

Treatment of Avulsion Fracture of Anterior Cruciate Ligament Tibial Insertion with Double Row Suture under Arthroscopy
-
摘要:
目的 探讨关节镜下双排缝线固定治疗前交叉韧带胫骨止点撕脱骨折的疗效。 方法 选择昆明医科大学第一附属医院运动医学科2017年1月至2020年12月收治的符合纳入、排除标准的前交叉韧带胫骨止点撕脱骨折患者35例,所有患者均在关节镜下行双排缝线固定治疗。比较患者术前与术后12月的Lysholm评分、国际膝关节文献委员会评分。所有入组患者均签署相关知情同意书,试验方案经昆明医科大学第一附属医院伦理委员会通过。 结果 患者12月复查时,Lysholm评分、IKDC评分均高于术前,且差异有统计学意义(Lysholm评分:(91.143±3.228)分vs(39.343±4.721)分,t = 60.526,P < 0.001;IKDC评分:(89.171±3.510)分vs(39.143±4.044)分,t = 69.368,P < 0.001)。 结论 关节镜下Versalok锚钉双排缝线固定法手术操作简单,即能保证撕脱骨块的稳定固定又能恢复前交叉韧带的张力,恢复膝关节稳定性。 -
关键词:
- 前交叉韧带胫骨止点撕脱骨折 /
- Versalok锚钉 /
- 关节镜 /
- 微创治疗 /
- Meyers-Mckeever分型
Abstract:Objective To investigate the effect of double row suture fixation on avulsion fracture of anterior cruciate ligament (ACL) tibial insertion under arthroscopy. Methods A total of 35 patients with avulsion fracture of anterior cruciate ligament tibial insertion and meeting the inclusion and exclusion criteria were selected from the Department of Sports Medicine, the First Affiliated Hospital of Kunming Medical University from January 2017 to December 2020. All patients were treated with double row sutures under arthroscopy. Lysholm score and International Committee for Knee Literature score were compared between the patients before and 12 months after the surgery. All the enrolled patients signed the relevant informed consent, and the trial plan was approved by the Ethics Committee of the First Affiliated Hospital of Kunming Medical University. Results Lysholm score and IKDC score at 12 months of review were higher than those before the surgery, and the differences were statistically significant (Lysholm score: (91.14±3.22) vs (39.34±4.72), t = 60.53, P < 0.001; IKDC score: (89.17±3.51) vs (39.14±4.04), t = 69.37, P < 0.001. Conclusion The Versalok anchor double-row suture fixation method under arthroscopy is simple and can ensure the stable fixation of avulsed bone and restore the tension of ACL and stability of knee joint. -
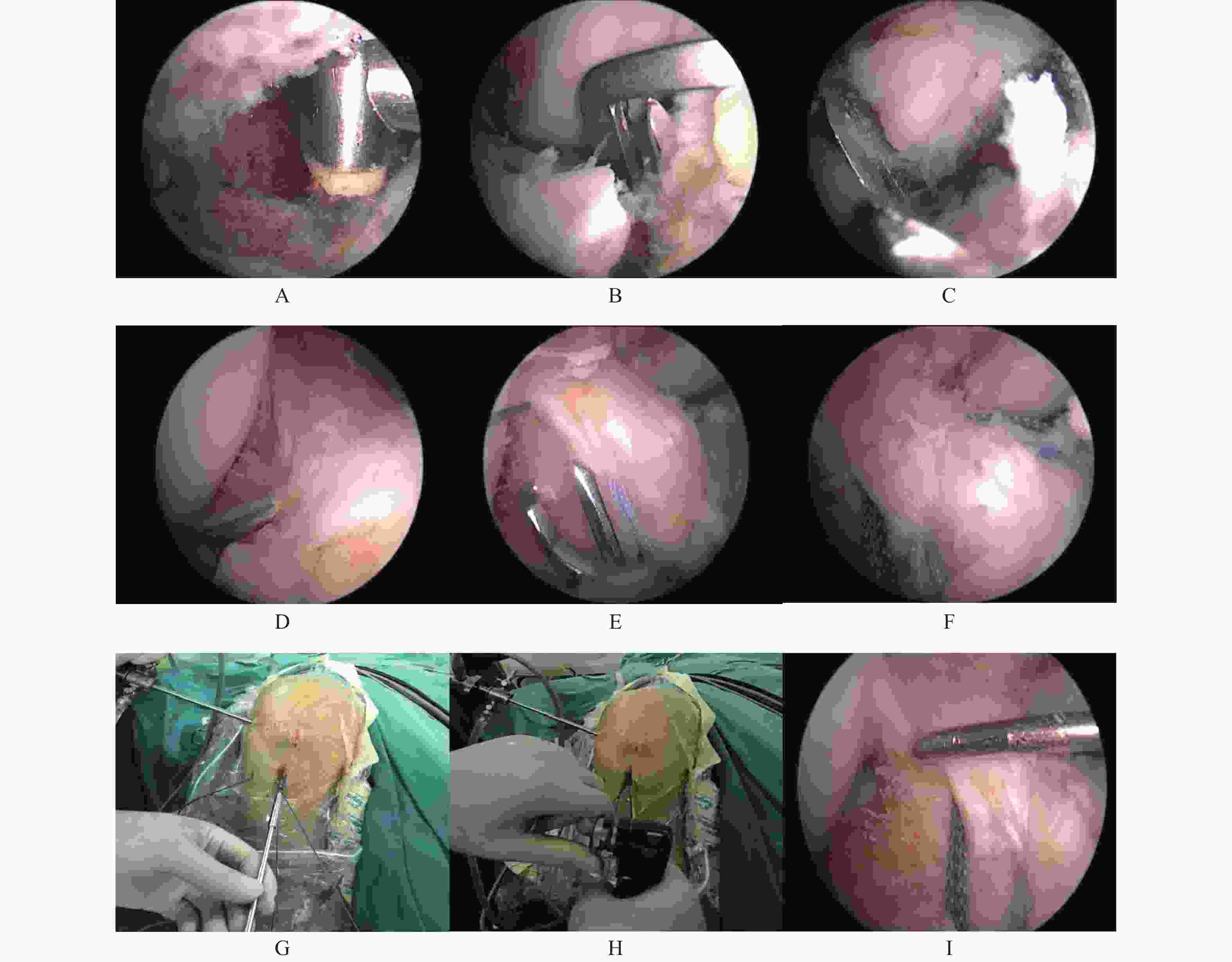
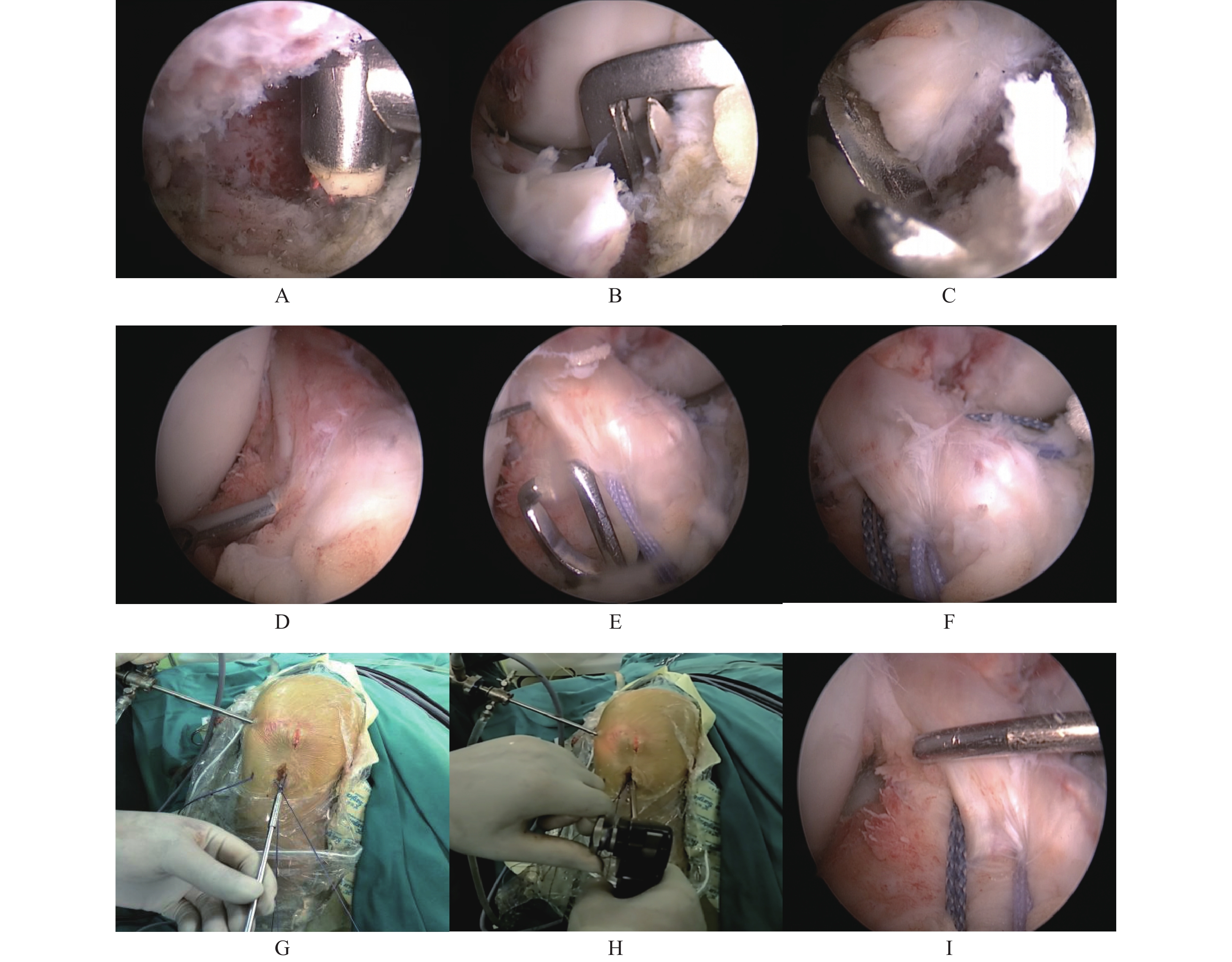
图 1 关节镜下Versalok锚钉双排缝线固定手术方法
A:清理胫骨足印区;B:在胫骨足印区中前1/3内侧钻取骨道;C:在胫骨足印区中前1/3外侧钻取骨道;D:在骨块-前交叉韧带交界处中前1/3穿线;E:在骨块-前交叉韧带交界处中后1/3穿线;图F为各穿两道线后的前交叉韧带止点端;G:双排法布线后置入Versalok锚钉;H:转动轮盘收紧缝线;I:测试骨块复位是否牢固及前交叉韧带的紧张度。
Figure 1. Surgical method of Versalok anchor double row suture fixation under arthroscopy

图 2 典型患者影像学资料及前交叉韧带重建术中关节镜下情况
A:术前MRI,箭头处可见前交叉韧带胫骨止点处骨撕脱;B:术前X线,箭头处可见骨折线;C:术中关节镜下,箭头处可见前交叉韧带胫骨止点端撕脱的骨块;D:关节镜下双排缝线固定后的前交叉韧带;E:术后6月MRI,箭头处可见前叉韧带位置良好;F:术后6月X线,可见骨折线消失。
Figure 2. Imaging data of typical patients and the arthroscopic situation during anterior cruciate ligament reconstruction
表 1 患者的一般资料 [(
$\bar x \pm s $ )/n]Table 1. General patient information [(
$\bar x \pm s $ )/n]指标 数据 性别(男/女) 19/16 年龄(岁) 29.114 ± 6.429 膝关节位置 (左/右) 14/21 Meyers-Mckeever分型(Ⅱ型/Ⅲ型) 15/20 受伤至手术时间(d) 5.943 ± 2.678  下载: 导出CSV
下载: 导出CSV
表 2 患者术后12个月时与术前Lysholm评分、IKDC评分比较[n = 35,(
$\bar x \pm s $ ),分]Table 2. Comparison of Lysholm score and IK9DC score between patients 12 months after surgery and those before surgery [n = 35,(
$\bar x \pm s $ ),points]时间 Lysholm评分 IKDC评分 术前 39.343 ± 4.721 39.143 ± 4.044 术后12月 91.143 ± 3.228 89.171 ± 3.510 t 60.526 69.368 P < 0.001* < 0.001* *P < 0.05。
下载: 导出CSV
-
[1] Strauss Eric J,Kaplan Daniel James,Weinberg Maxwell E,et al. Arthroscopic management of tibial spine avulsion fractures:Principles and techniques[J]. J Am Acad Orthop Surg,2018,26(10):360-367. doi: 10.5435/JAAOS-D-16-00117 [2] Meyers M H,Mckeever F M. Fracture of the intercondylar eminence of the tibia[J]. The Journal of bone and joint surgery. American volume,1959,41-A(2):209-222. [3] 万大地,董志杰,段祥瑞,等. 前交叉韧带胫骨止点撕脱骨折治疗进展[J]. 医学理论与实践,2020,33(14):2264-2266. doi: 10.19381/j.issn.1001-7585.2020.14.011 [4] 孙浩源,肖琼润,杨国夫. 前交叉韧带胫骨止点撕脱骨折治疗的研究进展[J]. 医学综述,2020,26(20):4098-4102. doi: 10.3969/j.issn.1006-2084.2020.20.027 [5] Zanna Luigi,Del Prete Armando,Benelli Giovanni,et al. Knee central pivot bicruciate avulsion and proximal anterior cruciate ligament tear primary repair:A rare case report[J]. Trauma Case Rep,2021,32(2021):100406. [6] 杨文君,张会久,李晨辰,等. 单枚空心钉治疗未成年MeyersⅡ、Ⅲ型前交叉韧带胫骨止点撕脱骨折[J]. 锦州医科大学学报,2021,42(4):83-87. [7] 肖坤,闵军,杨杰,等. 改良缝线固定前交叉韧带胫骨止点撕脱骨折的疗效观察[J]. 实用骨科杂志,2020,26(10):938-941. doi: 10.13795/j.cnki.sgkz.2020.10.020 [8] 王华磊,叶向阳,汤立新. 关节镜下带线锚钉固定治疗前交叉韧带胫骨止点撕脱骨折[J]. 临床骨科杂志,2020,23(5):749-750. doi: 10.3969/j.issn.1008-0287.2020.05.051 [9] Wu J,Luo W,Ren F et al. Therapeutic effects of small incision open reduction and internal fixation and arthroscopic high strength non-absorbable suture on tibial insertion avulsion fracture of the anterior cruciate ligament[J]. Acta Chir Orthop Traumatol Cech,2022,89(1):53-59. [10] Acebrón-Fabregat Á,Pino-Almero L,López-Lozano R et al. Treatment and evolution of chronic avulsion of the anterior tibial spine in the pediatric age[J]. Acta Ortop Mex,2019,33(2):96-101. [11] 牛金龙,黄远章,王晋豫,等. 前交叉韧带胫骨止点撕脱骨折研究进展[J]. 中华临床医师杂志,2016,10(12):1819-1822. [12] Musahl Volker,Nazzal Ehab M,Lucidi Gian Andrea,et al. Current trends in the anterior cruciate ligament part 1:Biology and biomechanics[J]. Knee Surg Sports Traumatol Arthrosc,2022,30(1):20-33. doi: 10.1007/s00167-021-06826-y [13] Della Villa Francesco,Tosarelli Filippo,Ferrari Rocco,et al. Systematic video analysis of anterior cruciate ligament injuries in professional male rugby players:Pattern,injury mechanism,and biomechanics in 57 consecutive cases[J]. Orthop J Sports Med,2021,9(11):23259671211048182. [14] Cui Ze,Chen Zenghao,Qian Donghai,et al. A study of knee anterior cruciate ligament biomechanics with respect to energy and relaxation[J]. Clin Biomech (Bristol,Avon),2020,80(2020):105159. [15] Hannon Joseph P,Goto Shiho,Singleton Steve,et al. Effects of anterior cruciate ligament reconstruction on patellofemoral joint stress and lower extremity biomechanics at 12 weeks post-surgery and at time of return to sport in adolescent females[J]. Clin Biomech (Bristol,Avon),2020,80(2020):105164. [16] Kaur Mandeep,Ribeiro Daniel Cury,Webster Kate E,et al. Knee biomechanics while navigating steps in participants with anterior cruciate ligament reconstruction,between 2 and 10 years following surgery[J]. Phys Ther Sport,2020,46(2020):70-76. [17] Lindanger L,Strand T,Mlster A O,et al. Predictors of osteoarthritis development at a median 25 years after anterior cruciate ligament reconstruction using a patellar tendon autograft[J]. The American Journal of Sports Medicine,2022,50(5):1195-1204. doi: 10.1177/03635465221079327 [18] 邓永,李俊,张季永,等. 关节镜下"8"字缝线和带线锚钉治疗前交叉韧带胫骨止点撕脱性骨折的疗效对比[J]. 实用骨科杂志,2022,28(1):86-89. [19] 陈秋辉,肖伟,李发平,等. 关节镜下Fiber Tape环形固定对前交叉韧带胫骨止点撕脱性骨折患者膝关节功能恢复的影响[J]. 微创医学,2021,16(5):661-664. [20] 赵智,邓煜,陈宇,等. 关节镜下免打结锚钉联合Endobutton钛板治疗后交叉韧带胫骨止点撕脱骨折[J]. 中国骨伤,2021,34(12):1136-1140. [21] Mortazavi Seyed Mohammad Javad,Hasani Satehi Sadegh,Vosoughi Farzad et al. Arthroscopic fixation of anterior cruciate ligament avulsion fracture using fiber wire suture with suture disc[J]. Arthrosc Tech,2021,10(7):1709-1715. doi: 10.1016/j.eats.2021.03.018 [22] 潘平,邓凯. 前交叉韧带胫骨止点撕脱骨折的两种固定方式[J]. 中国继续医学教育,2021,13(30):115-118. doi: 10.3969/j.issn.1674-9308.2021.30.030 [23] Hunter R E,Willis J A. Arthroscopic fixation of avulsion fractures of the tibial eminence:Technique and outcome[J]. Arthroscopy the Journal of Arthroscopic & Related Surgery,2004,20(2):113-121. [24] Seon J K,Park S J,Lee K B,et al. A clinical comparison of screw and suture fixation of anterior cruciate ligament tibial avulsion fractures[J]. American Journal of Sports Medicine,2009,37(12):2334-2339. doi: 10.1177/0363546509341031 [25] Sonak I,Wiedemann A,Heppner H J. Treatment of tibial eminence fractures:A systematic review[J]. J Knee Surg,2015,28(3):255-262. [26] Leonardo,Osti,Matteo,et al. Arthroscopic treatment of tibial eminence fracture:A systematic review of different fixation methods[J]. British medical bulletin,2016,118(1):73-90. doi: 10.1093/bmb/ldw018 [27] Hiranaka Takaaki, Furumatsu Takayuki, Tanaka Takaaki, et al. Combining pullout suture and retrograde screw fixation for anterior cruciate ligament tibial eminence avulsion fractures: A case report [J] . J Orthop Surg (Hong Kong), 2020, 28(2): 2309499020918681. [28] 倪建龙,时志斌,樊立宏,等. 关节镜下双头空心加压螺钉固定治疗前交叉韧带胫骨止点撕脱骨折的疗效[J]. 中华骨与关节外科杂志,2019,12(11):877-881. doi: 10.3969/j.issn.2095-9958.2019.11.09 [29] 成兵,刘振华,程伟. 关节镜下Arthrex锚钉内固定治疗前交叉韧带胫骨止点撕脱骨折[J]. 中国骨与关节损伤杂志,2020,35(4):420-422. doi: 10.7531/j.issn.1672-9935.2020.04.032 [30] 程松苗,陈鹏旭,李强,等. 关节镜下缝线桥技术治疗儿童新鲜前交叉韧带胫骨止点骨折[J]. 创伤外科杂志,2020,22(8):583-587. -






 点击查看大图
点击查看大图
计量
- 文章访问数: 3332
- HTML全文浏览量: 2648
- PDF下载量: 26
- 被引次数: 0
