

The Value of HCT-ALB in the Early Diagnosis of Sepsis-associated Encephalopathy
-
摘要:
目的 寻找简便且可靠的临床定量指标对SAE进行早期诊断是防治SAE的关键。 方法 收集2020年4月至2022年4月入住ICU脓毒症患者72例,脓毒症脑病(SAE)组31例,无脓毒症脑病(Ne-SAE)组41例。记录患者APACHEⅡ、SOFA、一般资料和临床指标计算CLI、HCT-ALB。采集血浆用ELISA检测NT-proCNP、S100A 8、Tau 蛋白、C5a。 结果 SAE组APACHEⅡ评分、SOFA评分较Ne-SAE组明显升高(P < 0.0001),血浆中NT-proCNP和S100A 8较Ne-SAE组明显升高(P < 0.05)。SAE组与Ne-SAE组患者CLI差异无统计学意义(P = 0.823),而2组间HCT-ALB有统计学意义(P = 0.035)。ROC曲线分析结果显示:CLI界值11.04,(AUC = 0.478,95%可信区间0.340~0.616,P = 0.746)敏感度46.34%,特异度80.65%,HCT-ALB界值14.85,(AUC = 0.627,95%可信区间0.491~0.762,P = 0.017)敏感度68.27%,特异度67.74%。 结论 HCT-ALB对脓毒症患者发生SAE具有早期诊断价值。 -
关键词:
- 脓毒症相关性脑病 /
- 毛细血管渗漏指数 /
- 红细胞压积与白蛋白差值 /
- 早期诊断
Abstract:Objective To find simple and reliable clinical quantitative indicators for the early diagnosis of SAE. Methods Seventy-two septic patients who were admitted to ICU from April 2020 to April 2022, including 31 with sepsis encephalopathy (SAE) and 41 without sepsis encephalopathy (Ne-SAE), were collected. APACHE Ⅱ, SOFA and general data of Patients were recorded, and CLI, HCT-ALB were calculated based on the clinical assays. Plasma was collected using ELISA to detect NT-proCNP, S100A 8, Tau protein and C5a. Results APACHEⅡscore and SOFA score in SAE group were significantly higher compared with the patients in Ne-SAE group (P < 0.05). Plasma NT-proCNP and S100A8 levels were significantly higher in the patients with SAE than that of the Ne-SAE group (P < 0.05). There was no significant difference in CLI between SAE group and NE-SAE group. (P = 0.823). But , the hct-alb was statistically significant between the two groups (P = 0.035). The roc curve analysis showed: A cutoff value CLI of 11.04 (AUC = 0.478,95% CI 0.340-0.616, P = 0.746) had 46.34% sensitivity and 80.65% specificity in diagnosing SAE. A cutoff value HCT-ALB of 14.85 (AUC = 0.627,95% CI 0.491-0.762, P = 0.017) had 68.27% sensitivity and 67.74% specificity in diagnosing SAE. Conclusion The HCT-ALB level can be useful in the early diagnosis of SAE in patients with sepsis. -
表 1 SAE组与Ne-SAE组患者一般资料比较 (
$\bar x \pm s $ )Table 1. The comparison of general data between SAE group and Ne-SAE group (
$\bar x \pm s $ )一般资料 SAE组 Ne-SAE组 t/χ2 P (男/女)n(%) 21/10 (67.7/32.3) 28/13(68.3/31.7) 0.002 0.580 年龄(岁) 58.29 ± 12.20 61.41 ± 11.18 −1.129 0.263 APACHEⅡ评分(分) 17.74 ± 2.00 14.78 ± 2.39 5.573 < 0.0001*** SOFA评分(分) 7.42 ± 2.62 4.63 ± 2.03 5.083 < 0.0001*** 感染部位(n) 0.271 0.873 腹腔 18 26 下颌间隙 9 11 肺部 4 4 病原菌检出(n) 0.072 0.513 有 25 27 无 6 9 *P < 0.05,**P < 0.01,***P < 0.001。  下载: 导出CSV
下载: 导出CSV
表 2 SAE组与Ne-SAE组患者血浆NT-proCNP、S100A 8、C5a和Tau蛋白比较[(
$\bar x \pm s $ ),pg/mL]Table 2. The comparison of the levels of NT-proCNP, S100A 8, C5a, and Tau proteins between SAE group and Ne-SAE group [(
$\bar x \pm s $ ),pg/mL]指标 SAE组 Ne-SAE组 t P NT-proCNP 1.01 ± 0.19 0.76 ± 0.06 4.162 0.0005*** S100A 8 1.06 ± 0.22 0.80 ± 0.23 2.760 0.012* Tau蛋白 1.03 ± 0.33 0.88 ± 0.25 1.162 0.259 C5a 0.20 ± 0.07 0.16 ± 0.04 1.494 0.151 *P < 0.05,***P < 0.001。
下载: 导出CSV
表 3 SAE组与Ne-SAE组患者CLI和HCT-ALB比较 (
$\bar x \pm s $ )Table 3. The comparison of the levels of CLI and HCT-ALB between SAE group and Ne-SAE group (
$\bar x \pm s $ )指标 SAE组 Ne-SAE组 t P CLI 7.66 ± 3.94 7.02 ± 3.28 −0.224 0.823 HCT-ALB 17.45 ± 6.96 12.76 ± 4.72 2.155 0.035* *P < 0.05。
下载: 导出CSV
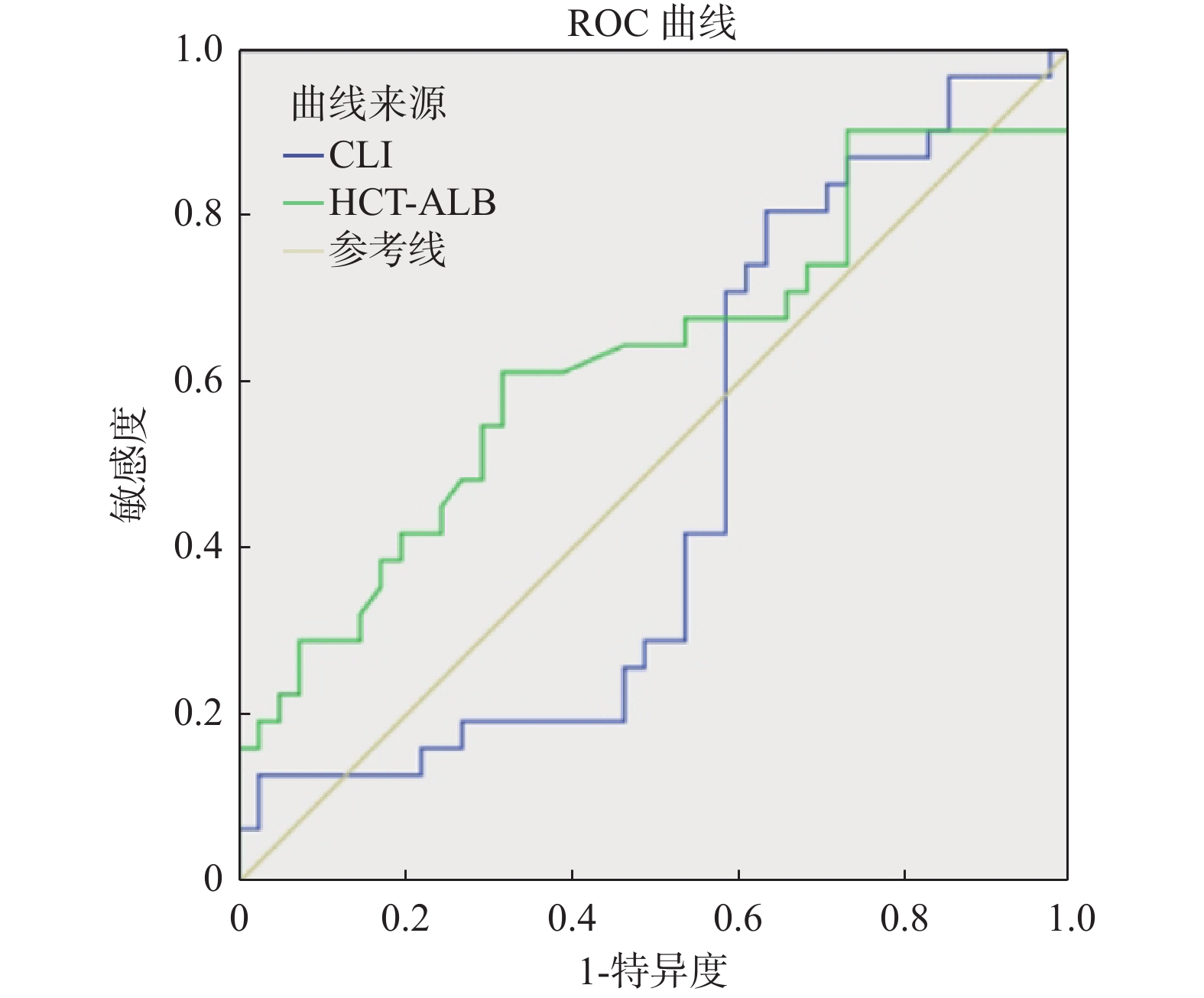
表 4 CLI和HCT-ALB对SAE诊断ROC分析结果
Table 4. The results of ROC analysis about SAE diagnostic by CLI and HCT-ALB
指标 界值 AUC 95%可信区间 敏感度(%) 特异度(%) CLI 11.04 0.478 0.340~0.616 46.34 80.65 HCT-ALB 14.85 0.627 0.491~0.762 68.27 67.74
下载: 导出CSV
-
[1] Tauber S C,Djukic M,Gossner J,et al. Sepsis-associated encephalopathy and septic encephalitis:An update[J]. Expert Rev Anti Infect Ther,2021,19(2):215-231. doi: 10.1080/14787210.2020.1812384 [2] Chen J,Shi X,Diao M,et al. A retrospective study of sepsis-associated encephalopathy:Epidemiology,clinical features and adverse outcomes[J]. BMC Emerg Med,2020,20(1):77. doi: 10.1186/s12873-020-00374-3 [3] Annane D,Sharshar T. Cognitive decline after sepsis[J]. Lancet Respir Med,2015,3(1):61-69. [4] Singer M,Deutschman C S,Seymour C W,et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3)[J]. JAMA,2016,315(8):801-810. doi: 10.1001/jama.2016.0287 [5] Cordemans C,De Laet I,Van Regenmortel N,et al. Fluid management in critically ill patients:The role of extravascular lung water,abdominal hypertension,capillary leak,and fluid balance[J]. Ann Intensive Care,2012,2(Suppl 1):S11-S12. [6] Dai D M,Wang D,Hu D,et al. Difference in hematocrit and plasma albumin levels as an additional biomarker in the diagnosis of infectious disease[J]. Arch Med Sci,2020,16(3):522-530. doi: 10.5114/aoms.2019.86898 [7] Tauber S C,Eiffert H,Bruck W,et al. Septic encephalopathy and septic encephalitis[J]. Expert Rev Anti Infect Ther,2017,15(2):121-132. doi: 10.1080/14787210.2017.1265448 [8] Pensato U,Muccioli L,Cani I,et al. Brain dysfunction in COVID-19 and CAR-T therapy:Cytokine storm-associated encephalopathy[J]. Ann Clin Transl Neurol,2021,8(4):968-979. doi: 10.1002/acn3.51348 [9] Gofton T E,Young G B. Sepsis-associated encephalopathy[J]. Nat Rev Neurol,2012,8(10):557-566. doi: 10.1038/nrneurol.2012.183 [10] Ehler J,Saller T,Wittstock M,et al. Diagnostic value of NT-proCNP compared to NSE and S100B in cerebrospinal fluid and plasma of patients with sepsis-associated encephalopathy[J]. Neurosci Lett,2019,692(10):167-173. [11] Heming N,Mazeraud A,Verdonk F,et al. Neuroanatomy of sepsis-associated encephalopathy[J]. Crit Care,2017,21(1):65. doi: 10.1186/s13054-017-1643-z [12] Zhang L N,Wang X H,Wu L,et al. Diagnostic and predictive levels of calcium-binding protein A8 and tumor necrosis factor receptor-associated factor 6 in sepsis-associated encephalopathy:A prospective observational study[J]. Chin Med J (Engl),2016,129(14):1674-1681. doi: 10.4103/0366-6999.185860 [13] Li X L,Xie J F,Ye X Y,et al. Value of cerebral hypoxic-ischemic injury markers in the early diagnosis of sepsis associated encephalopathy in burn patients with sepsis[J]. Zhonghua Shao Shang Za Zhi,2022,38(1):21-28. [14] Orhun G,Tüzün E,Özcan P E,et al. Association between inflammatory markers and cognitive outcome in patients with acute brain dysfunction due to sepsis[J]. Noro Psikiyatr Ars,2019,56(1):63-70. [15] 李永胜,梅华鲜,黄中会,等. 毛细血管渗漏指数对脓毒症危险分层及预后评估的价值[J]. 临床急诊杂志,2017,18(5):362-365. doi: 10.13201/j.issn.1009-5918.2017.05.010 [16] 王晓晖,徐云海,张波. 毛细血管渗漏指数对脓毒症合并ARDS早期诊断及预后的评估价值[J]. 临床急诊杂志,2020,21(5):350-354. doi: 10.13201/j.issn.1009-5918.2020.05.003 [17] Dai D M,Cao J,Yang H M,et al. Hematocrit and plasma albumin levels difference may be a potential biomarker to discriminate preeclampsia and eclampsia in patients with hypertensive disorders of pregnancy[J]. Clin Chim Acta,2017,464(1):218-222. [18] Clyne B,Olshaker J S. The C-reactive protein[J]. J Emerg Med,1999,17(6):1019-25. doi: 10.1016/S0736-4679(99)00135-3 [19] Pierrakos C,Velissaris D,Bisdorff M,et al. Biomarkers of sepsis:Time for a reappraisal[J]. Crit Care,2020,24(1):287. doi: 10.1186/s13054-020-02993-5 -







 点击查看大图
点击查看大图
计量
- 文章访问数: 3858
- HTML全文浏览量: 2175
- PDF下载量: 27
- 被引次数: 0
