

Predictive Value of RDW and Blood Lipid on Gastroesophageal Variceal Bleeding in Patients with Liver Cirrhosis
-
摘要:
目的 探讨红细胞分布宽度(red cell distribution width, RDW)及血脂与肝硬化伴食管胃底静脉曲张破裂出血(gastroesophageal variceal bleeding, GEVB)的相关性及临床价值。 方法 以昆明市第三人民医院肝病综合科2021年1月至2021年5月期间收治住院的发生GEVB的肝硬化患者60例为出血组,随机选取同期住院的未发生GEVB的肝硬化患者60例为未出血组。对比分析2组患者的基本资料、RDW、PLT、肝功能生化指标和血脂相关指标,然后通过多因素二元Logistic回归分析探索RDW和血脂对GEVB的影响,最后用ROC曲线判断其诊断效能。 结果 与未出血组相比,出血组RDW升高,TG、TC、HDL-C、LDL-C、ApoA1、ApoE降低(均P < 0.05)。二元Logistic回归分析提示,RDW是肝硬化患者发生GEVB的独立危险因素(OR = 1.367, 95%CI:1.141~1.639),TC是肝硬化患者发生GEVB的独立保护因素(OR = 0.437, 95%CI: 0.262~0.728)(均P < 0.05)。通过绘制ROC曲线提示,RDW诊断GEVB的曲线下面积(AUC)为0.803(P < 0.05),最佳临界值15.25%,敏感度为86.7%、特异性为63.3%;TC诊断GEVB的AUC为0.789(P < 0.05),最佳临界值2.765 mmol/L,敏感度为78.3%、特异性为75.0%。 结论 RDW及TC对于肝硬化患者发生GEVB具有较高的判断价值,临床需高度重视。 -
关键词:
- 肝硬化 /
- 食管胃底静脉曲张破裂出血 /
- 红细胞分布宽度 /
- 血脂
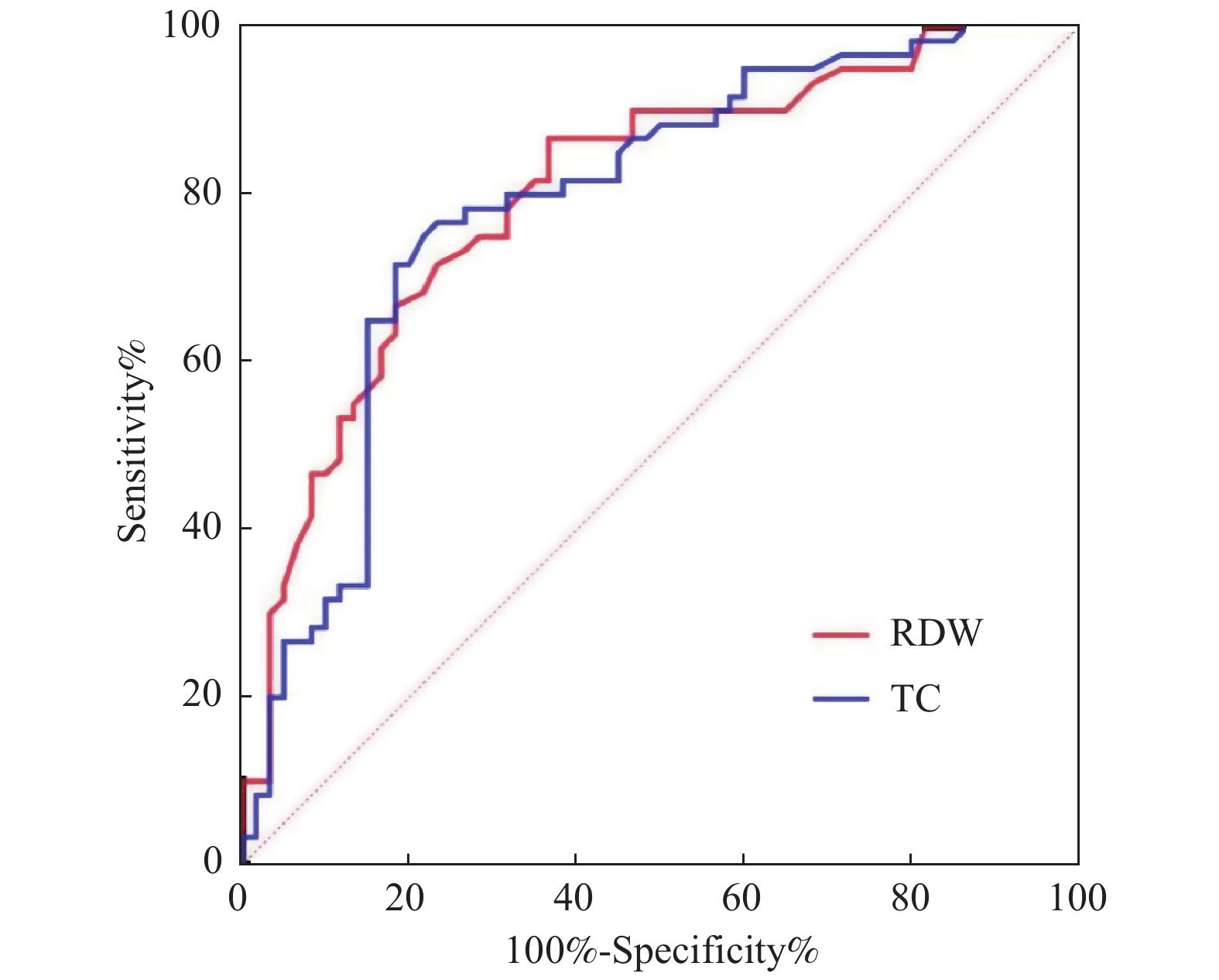
Abstract:Objective To explore the correlation between the red blood cell distribution width (RDW) / lipids and gastroesophageal variceal bleeding (GEVB) in patients with liver cirrhosis. Methods A total of 60 GEVB patients admitted to the Comprehensive Hepatology Department of the Third People’s Hospital of Kunming from January, 2021 to May, 2021 were assigned to the bleeding group, meanwhile, another 60 liver cirrhosis patients without GEVB were randomly selected as the non-bleeding group. The basic data, RDW, PLT, biochemical indexes of liver function and blood lipid related indexes of the two groups were compared, and then the effects of RDW and blood lipid on GEVB were explored through multivariate binary logistic regression analysis. Finally, ROC curves were used to assess the diagnostic effectiveness. Results Compared with the non-bleeding group, RDW in the bleeding group increased significantly, while TG, TC, HDL-C, LDL-C, ApoA1 and ApoE decreased significantly (all P < 0.05). Binary logistic regression analysis showed that RDW was an independent risk factor (OR = 1.367, 95%CI: 1.141~1.639) while TC was the protective factor (OR = 0.437, 95%CI: 0.262~0.728) for GEVB in patients with liver cirrhosis (all P < 0.05). For RDW, the area under curve (AUC) of ROC was 0.803 (P < 0.05), optimum threshold was 15.25%, sensitivity and specificity were 86.7% and 63.3%, respectively; and for TC, AUC of ROC was 0.789 (P < 0.05), optimum threshold was 2.765 mmol/L and the sensitivity and specificity were 78.3% and 75.0%, respectively. Conclusion RDW and TC have the high value in the diagnosis of GEVB in patients with liver cirrhosis, to which intensive attention should be paid clinically. -

图 1 RDW和TC诊断肝硬化伴GEVB的ROC曲线
Figure 1. ROC curve of RDW and TC in the diagnosis of liver cirrhosis with GEVB
表 1 出血组与未出血组基本资料比较[
$\bar x \pm s$ /n(%)/M(P25,P75)]Table 1. Comparison of basic data between bleeding group and non bleeding group[
$\bar x \pm s$ /n(%)/M(P25,P75)]项目 出血组(n=60) 未出血组(n=60) χ2/t/U P 年龄(岁) 48.75 ± 8.75 51.73 ± 1.733 −1.674 0.097 性别 44/16 39/21 0.977a 0.323 男性 44 (73.33) 39 (65.00) 女性 16 (26.67) 21 (35.00) 吸烟 30(50.00) 32(53.33) 0.133a 0.715 饮酒 28(46.67) 24(40.00) 0.543a 0.461 RDW (%) 18.15(15.93~19.9) 14.45(13.43~16.6) 708.00 < 0.001* PLT (×109/L) 73.00(65.25~98.00) 73.00(52.00~95.50) 1795.50 0.981 TBIL (μmol/L) 26.00(16.90~40.98) 30.65(20.93~64.43) 144.05 0.059 AST (U/L) 43.00(27.25~73.50) 42.50(29.00~74.25) 1684.50 0.544 ALT (U/L) 28.50(17.25~50.25) 32.00(22.00~53.00) 1632.00 0.378 ALB (g/L) 29.25(23.38~34.00) 34.30(27.13~41.63) 1172.50 0.001* CHE (U/L) 2387.50(2014.25~3573) 4162.50(2546.75~6096.00) 950.50 < 0.001* TG (mmol/L) 0.66(0.49~0.93) 0.81(0.54~1.26) 1408.00 0.040* TC (mmol/L) 2.40(1.67~2.77) 3.34(2.8~4.23) 758.00 < 0.001* HDL-C (mmol/L) 0.65(0.46~0.92) 1.07(0.79~1.35) 976.50 < 0.001* LDL-C (mmol/L) 1.40 ± 0.54 1.92 ± 0.70 −4.531 < 0.001* ApoA1 (g/L) 0.82 ± 0.26 1.11 ± 0.47 −4.234 < 0.001* ApoE (mg/L) 37.75(29.35~45.8) 42.6(30.85~78.55) 1356.50 0.020* *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 肝硬化伴GEVB的相关因素分析
Table 2. Analysis of related factors of liver cirrhosis with GEVB
自变量 B S.E. Wald DF P OR OR的95% CI 下限 上限 RDW (%) 0.313 0.092 11.463 1 0.001* 1.367 1.141 1.639 TC(mmol/L) −0.828 0.260 10.128 1 0.001* 0.437 0.262 0.728 *P < 0.05。
下载: 导出CSV
-
[1] 方园,沈翔,张慧. 肝硬化门脉高压所致食管胃底静脉曲张破裂出血的影响因素分析[J]. 肝脏,2020,25(6):607-610. doi: 10.3969/j.issn.1008-1704.2020.06.018 [2] 王汝刚,张伟,李晓栋. 肝硬化合并消化道出血患者的临床影响因素分析[J]. 中国当代医药,2016,23(4):20-22. [3] Lou Y,Wang M,Mao W. Clinical usefulness of measuring red blood cell distribution width in patients with hepatitis B[J]. PLoS One,2012,7(5):e37644. doi: 10.1371/journal.pone.0037644 [4] Turcato G,Serafini V,Dilda A,et al. Red blood cell distribution width independently predicts medium-term mortality and major adverse cardiac events after an acute coronary syndrome[J]. Ann Transl Med,2016,4(13):254. doi: 10.21037/atm.2016.06.35 [5] Ma Y X,Li Z K,Chen L,et al. Blood lipid levels,statin therapy and the risk of intracerebral hemorrhage[J]. Lipids Health Dis,2016,15(1):43. doi: 10.1186/s12944-016-0213-8 [6] Leonard C E,Brensinger C M,Bilker W B,et al. Gastrointestinal bleeding and intracranial hemorrhage in concomitant users of warfarin and antihyperlipidemics[J]. Int J Cardiol,2017,228(1):761-770. [7] Kucera M,Balaz D,Kruzliak P,et al. The effects of atorvastatin treatment on the mean platelet volume and red cell distribution width inpatients with dyslipoproteinemia and comparison with plasma atherogenicity indicators-A pilot study[J]. Clin Biochem,2015,48(9):557-561. doi: 10.1016/j.clinbiochem.2015.02.010 [8] 中华医学会肝病学分会. 肝硬化诊治指南[J]. 临床肝胆病杂志,2019,35(11):2408-2416. doi: 10.3969/j.issn.1001-5256.2019.11.006 [9] 中华医学会肝病学分会,中华医学会消化病学分会,中华医学会内镜学分会. 肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J]. 临床肝胆病杂志,2016,32(2):203-219. doi: 10.3969/j.issn.1001-5256.2016.02.002 [10] GBD 2017 Cirrhosis Collaborators. The global,regional,and national burden of cirrhosis by cause in 195 countries and territories,1990-2017:A systematic analysis for the Global Bur-den of Disease Study 2017[J]. Lancet Gastroenterol Hepatol,2020,5(3):245-266. doi: 10.1016/S2468-1253(19)30349-8 [11] 李海深,宗慧丽. 食管胃底静脉曲张破裂出血患者红细胞分布宽度、谷胱甘肽过氧化物酶、过氧化脂质的变化及其临床意义[J]. 临床与病理杂志,2020,40(4):863-867. doi: 10.3978/j.issn.2095-6959.2020.04.009 [12] Lee K R,Park S O,Kim S Y,et al. Red cell distribution width as a novel marker for predicting high-risk from upper gastro-intestinal bleeding patients[J]. PLoS One,2017,12(11):e0187158. doi: 10.1371/journal.pone.0187158 [13] 孙喜斌,张玉虹,左路广,等. 血清IL-6与红细胞分布宽度联合检测对上消化道再出血的预测价值[J]. 山东医药,2020,60(19):50-53. doi: 10.3969/j.issn.1002-266X.2020.19.013 [14] 赵海燕,杨东,刘瑞霞,等. 红细胞分布宽度在乙型肝炎肝硬化失代偿及并发消化道出血中的临床价值[J]. 中华传染病杂志,2019,37(10):610-615. [15] 阮晓霞. 血脂异常与脏器出血的研究进展[J]. 心血管病学进展,2015,36(2):176-179. doi: 10.3969/j.issn.1004-3934.2015.02.014 [16] Hrabovsky V,Blaha V,Hyspler R,et al. Changes in cholesterol metabolism during acute upper gastrointestinal bleeding:Liver cirrhosis and non cirrhosis compared[J]. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub,2019,163(3):253-258. doi: 10.5507/bp.2018.055 [17] Xing G H,Wang L L,Li W,et al. Decreased serum monocyte chemoattractant protein-1 (MCP-1) expression in patients with upper gastrointestinal bleeding[J]. Med Sci Monit,2019,25(10):1822-1827. [18] 高境蔚,李罗红,欧艳,等. 肝硬化患者食管胃底静脉曲张破裂出血与血脂水平相关性分析[J]. 标记免疫分析与临床,2020,27(2):200-205. [19] 任家荣,赖平波,廖翠屏. 血清总胆固醇含量与食管胃底静脉曲张破裂出血的相关性探讨[J]. 现代医药卫,2011,27(6):833-834. [20] 阮晓霞. 急性消化道出血与血脂水平相关性的研究[D]. 重庆: 重庆医科大学硕士学位论文, 2016 . [21] Wang J,Huang R,Yan X,et al. Red blood cell distribution width:A promising index for evaluating the severity and long-term prognosis of hepatitis B virus-related diseases[J]. Dig Liver Dis,2020,52(4):440-446. doi: 10.1016/j.dld.2019.12.144 [22] Zhu M,Han M,Xiao X,et al. Dynamic differences of red cell distribution width levels contribute to the differential diagnosis of hepatitis B virus-related chronic liver diseases:A case-control study[J]. Int J Med Sci,2019,16(5):720-728. doi: 10.7150/ijms.31826 [23] Feng R,Guo X,Kou Y,et al. Association of lipid profile with decompensation,liver dysfunction,and mortality in patients with liver cirrhosis[J]. Postgrad Med,2021,133(6):626-638. doi: 10.1080/00325481.2021.1930560 -



 点击查看大图
点击查看大图
图(1) / 表(2)
计量
- 文章访问数: 3460
- HTML全文浏览量: 2374
- PDF下载量: 26
- 被引次数: 0
