

Interrupted Vertical Non-Absorbable Sutures Combined with Nis Knots in the Treatment of Inferior Pole Patella Fractures
-
摘要:
目的 探讨间断垂直不可吸收缝线联合尼斯结治疗髌骨下极骨折的技术要点及疗效。 方法 选取云南大学附属医院骨与创伤外科2016年01月至2020年12月收治髌骨下极骨折共22例行间断垂直不可吸收缝线联合尼斯结治疗患者(观察组),同时选取同期行克氏针钢丝张力带治疗的患者21例(对照组),阐述技术要点并根据各项指标综合评估临床疗效。 结果 (1)观察组手术时间、术中出血量、骨折愈合时间均明显短于对照组(P < 0.05);(2)观察组膝关节活动度(术后1、3、6月)均大于对照组(P < 0.05);观察组Lysholm评分(术后1、3、6、12月)、KSS评分(术后1、3、6月)均高于对照组(P < 0.05);(3)观察组无1例出现膝前疼痛,而对照组有12例;随访终末期膝关节Bostman评分优良率(100%)观察组显著高于对照组(95.23%)。 结论 间断垂直不可吸收缝线联合尼斯结治疗髌骨下极骨折避免了金属材料的使用,软组织激惹少,操作简单易行、耗时短、出血量少、固定牢靠,术后功能恢复好,远期内置物无需二次手术取出,有极佳的临床应用价值。 Abstract:Objective To Explore the technical points and clinical efficacy of interrupted vertical non-absorbable sutures combined with nis knots in the treatment of inferior patellar pole fractures. Methods A total of 22 patients admitted to the Department of Bone and Trauma Surgery of the Affiliated Hospital of Yunnan University from January 2016 to December 2020 with intermittent vertical non-absorbable sutures combined with nice knot treatment for inferior pole patella fractures were selected as the observation group, while 21 patients who were treated with a wire tension band with a knot needle at the same time were selected as the control group, and the technical points were elaborated and the clinical efficacy was comprehensively evaluated according to the index of each group. Results (1)The operating time, intraoperative bleeding and fracture healing time in the observation group were significantly shorter than those in the control group(P < 0.05). (2) Knee mobility(1, 3, and 6 months after the surgery) was greater in the observation group than that in the control group(P < 0.05); Lysholm score(1, 3, 6, and 12 months after the surgery) and KSS score(1, 3, and 6 months after thesurgery) were higher in the observation group than those in the control group(P < 0.05); (3) None of the cases in the observation group had anterior knee pain, while there were 12 cases in the control group; End-stage knee at follow-up Bostman score excellent rate(100%) was significantly higher in the observation group than that in the control group(95.23%). Conclusion Intermittent vertical non-absorbable sutures in combination with nis knots for the treatment of inferior pole patella fractures can avoid the use of metallic materials, have the advantages of less soft tissue irritation, simple and easy operation, short time-consuming, less bleeding, firm fixation, good postoperative functional recovery. Therefore, there is no need for the secondary operation to remove the long-term implant and have the excellent clinical application value. -
Key words:
- Inferior pole patella fracture /
- Non-absorbable suture /
- Nice knot /
- Tension band
-

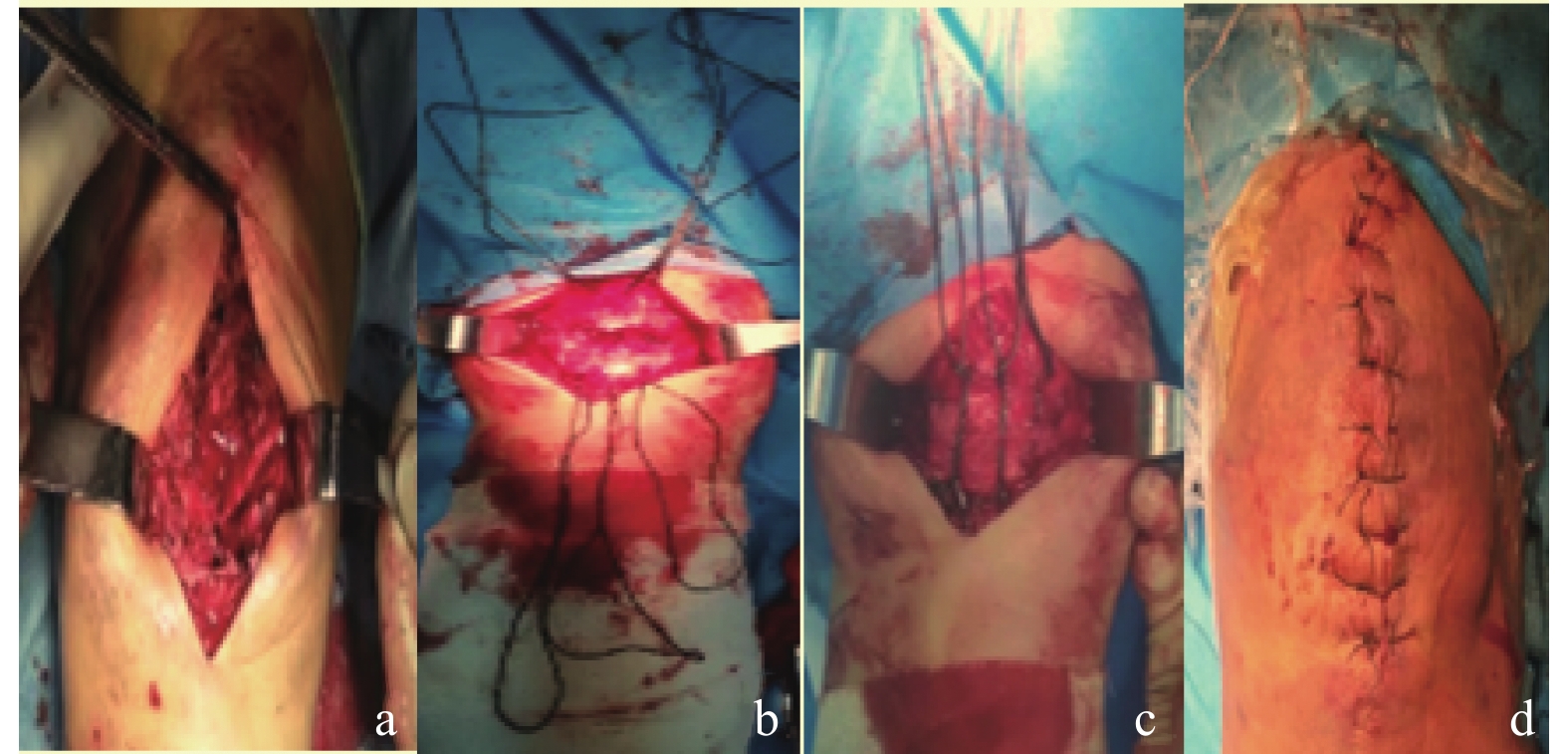
图 1 间断垂直不可吸收缝线结合Nice Knot技术治疗髌骨下极骨折示意图
a: 采用膝前正中纵形切口,暴露髌骨骨折端;b:不可吸收缝线分别于骨孔道穿出;c: 拉紧缝线使髌骨下极骨折块复位,尼斯结技术进行缝线打结;d:间断缝合关闭切口。
Figure 1. Fig. 1 Schematic diagram of an interrupted vertical non-absorbable suture combined with the Nice Knot technique for the treatment of a fracture of the lower pole of the patella

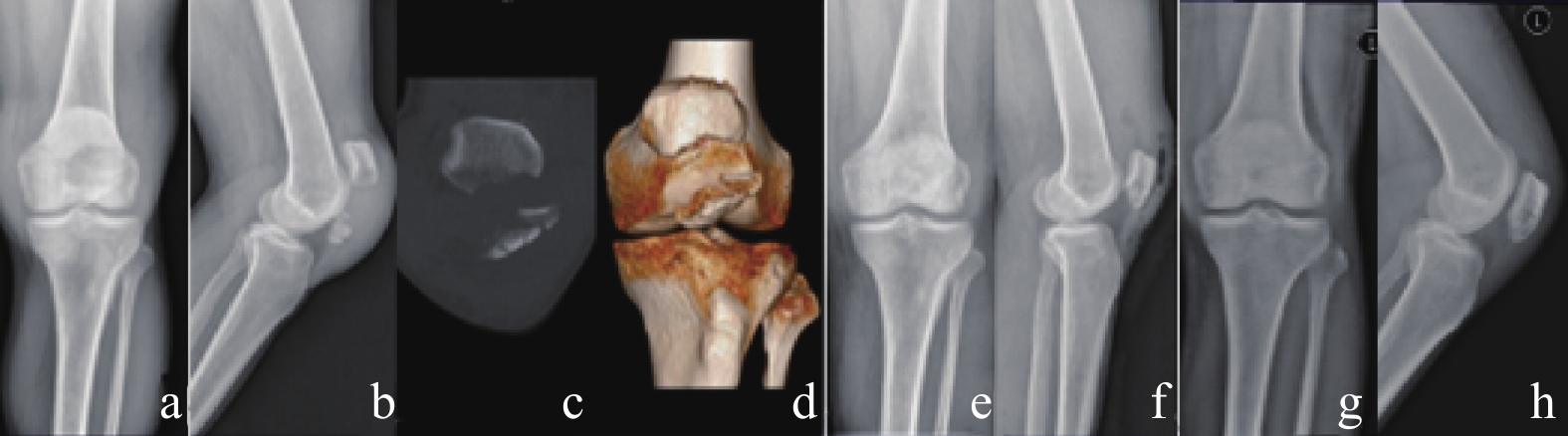
图 2 患者,男,47岁,摔伤致左髌骨下极骨折,采用间断垂直不可吸收缝线联合尼斯结治疗
a、b:术前X线片示髌骨下极骨折;c、d:术前CT及三维重建,可见髌骨下极骨折粉碎严重;e、f:术后复查X线片示骨折对位、对线良好,髌骨关节面平整;g、h:术后3个月复查X线片示骨折线模糊。
Figure 2. Patient,male,47 years old,with a fall resulting in a fracture of the lower pole of the left patella,treated with interrupted vertical non-absorbable sutures combined with the nice knots

图 3 患者术后3个月复查的膝关节功能位图像
Figure 3. Functional knee images of the patient,reviewed 3 months after surgery
表 1 2组患者一般资料比较[(
$ \bar x \pm s $ )/n]Table 1. Comparison of general information of patients between 2 groups [(
$ \bar x \pm s $ )/n]组别 n 性别(男/女) 平均年龄(岁) 骨折部位(左/右) 受伤原因(跌伤/其他伤) 受伤至手术时间(d) 观察组 22 13/9 49.00 ± 6.10 10/12 15/7 3.81 ± 1.00 对照组 21 15/6 48.32 ± 5.70 13/8 17/4 3.85 ± 1.04 χ2/t − 0.720 0.380 1.169 0.920 −0.064 P − 0.396 0.706 0.280 0.337 0.949  下载: 导出CSV
下载: 导出CSV
表 2 2组患者相关临床指标比较(
$ \bar x \pm s $ )Table 2. Comparison of relevant clinical indicators between the 2 groups of patients (
$ \bar x \pm s $ )组别 n 手术时间(min) 术中出血量(mL) 骨折愈合时间(周) 观察组 22 52.08 ± 6.27 87.13 ± 3.38 7.32 ± 0.51 对照组 21 64.90 ± 4.90 91.86 ± 3.93 7.86 ± 0.53 t − −7.444 −4.233 −3.404 P − < 0.001* < 0.001* 0.001* *P < 0.05。
下载: 导出CSV
表 3 2组患者术后1、3、6、12月膝关节活动度比较[(
$ \bar x \pm s $ ),°]Table 3. Comparison of knee mobility between 2 groups of patients at 1,3,6 and 12 months after surgery [(
$ \bar x \pm s $ ),°]组别 n 术后膝关节活动度(°) 1月 3月 6月 12月 观察组 22 79.90 ± 2.53 94.18 ± 5.16 124.84 ± 1.84 131.37 ± 1.70 对照组 21 74.37 ± 3.14 89.25 ± 5.83 121.75 ± 3.67 130.55 ± 1.66 t − 6.363 2.935 3.515 1.612 P − < 0.001* 0.005* 0.001* 0.115 *P < 0.05。
下载: 导出CSV
表 4 2组患者术后1、3、6、12月膝关节Lysholm评分比较[(
$ \bar x \pm s $ ),分]Table 4. Comparison of Lysholm scores of knee joint in 2 groups of patients at 1,3,6 and 12 months after surgery[(
$ \bar x \pm s $ ),Points]组别 n 术后Lysholm评分 1月 3月 6月 12月 观察组 22 69.01 ± 4.94 73.11 ± 2.99 82.14 ± 4.82 91.08 ± 2.26 对照组 21 57.95 ± 1.87 66.92 ± 2.93 76.86 ± 3.81 83.52 ± 1.29 t − 9.608 6.839 3.972 13.359 P − < 0.001* < 0.001* < 0.001* < 0.001* *P < 0.05。
下载: 导出CSV
表 5 2组患者术后1、3、6、12月膝关节KSS评分比较[(
$ \bar x \pm s $ ),分]Table 5. Comparison of KSS scores of knee joint in 2 groups of patients at 1,3,6 and 12 months after surgery[(
$ \bar x \pm s $ ),Points]组别 n 术后KSS评分 1月 3月 6月 12月 观察组 22 70.01 ± 4.45 75.11 ± 3.94 81.72 ± 2.87 90.59 ± 3.00 对照组 21 65.63 ± 1.76 71.15 ± 2.56 76.07 ± 2.97 89.02 ± 2.44 t − 4.209 3.893 6.380 1.870 P − < 0.001* < 0.001* < 0.001* 0.069 *P < 0.05。
下载: 导出CSV
表 6 2组患者随访终末期膝关节功能Bostman评分比较[n(%)]
Table 6. Comparison of Bostman scores for end-stage knee function at follow-up between the 2 groups[n(%)]
组别 n 优 良 差 优良率 观察组 22 20 2 0 22(100) 对照组 21 18 2 1 20(95.23) 膝关节Bostman评分:满分30分,其中28~30分为优,20~27分为良,< 20分为差。
下载: 导出CSV
-
[1] Larsen P,Court-Brown C M,Vedel J O,et al. Incidence and epidemiology of patellar fractures[J]. Orthopedics,2016,39(6):e1154-e1158. [2] 鲁秋东,张翠菊. 深浅双骨道钢丝环扎联合克氏针内固定治疗髌骨下极骨折的疗效观察[J]. 中国骨与关节损伤杂志,2019,34(10):1076-1078. doi: 10.7531/j.issn.1672-9935.2019.10.024 [3] Ruedi T P, AO principles of fracture management[M]. 2. Shanghai: Shanghai Science and Technology Press, 2010: 598. [4] 白晓东,芦重尧,张英泽. 等. 髌骨骨折的内固定治疗进展[J]. 河北医科大学学报,2020,41(7):865-868. [5] Kadar A,Sherman H,Drexler M,et al. Anchor suture fixation of distal pole fractures of patella:Twenty-seven cases and comparison to partial patellectomy[J]. Int Orthop,2016,40(1):149-154. doi: 10.1007/s00264-015-2776-9 [6] Oh H K,Choo S K,Kim J W,et al. Internal fixation of displaced inferior pole of the patella fractures using vertical wiring augmented with Krachow suturing[J]. Injury,2015,46(12):2512-2515. doi: 10.1016/j.injury.2015.09.026 [7] 孙海波,周君琳,张万龙,等. 钛缆环扎联合8字减张带治疗髌骨下极粉碎性骨折[J]. 实用骨科杂志,2015,21(3):217-219. [8] 徐润冰,何双华,车坚,等. 髌爪联合钢丝和可吸收线治疗髌骨骨折的疗效观察[J]. 中国骨与关节损伤杂志,2014,29(1):81-82. [9] Ng W M,Al-Fayyadh M Z M,Kho J,et al. Crossing suture technique for the osteochondral frac tures repair of patella[J]. Arthrosc Tech,2017,6(4):e1035-e1039. doi: 10.1016/j.eats.2017.03.020 [10] Camarda L,Morello S,Balistreri F,et al. Non-metallic implant for patellar fracture fixation:A systematic review[J]. Injury,2016,47(8):1613-1617. doi: 10.1016/j.injury.2016.05.039 [11] Böstman O. Kiviluoto O,Nirhamo J. Comminuted displaced fractures of the patella[J]. In jury,1981,13(3):196-202. [12] Kim K S,Suh D W,Park S E,et al. Suture anchor fixation of comminuted inferior pole patella fracture-novel technique:Suture bridge anchor fixation technique[J]. Arch Orthop Trauma Surg,2021,141(11):1889-1897. doi: 10.1007/s00402-020-03671-5 [13] 孙彬,张志山,周方,等. 新型张力带系统治疗髌骨下极粉碎性骨折[J]. 北京大学学报,2015,47(2):272-275. [14] Taylor B C,Mehta S,Castaneda J,et al. Plating of patella fractures:Techniques and outcomes[J]. J Orthop Trauma,2014,28(9):e231-e235. doi: 10.1097/BOT.0000000000000039 [15] 赵宇,代风波,林德涛,等. Krackow缝合髌韧带结合钢丝环扎治疗髌骨下极骨折[J]. 临床骨科杂志,2020,23(5):643. doi: 10.3969/j.issn.1008-0287.2020.05.012 [16] Wessels M,Hekman E E,Kruyt M C,et al. Spinal shape modulation in a porcine model by a highly flexible and extendable non-fusion implant system[J]. Eur Spine J,2016,25(9):2975-2983. doi: 10.1007/s00586-016-4570-9 [17] He S,Huang X,Yan B,et al. Modified technique of separate vertical wiring for the fixation of patellar inferior pole fracture[J]. J Orthop Trauma,2018,32(4):e145-e150. doi: 10.1097/BOT.0000000000001080 [18] 潘明芒,薛锋,唐果. 等. 不同类型髌骨下极骨折的手术治疗[J]. 中国矫形外科杂志,2016,24(8):745-747. [19] Fan M,Wang D,Sun K,et al. Study of double button plate fixation in treatment of inferior pole of patella fracture[J]. Injury,2020,51(3):774-778. doi: 10.1016/j.injury.2020.01.031 [20] Yang T Y,Huang T W,Chuang P Y,et al. Treatment of displaced transverse fractures of the patella:Modified tension band wiring technique with or without augmented circumferential cerclage wire fixation[J]. BMC Musculoskelet Disord,2018,19(1):167. doi: 10.1186/s12891-018-2092-9 [21] 李旭,李石伦,李升,等. 全切术和部分切除术对髌骨粉碎性骨折的远期疗效比较[J]. 河北医药,2020,42(12):1809-1812. doi: 10.3969/j.issn.1002-7386.2020.12.011 [22] Gwinner C,Märdian S,Schwabe P,et al. Current concepts review:Fractures of the patella[J]. GMS Interdiscip Plast Reconstr Surg DGPW,2016,18(1):2-6. [23] Boileau P,Alami G,Rumian A,et al. The doubled-suture nice knot[J]. Orthope dics,2017,40(2):e382-e386. [24] Swensen S,Fisher N,Atanda A,et al. Suture repair of a pole patella fracture[J]. J Orthop Trauma,2017,31(3):28-29. doi: 10.1097/BOT.0000000000000901 [25] Adjal J,Ban I. Patella fractures treated with suture tension band fixation[J]. J Orthop Surg Res,2021,16(1):179. doi: 10.1186/s13018-021-02309-5 [26] Boileau P,Pennington S D,Alami G. Proximal humeral fractures in younger patients:Fixation techniques and arthroplasty[J]. J Shoulder Elbow Surg,2011,20(2):S47-S60. doi: 10.1016/j.jse.2010.12.006 [27] Collin P,Laubster E,Denard P J,et al. The Nice knot as an improvement on current knot options:A mechanical analysis[J]. Orthop Traumatol Surg Res,2016,102(3):293-296. doi: 10.1016/j.otsr.2016.01.005 [28] Chen M,Jin X,Fryhofer G W,et al. The application of the nice knots as an auxiliary reduction technique in displaced comminuted patellar fractures[J]. Injury,2020,51(2):466-472. doi: 10.1016/j.injury.2019.12.005 [29] Hill S W,Chapman C R,Adeeb S,et al. Biomechanical evaluation of the nice knot[J]. Int J Shoul der Surg,2016,10(1):15-20. doi: 10.4103/0973-6042.174513 [30] 付中国. Nice Knot方法在肱骨近端骨折假体置换术大小结节固定修复中的应用[J]. 中华肩肘外科电子杂志,2013,1(1):65-69. -












 点击查看大图
点击查看大图
计量
- 文章访问数: 2680
- HTML全文浏览量: 1963
- PDF下载量: 29
- 被引次数: 0
