

Application of Different Assessment Methods in Cardiovascular Disease Risk Assessment of T2DM
-
摘要:
目的 分析Framinghan、ADVANCE-Risk评分表与“糖心风险评估”、“CV风险评估”模型评估对T2DM患者未来10 a心血管疾病死亡风险评估的一致性。 方法 回顾性收集昆明医科大学第二附属医院内分泌科2018年1月至2020年12月符合2型糖尿病诊断标准住院患者527例:(1)使用“糖心风险评估”模型与Framingham评分分别评估未来10 a心血管病发病风险;(2)纳入增加糖尿病病程、UACR等指标的患者148例,使用ADVANCE-Risk评分和“CV风险评估项目”,分别评估同一患者的未来10 a心血管病死亡风险。以上2组均采用Kappa值来评估2种方法结果的一致性。 结果 (1)院内风险评估模型“糖心风险评估”结果中:中危组431人(81.78%),Friminghan评分评估结果为:高危组250人(47.44%)。SPSS分析得出Kappa值,K = 0.051,P = 0.001;(2)院内风险评估模型“CV风险项目”结果中:极高危组98人(66.22%),ADVANCE-Risk模型评估结果为:极高危组76人(50%)。SPSS分析得出Kappa值,K = 0.492,P = 0.000。 结论 “糖心风险评估”模型与Framingham评分对2型糖尿病患者未来10 a心血管病发生风险的评估结果一致性差。“CV风险评估项目”和ADVANCE-Risk评分对2型糖尿病患者未来10 a心血管病死亡风险的评估结果一致性中等。 Abstract:Objective To analyze the consistency between the Framinghan, the advance-risk scale and the “sugar-heart risk assessment”, the “CV risk assessment” model on the risk of cardiovascular death in T2DM patients in the next 10 years. Methods A retrospective study of 527 inpatients who met the diagnostic criteria for type 2 diabetes in the Department of Endocrinology, The Second Affiliated Hospital of Kunming Medical University from January 2018 to December 2020 was conducted. The Framinghan rating scale and the Cardiovascular risk assessment for diabetes mellitus model were used to assess the occurrence risk of cardiovascular disease over the next 10 years. 148 patients with increased diabetes duration, UACR and other indicators were included. ADVANCE Risk score and CV Risk Assessment project were used to evaluate the risk of cardiovascular death of the same patient in the next 10 years. Kappa values were used to evaluate the consistency of the results of the two methods. Results The result of Cardiovascular risk assessment for diabetes mellitus model: 431 patients (81.78%) in the medium-risk group, and 250 patients (47.44%) in the high-risk group using Framinghan rating scale. SPSS analysis showed Kappa value, K = 0.051, P = 0.001; The result of CV Risk assessment”: 98 patients (66.22%) in the very high Risk group, and 76 patients (50%) in the ADVANCE Risk model. SPSS analysis showed Kappa value, K = 0.492, P = 0.000. Conclusion In this study, the “Cardiovascular risk assessment for diabetes mellitus” model and Framinghan rating scale in assessing the occurrence risk of cardiovascular disease in patients with type 2 diabetes in the next 10 years were very inconsistent. The “CV Risk assessment” and ADVANCE Risk model had moderate consistency in assessing the mortality risk of cardiovascular in patients with type 2 diabetes over the next 10 years. -
Key words:
- Type 2 diabetes /
- Cardiovascular disease /
- Risk assessment
-

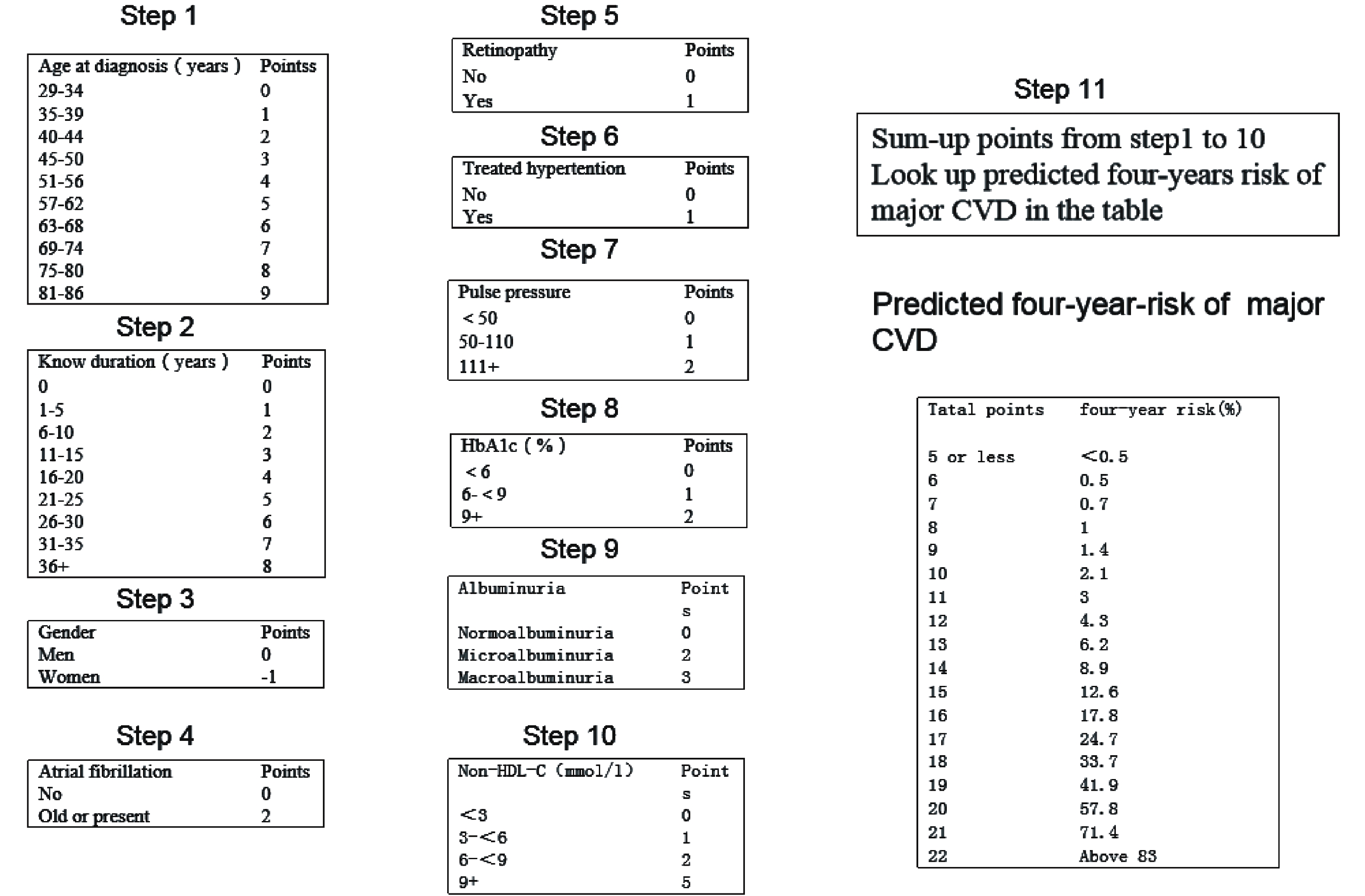
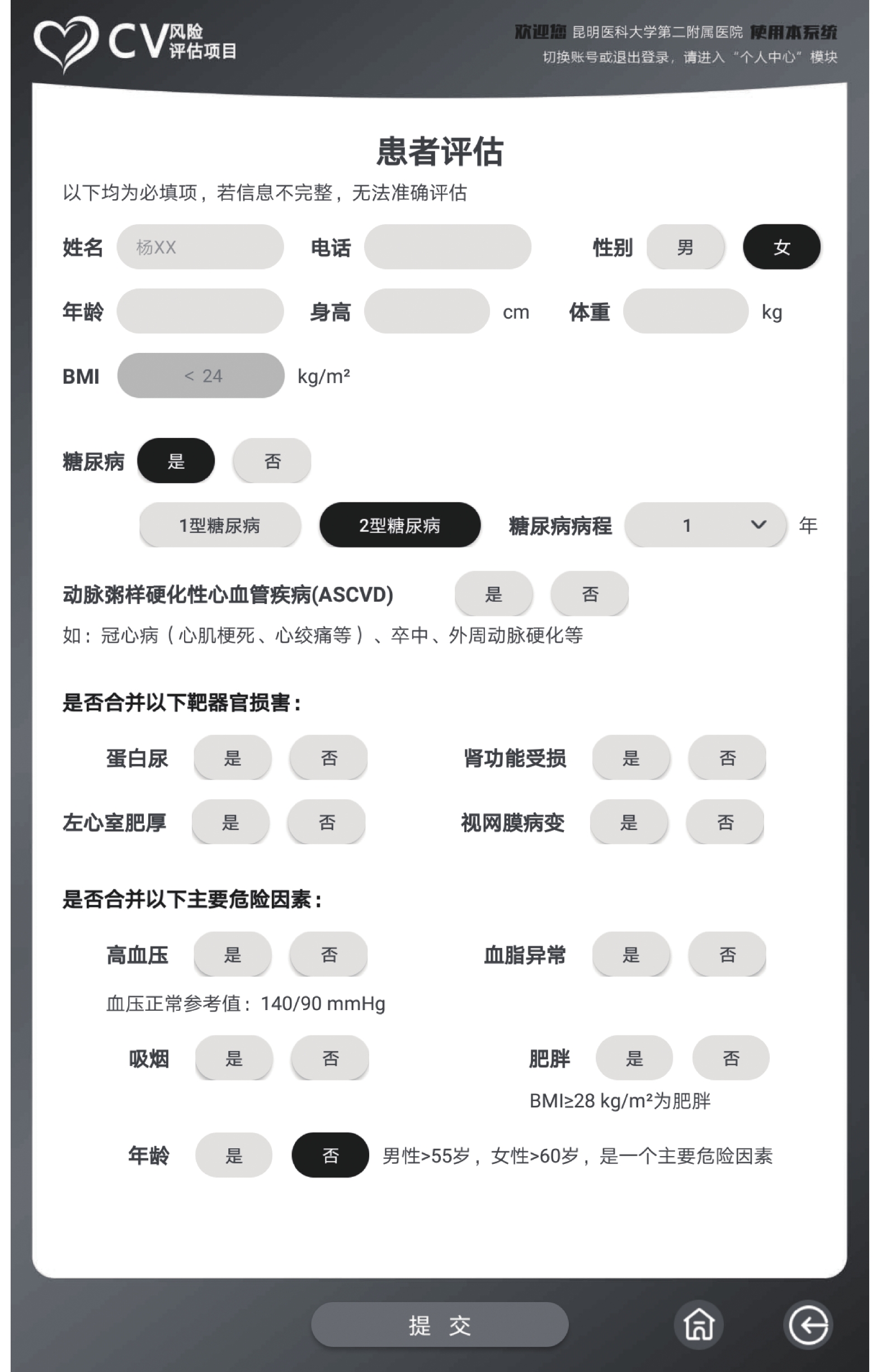
图 1 CV风险项目纳入患者的各指标图示
Figure 1. Indicators of patients included in the CV risk project are shown in the figure
表 1 女性10 a风险评估(年龄、收缩压、吸烟与否、HDL-C)(分)
Table 1. Assessment of 10-year risk for women(age,SBP,smoker or not,HDL-C)(scores)
年龄(岁) 年龄
评分收缩压
(mmHg)年龄+收缩压+
治疗评分年龄+收缩压+
未治疗评分年龄+
未吸烟评分年龄+
吸烟评分HDL-C
(mg/dL)HDL-C
评分20~34 −7 < 120 0 0 0 9 ≥60 −1 35~39 −3 40~44 0 120~129 3 1 0 7 50~59 0 45~49 3 50~54 6 130~139 4 2 0 4 40~49 1 55~59 8 60~64 10 140~159 5 3 0 2 < 40 2 65~69 12 70~74 14 ≥160 6 4 0 1 75~79 16  下载: 导出CSV
下载: 导出CSV
表 2 女性10 a风险评估(TC)
Table 2. Assessment of 10-year risk for women (TC)
年龄(岁) TC(mg/dL)
< 160评分TC(mg/dL)
160~199评分TC(mg/dL)
200~239评分TC(mg/dL)
240~279评分TC(mg/dL)
≥280评分20~39 0 4 8 11 13 40~49 0 3 6 8 10 50~59 0 2 4 5 7 60~69 0 1 2 3 4 70~79 0 1 1 2 2
下载: 导出CSV
表 3 男性10 a风险评估(年龄、收缩压、吸烟与否、HDL-C)
Table 3. Assessment of 10-year risk for men(age,SBP,smoker or not,HDL-C)
年龄(岁) 年龄
评分收缩压
(mmHg)年龄+收缩压+
治疗评分年龄+收缩压+
未治疗评分年龄+
未吸烟评分年龄+
吸烟评分HDL-C
(mg/dL)HDL-C
评分20~34 −9 < 120 0 0 0 8 ≥60 −1 35~39 −4 40~44 0 120~129 1 0 0 5 50-59 0 45~49 3 50~54 6 130~139 2 1 0 3 40-49 1 55~59 8 60~64 10 140~159 2 1 0 1 < 40 2 65~69 11 70~74 12 ≥160 3 2 0 1 75~79 13
下载: 导出CSV
表 4 男性10 a风险评估 (TC)
Table 4. Assessment of 10-year risk for men (TC)
年龄(岁) TC(mg/dL)
< 160评分TC(mg/dL)
160~199评分TC(mg/dL)
200~239评分TC(mg/dL)
240~279评分TC(mg/dL)
≥280评分20~39 0 4 7 9 11 40~49 0 3 5 6 8 50~59 0 2 3 4 5 60~69 0 1 1 2 3 70~79 0 0 0 1 1
下载: 导出CSV
表 5 10 a风险评估总分表
Table 5. Assessment of 10-year risk total score table
女性
总分女性10 a
风险,%男性
总分男性10 a
风险,%< 9 < 1 ≤0 ≤1 9 1 1 1 10 1 2 1 11 1 3 1 12 1 4 1 13 2 5 2 14 2 6 2 15 3 7 3 16 4 8 4 17 5 9 5 18 6 10 6 19 8 11 8 20 11 12 10 21 14 13 12 22 17 14 16 23 22 15 20 24 27 16 25 ≥25 ≥30 ≥17 ≥30
下载: 导出CSV
表 6 糖尿病性视网膜病变国际临床分型
Table 6. International clinical typing of diabetic retinopathy
病变 扩瞳眼底检査所见 无明显视网膜病变 无异常 轻度非増殖期视网膜病变 仅有微动脉瘤 中度非増殖期视网膜病变 微动脉瘤伴轻至重度非增殖性视网膜病变 重度非増殖期视网膜病变 出现以下任一改变,但无增殖性视网膜病变的体征: ①4个象限中每1象限出现 > 20处视网膜内出血;②在 > 2个象限出现静脉串珠样改变;③至少1象限出现明显视网膜内微血管异常 增殖性糖尿病性视网膜病变 出现1种或1种以上改变:①新生血管;②玻璃体积血或视网膜出血
下载: 导出CSV
表 7 “糖心风险评估”与Framinghan评分表结果列联表
Table 7. The results contingency tables of the "Cardiovascular risk assessment for diabetes mellitus"and the Framinghan rating scale
项目 糖心评估模型 合计 P 低危 中危 高危 Framinghan评分 低危 1 178 17 196 0.001* 中危 0 67 14 81 高危 0 185 65 250 合计 1 430 96 527 *P < 0.05。
下载: 导出CSV
表 8 “CV风险项目”与ADVANCE-Risk模型结果列联表
Table 8. The results contingency tables of the "CV Risk assessment" model and the ADVANCE-Risk model
项目 CV风险项目 合计 P 中危 高危 极高危 ADVANCE-Risk 中危 29 0 7 36 0.000* 高危 11 5 22 38 极高危 4 1 69 74 合计 44 6 98 148 *P < 0.05。
下载: 导出CSV
-
[1] Khan M A B,Hashim M J,King J K,et al. Epidemiology of type 2 diabetes - global burden of disease and forecasted trends[J]. J Epidemiol Glob Health,2020,10(1):107-111. [2] 中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2017年版)[J]. 中国实用内科杂志,2018,38(4):292-344. [3] American Diabetes Association. 9. Cardiovascular disease and risk management: Standards of medical care in diabetes-2018[J]. Diabetes Care, 2018, 41(Suppl 1): 86-104. [4] Grimaldi A,Heurtier A. Critères diagnostiques du diabète de type 2 [Diagnostic criteria for type 2 diabetes][J]. Rev Prat,1999,49(1):16-21. [5] Yang X,Li J,Hu D,et al. Predicting the 10-year risks of atherosclerotic cardiovascular disease in chinese population:The China-PAR project (prediction for ASCVD risk in China)[J]. Circulation,2016,134(19):1430-1440. doi: 10.1161/CIRCULATIONAHA.116.022367 [6] Nishimura K,Okamura T,Watanabe M,et al. Predicting coronary heart disease using risk factor categories for a Japanese Urban Population,and comparison with the Framingham risk score:The Suita Study[J]. J Atheroscler Thromb,2016,23(9):1138-1139. doi: 10.5551/jat.Er19356 [7] Expert Panel on Detection,Evaluation and treatment of high blood cholesterol in adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP)Expert Panel on Detection,Evaluation and treatment of high blood cholesterol in adults (Adult Treatment Panel III)[J]. JAMA,2001,285(19):2486-2497. doi: 10.1001/jama.285.19.2486 [8] 孙宁玲,施仲伟,霍勇. 高血压合并左心室肥厚诊治专家共识[J]. 中华心血管病杂志(网络版),2019,2(1):5. [9] 廖二元, 袁凌青, 谢忠建, 等. 内分泌代谢病学[M]. 北京: 人民卫生出版社, 2019: 1571. [10] 诸骏仁,高润霖,赵水平,等. 中国成人血脂异常防治指南(2016年修订版)[J]. 中华健康管理学杂志,2017,11(1):7-28. doi: 10.3760/j.issn.1674-0815.2017.01.003 [11] 中国心血管病预防指南(2017)写作组,中华心血管病杂志编辑委员会. 中国心血管病预防指南(2017)[J]. 中华心血管病杂志,2018,46(01):10-25. doi: 10.3760/cma.j.issn.0253-3758.2018.01.004 [12] Kengne A P. The ADVANCE cardiovascular risk model and current strategies for cardiovascular disease risk evaluation in people with diabetes[J]. Cardiovasc J Afr,2013,24(9-10):376-381. [13] Kengne A P,Patel A,Marre M,et al. Contemporary model for cardiovascular risk prediction in people with type 2 diabetes[J]. Eur J Cardiovasc Prev Rehabil,2011,18(3):393-398. doi: 10.1177/1741826710394270 [14] Zheng Y,Ley S H,Hu F B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications[J]. Nat Rev Endocrinol,2018,14(2):88-98. doi: 10.1038/nrendo.2017.151 [15] De Meyer T,Nawrot T,Bekaert S,et al. Telomere length as cardiovascularagingbiomarker:JACC review topic of the week[J]. J Am Coll Cardiol,2018,72(7):805-813. doi: 10.1016/j.jacc.2018.06.014 [16] Wada H,Miyauchi K,Daida H. Gender differences in the clinical features and outcomes of patients with coronary artery disease[J]. Expert Rev Cardiovasc Ther,2019,17(2):127-133. doi: 10.1080/14779072.2019.1561277 [17] Choi Y J,Kim S H,Kang S H,et al. Reconsidering the cut-off diastolic blood pressure for predicting cardiovascular events:A nationwide population-based study from Korea[J]. Eur Heart J,2019,40(9):724-731. doi: 10.1093/eurheartj/ehy801 [18] Østergaard H B,Mandrup Poulsen T,Berkelmans G F N,et al. Limited benefit of haemoglobin glycation index as risk factor for cardiovascular disease in type 2 diabetes patients[J]. Diabetes Metab,2019,45(3):254-260. doi: 10.1016/j.diabet.2018.04.006 [19] Cooney M T,Selmer R,Lindman A,et al. Cardiovascular risk estimation in older persons:SCORE O. P[J]. Eur J Prev Cardiol,2016,23(10):1093-1103. doi: 10.1177/2047487315588390 [20] Brownrigg J R,Hughes C O,Burleigh D,et al. Microvascular disease and risk of cardiovascular events among individuals with type 2 diabetes:A population-level cohort study[J]. Lancet Diabetes Endocrinol,2016,4(7):588-597. doi: 10.1016/S2213-8587(16)30057-2 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3749
- HTML全文浏览量: 1936
- PDF下载量: 28
- 被引次数: 0
