3.572 < 0.001* 术后1月 85.94 ± 6.6 79.86 ± 6.7 2.598 0.008* 术后3月 87.32 ± 4.6 86.25 ± 5.6 0.231 0.786 术后6月 89.78 ± 5.7 87.12 ± 4.3 0.285 0.695 术后12月 91.44 ± 3.8 90.45 ± 3.6 0.234 0.772 膝关节活动度(°) 术后3 d 102.35 ± 10.68 103.03 ± 7.84 0.232 0.782 术后1月 120.32 ± 12.40 118.08 ± 8.99 0.322 0.649 术后3月 128.12 ± 11.31 125.92 ± 10.55 0.167 0.939 术后6月 132.29 ± 8.07 131.86 ± 8.78 0.204 0.831 术后12月 135.64 ± 7.32 134.56 ± 4.89 0.165 0.943 *P < 0.05。
下载: 导出CSV
-
[1] Katz J N,Arant,K R,Loeser R F. Diagnosis and treatment of hip and knee osteoarthritis:A review[J]. JAMA,2021,325(6):568-578. doi: 10.1001/jama.2020.22171 [2] Yoo M J,Shin Y E. Open wedge high tibial osteotomy and combined arthroscopic surgery in severe medial osteoarthritis and varus malalignment:Minimum 5-year results[J]. Knee Surg Relat Res,2016,28(4):270-276. doi: 10.5792/ksrr.15.075 [3] 王飞,陈百成,高石军,等. 内侧撑开和外侧闭合胫骨高位截骨术治疗膝内翻骨关节炎[J]. 中华骨科杂志,2010,30(6):558-562. doi: 10.3760/cma.j.issn.0253-2352.2010.06.005 [4] Schuster P,Schulz M,Mayer P,et al. Open-Wedge high tibial osteotomy and combined abrasion/microfracture in severe medial osteoarthritis and varus malalignment:5-year results and arthroscopic findings after 2 years[J]. Arthroscopy,2015,31(7):1279-1288. doi: 10.1016/j.arthro.2015.02.010 [5] 黄野,柳剑,王兴山,等. 胫骨高位截骨术适应证解析[J]. 中华外科杂志,2020,58(6):420-424. [6] Celik D,Coskunsu D,Kilicoglu O. Translation and cultural adaptation of the turkish lysholm knee scale:easeof use,validity,and reliability[J]. Clin Orthop Relat Res,2013,471(8):2602-2610. [7] Ben-Zikri Y K,Yaniv Z R,Baum K,et al. A marker-free registration method for standing x-ray panorama reconstruction for hip-knee-ankle axis defformity assessment[J]. Comput Methods Biomech Biomed Eng Imaging Vis,2019,7(4):464-478. [8] Yang S S,Seo T B,Kim Y P. Effect of aqua walking exercise on knee joint angles,muscular strength,and visual analogue scale for patients with limited range of motion of the knee[J]. J Exerc Rehabil,2021,17(4):265-269. [9] Stupik A,Biatoszewski D. A comparative analysis of the clinical utility of the Staffelstein-score and the hospital for special surgery knee score (HSS) in monitoring physiotherapy of total knee replacement patients--preliminary study[J]. Ortop Traumatol Rehabil,2009,11(1):37-45. [10] Sharma,L. Osteoarthritis of the knee[J]. N Engl J Med,2021,384(1):51-59. [11] Arden N K,Perry T A,Bannuru R R,et al. Non-surgical management of knee osteoarthritis:comparison of ESCEO and OARSI 2019 guidelines[J]. Nat Rev Rheumatol,2021,17(1):59-66. doi: 10.1038/s41584-020-00523-9 [12] Jung W H,Takeuchi R,Chun C W,et al. Second-look arthroscopic assessment of cartilage regeneration after medial opening-wedge high tibial osteotomy[J]. Arthroscopy,2014,30(1):72-79. [13] 黄将来. 胫骨高位截骨术治疗内翻型膝骨性关节炎的效果分析[J]. 河南医学研究,2016,25(6):1042-1043. doi: 10.3969/j.issn.1004-437X.2016.06.044 [14] Lau L C M,Fan J C H,Chung K Y,et al. Satisfactory long-term survival,functional and radiological outcomes of open-wedge high tibial osteotomy for managing knee osteoarthritis:Minimum 10-year follow-up study[J]. J Orthop Translat,2021,30(26):60-66. [15] Song J H,Bin S I,Kim J M,et al. Cartilage status,Rather than chronologic age,Determines the outcomes of open wedge high tibial osteotomy:A cartilage status-matched cohort study[J]. Arthroscopy,2021,37(9):2915-2922. doi: 10.1016/j.arthro.2021.03.075 [16] Ishimatsu T,Takeuchi R,Ishikawa H,et al. Hybrid closed wedge high tibial osteotomy improves patellofemoral joint congruity compared with open wedge high tibial osteotomy[J]. Knee Surg Sports Traumatol Arthrosc,2019,27(4):1299-1309. doi: 10.1007/s00167-019-05350-4 [17] Pape D,Dueck K,Haag M,et al. Wedge volume and osteotomy surface depend on surgical technique for high tibial osteotomy[J]. Knee Surg Sports Traumatol Arthrosc,2013,21(1):127-133. doi: 10.1007/s00167-012-1913-x [18] Akamatsu T,Kumagai K,Yamada S,et al. No differences in clinical outcomes and cartilage repair between opening wedge and closed wedge high tibial osteotomies at short-term follow-up:A retrospective case seriesanalysis[J]. J Orthop Surg(Hong Kong),2021,29(2):2309-2310. [19] Paatela T,Vasara A,Nurmi H,et al. Assessment of cartilage repair quality with the international cartilage repair society score and the oswestry copy score[J]. J Orthop Res,2020,38(3):555-562. [20] He M,Zhong X,Li Z,et al. Progress in the treatment of knee osteoarthritis with hightibial osteotomy:a systematic review[J]. Syst Rev,2021,10(1):56. doi: 10.1186/s13643-021-01601-z [21] Jin Q H,Lee W G,Song E K,et al. Comparison of long-term survival analysis between open-wedge high tibial osteotomy and unicompartmental knee Arthroplasty[J]. J Arthroplasty,2021,36(5):1562-1567. [22] 肖国庆,钟喜红,程劲,等. 关节镜治疗轻中度膝关节骨关节炎疗效分析[J]. 中国修复重建外科杂志,2011,25(6):765-766. [23] Kim C W,Lee C R,Seo S S,et al. Clinical efficacy of an arthroscopic surgery in open wedge high tibial osteotomy[J]. J Knee Surg,2017,30(4):352-358. [24] Zhu J W,Chen D S,Wang T F,et al. Analysis of com- plications after medial opening wedge high ti- bial osteotomy[J]. Zhonghua Wai Ke Za Zhi,2020,58(6):447-451. [25] 李文新. 关节镜联合胫骨高位截骨术治疗内翻型膝关节骨性关节炎的临床效果研究[J]. 中国现代医生,2017,55(29):64-66. [26] Wang Z,Zeng Y,She W,et al. Is opening-wedge high tibial osteotomy superior to closing-wedge high tibial osteotomy in treatment of unicompartmental osteoarthritis?A meta-analysis of randomized controlled trials[J]. Int J Surg,2018,60(12):153-163. -










 点击查看大图
点击查看大图
计量
- 文章访问数: 5222
- HTML全文浏览量: 3051
- PDF下载量: 20
- 被引次数: 0
