

Effect of Matrix Radiofrequency Combined with Biofeedback Electrical Stimulation on Uterine Prolapse
-
摘要:
目的 探讨妇科射频联合生物反馈电刺激对子宫脱垂的临床疗效。 方法 选取符合纳入标准的患者150例,随机分为对照组和观察组,对照组予盆底生物反馈电刺激治疗,观察组予盆底生物反馈电刺激+妇科射频治疗,对2组患者治疗前后子宫脱垂程度、盆底肌功能进行评价。 结果 观察组、对照组治疗后子宫脱垂程度平均值均高于治疗前(P < 0.05),观察组治疗治疗后子宫脱垂程度平均值高于对照组(P < 0.05);观察组、对照组治疗后盆底肌功能平均值均高于治疗前(P < 0.05),观察组治疗后盆底肌功能平均值高于对照组(P < 0.05)。 结论 妇科射频联合生物反馈电刺激对子宫脱垂的治疗优于传统的生物反馈电刺激。 Abstract:Objective To investigate the clinical effect of gynecological RF combined with biofeedback electrical stimulation on uterine prolapse. Methods A total of 150 patients who met the inclusion criteria were randomly divided into control group and observation group. The control group received pelvic floor biofeedback electrical stimulation, and the degree of uterine prolapse and pelvic floor muscle function before and after treatment were evaluated. Results The mean degree of uterine prolapse in the observation group and control group was higher than before treatment (P < 0.05), and the mean degree was higher than in the control group (P < 0.05), which was higher than before treatment (P < 0.05), and higher than in the control group (P < 0.05). Conclusion The treatment of uterine prolapse combined with biofeedback electrical stimulation is better than the conventional biofeedback electrical stimulation. -
Key words:
- RF treatment /
- Biofeedback for electrical stimulation /
- Uterine prolapse
-
表 1 2组基本情况比较(
$\bar x \pm s $ )Table 1. Basic information comparison between the two groups (
$\bar x \pm s $ )组别 n 年龄(岁) 产次(次) 阴道分娩次数(次) 剖宫产分娩次数(次) 观察组 72 34.11 ± 5.68 1.53 ± 0.581 1.33 ± 0.77 0.22 ± 0.54 对照组 68 32.22 ± 6.94 1.25 ± 0.61 0.94 ± 0.81 0.32 ± 0.56 P 0.14 0.735 0.633 0.902  下载: 导出CSV
下载: 导出CSV
表 2 2组治疗疗效比较[n(%)]
Table 2. Comparison of curative effect between two groups [n(%)]
组别 n 治愈 有效 无效 观察组 72 50(69.4) 14(19.4) 8(11.1) 对照组 68 30(44.1) 23(33.8) 15(22.1)
下载: 导出CSV
表 3 2组阴道前后壁情况比较[(
$\bar x \pm s $ ),cm]Table 3. Comparison of the anterior and posterior vaginal walls between the two groups [(
$\bar x \pm s $ ),cm]组别 n 阴道前壁 阴道后壁 治疗前Aa(cm) 治疗后Aa(cm) 治疗前Ap(cm) 治疗后Ap(cm) 观察组 72 −1.12 ± 1.07 −2.51 ± 0.56* −2.17 ± 0.96 −2.73 ± 0.51* 对照组 68 −0.96 ± 1.35 −1.49 ± 1.19* −1.68 ± 1.39 −2.09 ± 1.05* 与治疗前比较,*P < 0.05。
下载: 导出CSV
表 4 2组治疗前后子宫脱垂情况比较[(
$\bar x \pm s $ ),cm]Table 4. Comparison of uterine prolapse before and after treatment in two groups [(
$\bar x \pm s $ ),cm]组别 n 治疗前C点 治疗后C点 治疗前后子宫脱垂疗效程度 观察组 72 −3.06 ± 0.97* −5.59 ± 1.34* 2.51 ± 0.122* 对照组 68 −3.48 ± 0.62 −4.31 ± 1.03 0.85 ± 0.89 P 0.017 0 0 与对照组比较,*P < 0.05。
下载: 导出CSV
表 5 2组治疗前后慢肌阶段平均值情况对比较(
$\bar x \pm s $ )Table 5. Comparison of the mean value of the slow muscle stage before and after treatment between the two groups (
$\bar x \pm s $ )组别 n 治疗前慢肌阶段平均值 治疗后慢肌阶段平均值 P 观察组 72 22.02 ± 9.49 30.655 ± 8.15 0 对照组 68 23.28 ± 9.47 27.38 ± 1.40 0.004 P 0.363 0.018
下载: 导出CSV
表 6 2组治疗前后耐力测试阶段平均值情况比较(
$\bar x \pm s $ )Table 6. Comparison of the mean value of endurance test before and after treatment in two groups (
$\bar x \pm s $ )组别 n 治疗前耐力测试阶段平均值 治疗后耐力测试阶段平均值 P 观察组 72 19.82 ± 8.33 27.81 ± 7.56 0 对照组 68 21.07 ± 8.78 26.39 ± 5.34 0 P 0.366 0.004
下载: 导出CSV
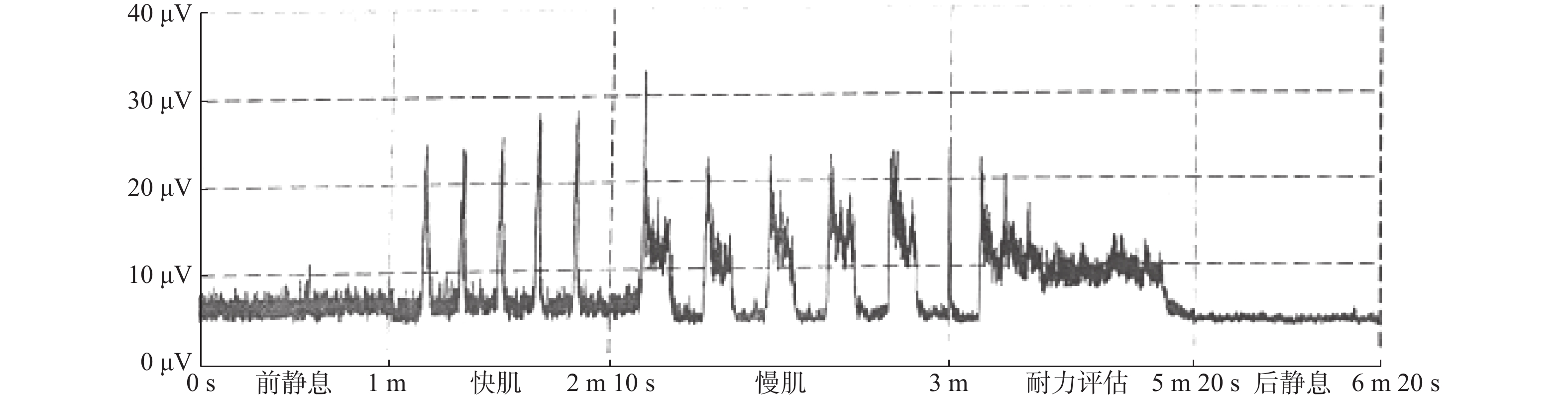
表 7 盆底肌电评估
Table 7. Glazer evaluation chart
阶段 指标 测试值 参考值 前静息阶段 平均值 6.44↑ 2~4 μV 变异性 0.10 < 0.2 快肌(Ⅱ 类肌)测试阶段 快速收缩时间 0.26 < 0.5 s 最大值 25.21↓ 35~45 μV 快速放松时间 12.80↓ 30~40 μV 慢肌(Ⅰ类肌)测试阶段 平均值 10.13↓ 25~35 μV 变异性 0.67↑ < 0.5 s 耐心测试 平均值 0.28↑ < 0.2 变异性 0.18 < 0.2 后 10 s/前 10 s比值 0.75↓ 0.8~1.0 后静息阶段 平均值 3.90 2~4 μV 变异性 0.06 < 0.2
下载: 导出CSV
-
[1] 谢辛, 孔北华, 段涛, 等. 妇产科学[M]. 第9版, 人民卫生出版社. 北京, 2018, 10(3): 279-284. [2] Mesh inlay, mesh kit or native tissue repair for women having repeat anterior or posterior prolapse surgery: randomised controlled trial (PROSPECT)[J]. BJOG: An International Journal of Obstetrics & Gynaecology , 2020, 127(Issue 8): 1002-1013. [3] 朱兰, 郎景和. 女性盆底学[M]. 北京: 人民卫生出版社, 2021: 123-127. [4] Walker G J,Gunasekera P. Pelvic organ prolapse and incontinence indeveloping countries:Review of prevalence and risk factors[J]. Int Urogynecol J,2011,22(2):127-135. [5] 王园园. 益气固脱方联合温针灸治疗轻中度子宫脱垂的临床研究[D]. 南京: 南京中医药大学硕士论文, 2018. [6] 刘毛毛,黄凌,张娅娅,等. 盆底重建术联合聚丙烯网带尿道中段悬吊术治疗子宫脱垂合并压力性尿失禁的临床效果及对盆底功能的影响[J]. 中国妇幼保健,2021,36(22):5348-5352. doi: 10.19829/j.zgfybj.issn.1001-4411.2021.22.069 [7] N Shama,S W Bai,B C Chung,et al. Quantitative analysis of 17 amino acids in the connective tissue of patients with pelvic organ prolapse using capillary electrophoresis tandem mass spectrometry[J]. J. Chromatogr B,2008,865:18-24. [8] Bakas P,Liapis A,Salamalekis E,et al. Tension-free vaginal tape efficacy in relation to collagen quantity of pubocervical fascia[J]. Gynecologic and Obstetric Investigation,2004,57(3):149-152. doi: 10.1159/000076014 [9] ZHOU Yang,LING Ouyang,BO Li. Expression and significance of lysyl oxidase-like 1 and fibulin - 5 in the cardinal ligament tissue of patients with pelvic floor dysfunction[J]. Journal of Biomedical Research,2013,27(1):23-28. [10] 李秉枢,洪莉,程丽薇,等. 转化生长因子-β1/Smad 3在机械力下调盆底成纤维细胞胶原、弹性蛋白表达中的作用[J]. 中国计划生育和妇产科,2018,10(10):54-58. doi: 10.3969/j.issn.1674-4020.2018.10.13 [11] 张惠文,付婷婷,赵淑萍,等. 电刺激生物反馈及阴道哑铃Kegel锻炼治疗产后盆底功能障碍性疾病的临床效果分析[J]. 实用妇产科杂志,2020,36(11):864-867. [12] 张婷婷,张庆,刘盼,等. 盆底磁刺激疗法在产后盆底康复中的疗效观察[J]. 中国妇产科临床杂志,2021,22(5):516-517. doi: 10.13390/j.issn.1672-1861.2021.05.025 [13] Abraham M T,Mashkevich G. Monopolar radiofrequency skin tightening[J]. Facial Plast Surg Clin North Am,2007,15(2):169-177. doi: 10.1016/j.fsc.2007.01.005 [14] 中国整形美容协会 . “AI温控射频技术治疗盆底相关疾病的多中心临床试验 ” 专项基金评审结果公示[EB/OL]. (2019-12-25) [2020-2-25]. http://capa.org.cn/ contents/16/5051.html. [15] Lordelo P,Vilas Boas A,Sodre D,et al. New concept for treating female stress urinary incontinence with radiofrequency[J]. Int Braz J Urol,2017,43:896-902. doi: 10.1590/s1677-5538.ibju.2016.0621 [16] 朱亚丽,杨育丹,张彦梅,等. 射频治疗阴道松弛伴压力性尿失禁疗效分析[J]. 中国医疗美容,2021,11(6):53-56. [17] Fajkosova K,Machovcova A,Onder M Fritz K. Selective radiofrequency therapy as a non-invasive approach for contactless body contouring and circumferential reduction[J]. J Drugs Dermato,2014,13:291-296. [18] Bruce B Allan,Stacie Bell,Kathryn Husarek. A 12-month feasibility study to investigate the effectiveness of cryogencooled monopolar radiofrequency treatment for female stress urinary incontinence[J]. Can Urol Assoc J,2020,14(7):E313-E318. doi: 10.5489/cuaj.6145 [19] Vanaman Wilson M J,Bolton J,Jones I T,et al. Histologic and clinical changes in vulvovaginal tissue after treatment with a transcutaneous temperature-controlled radiofrequency device[J]. Dermatol Surg,2018,44(5):705-713. -











 点击查看大图
点击查看大图
计量
- 文章访问数: 2967
- HTML全文浏览量: 2004
- PDF下载量: 19
- 被引次数: 0
