

Value of 3.0T Magnetic Resonance Cholangiopancreatography in Diagnosing Pancreaticobiliary Maljunction in Children
-
摘要:
目的 探讨3.0T磁共振胆胰管成像(MRCP)诊断儿童胰胆管合流异常的术前诊断价值。 方法 回顾性分析广东省妇幼保健院25例经手术证实的胰胆管合流异常患儿(其中男8例,女17例;年龄1月3 d至14岁)的术前常规MR、MRCP原始图像及重建影像资料,并与术中所见及术中胆道造影对照,由2位副主任医师以上放射科诊断医师分析图像,然后讨论得出影像诊断结。 结果 25例确诊胰胆管合流异常患儿中,常规MR及MRCP准确显示了其中的 18例(符合率为72%),术中胆道造影准确显示了22例(符合率为88%),二者符合率差异无统计学意义(P > 0.05)。其中16例MRCP显示与术中胆道造影一致,可以清晰显示胰胆管合流、胰管、肝内胆管、胆总管,可明确胰胆管合流异常分型。25例患儿中胰胆管合流异常Ⅰ型16例、Ⅱ型5例、Ⅲ型3例、Ⅳ型1例。 结论 3.0TMR为无创性诊断儿童胰胆管合流异常的有效方法,与术中胆道造影相互补充,达到术前确诊的目的。 Abstract:Objective To investigate the preoperative diagnostic value of 3.0T magnetic resonance cholangiopancreatography (MRCP) in the diagnosis of Pancreaticobiliary maljunction (PBM) in children. Methods A retrospective analysis of 25 cases of children with PBM (8 males and 17 females; age 1 month 3 days to 14 years old) of 25 children with PBM confirmed by the Guangdong Worman and Children Hospital were conducted. We reconstructed the image data and compared it with the intraoperative findings and intraoperative cholangiography. Two radiologists at or above the deputy chief physician analyzed the images, and then discussed the results of the imaging diagnosis. Results Among the 25 children diagnosed with PBM, conventional MR and MRCP accurately showed 18 of them (the coincidence rate was 72%), and intraoperative cholangiography accurately showed 22 cases (the coincidence rate was 88%). There was no statistically significant difference in coincidence rate (P > 0.05). Among them, 16 cases of MRCP showed consistent with intraoperative cholangiography, which can clearly show PBM, pancreatic duct, intrahepatic bile duct, and common bile duct, which can clarify the abnormal classification of PBM. Among the 25 children with PBM, 16 cases were type Ⅰ, 5 cases were type Ⅱ, 3 cases were type Ⅲ, and 1 case was type Ⅳ. Conclusion 3.0T MR is an effective method for non-invasive diagnosis of PBM in children. It complements intraoperative cholangiography to achieve the purpose of preoperative diagnosis rate. -
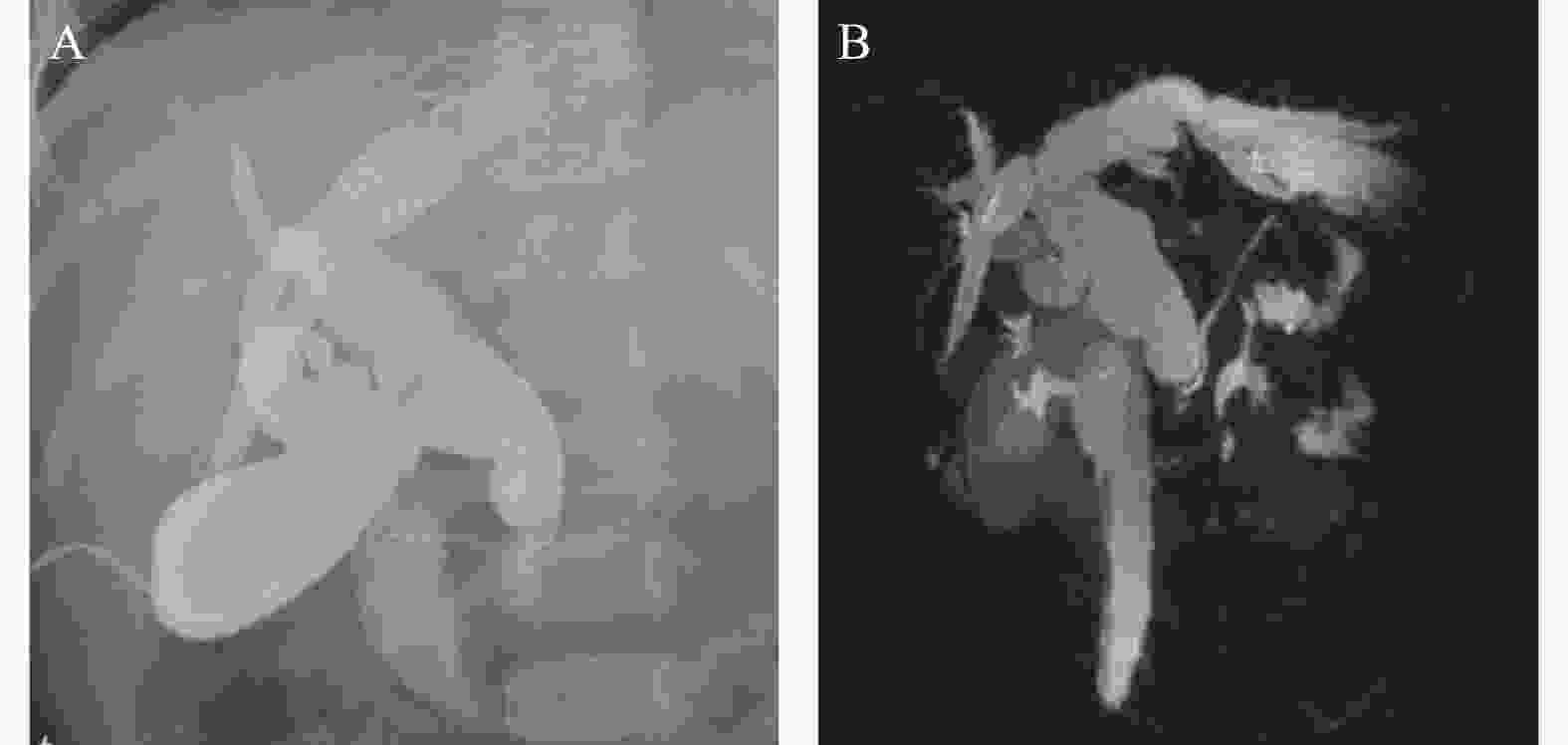
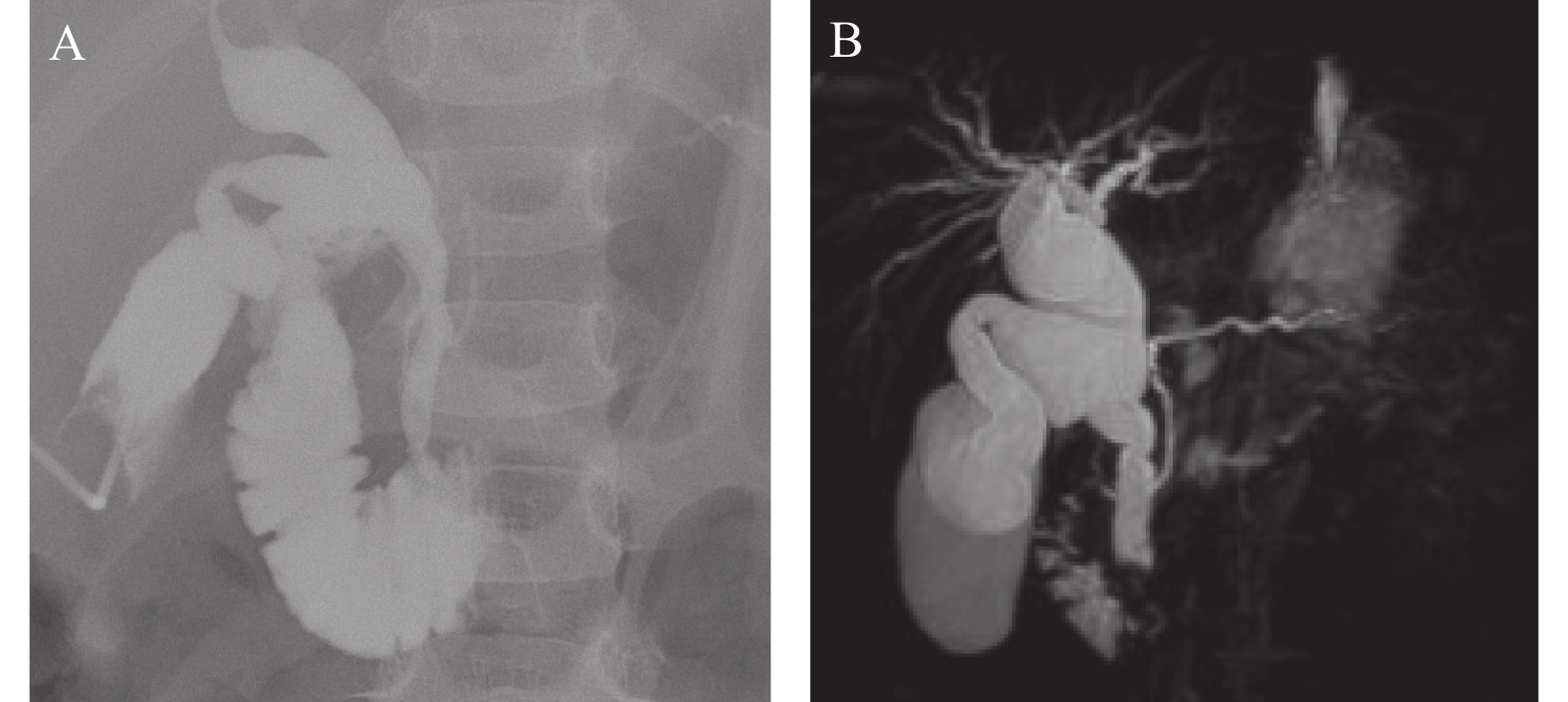
图 1 患儿4岁
胰胆管合流异常,术中胆道造影胆总管遮蔽胰胆管合流部,MRCP重建3D图像旋转约50度,清晰显示胰胆管合流部,显示胆总管合流部狭窄,明确分型为Ⅰ型。
Figure 1. A 4 year-old male patient

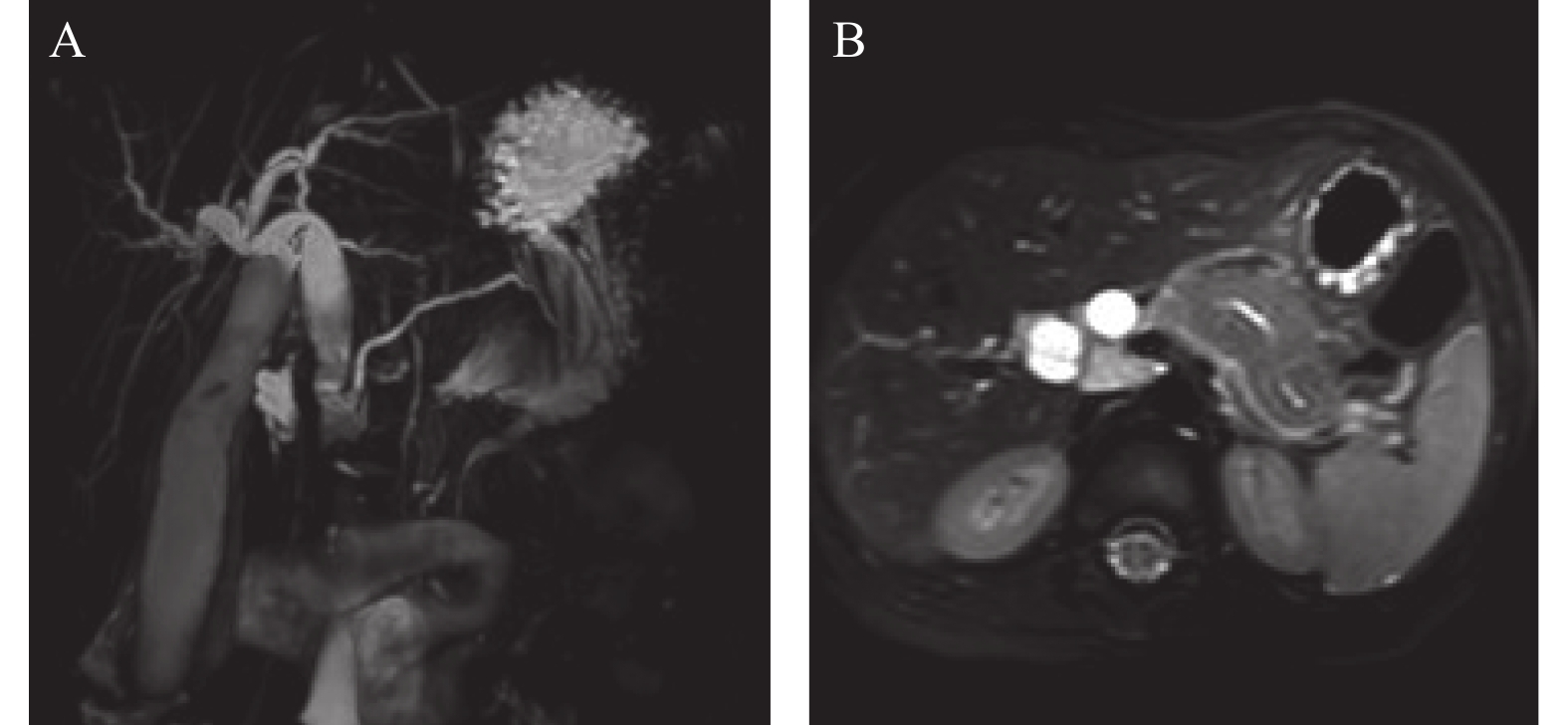
图 3 患儿,女,3岁
因皮肤间歇性黄染一周就诊,胰胆管合流异常Ⅱ型,轴位T2WI显示胰腺轴位少量渗出,提示胰腺炎。
Figure 3. A 3 year-old female patient
表 1 MRI和IOC对胰胆管显示情况(n)
Table 1. The display of pancreaticobiliary duct by MRI and IOC (n)
项目 MR IOC P PBM 18(72) 22(88) 1.0 PD 19(76) 24(96) 0.024* CBD 23(92) 25(100) - IHBD 25(100) 25(100) - MR磁共振成像,IOC 术中胰胆管造影,PBM:胰胆管合流异常,PD:胰管,CBD:胆总管,IHBD:肝内胆管。*P < 0.05。  下载: 导出CSV
下载: 导出CSV
-
[1] Ono Ayako,et al. Imaging of Pancreaticobiliary Maljunction[J]. Radiographics:A review publication of the Radiological Society of North America Inc,2020,40(2):378-392. [2] Andriulli A,Loperfido S,Napolitano G,et al. Incidence rates of post-ERCP complications:A systematic survey of prospective studies[J]. Am J Gastroenterol,2007,102(8):1781-1788. doi: 10.1111/j.1572-0241.2007.01279.x [3] Deng Z,Zeng J,Lv C,et al. Prevalence and factors associated with post-endoscopic retrograde cholangiopancreatography pancreatitis in children[J]. Dig Dis Sci,2021,66(1):224-230. doi: 10.1007/s10620-020-06179-5 [4] Guo W L,Wang J. Preoperative one-stop magnetic resonance imaging evaluation of the pancreaticobiliary junction and hepatic arteries in children with pancreaticobiliary maljunction:A prospective cohort study[J]. Surg Today,2021,51(1):79-85. doi: 10.1007/s00595-020-02077-5 [5] 刘菁华,杨秀军. 3.0T磁共振胆胰管成像在儿童先天性胆道畸形诊断中的价值[J]. 中华实用儿科临床杂志,2017,32(18):1425-1428. doi: 10.3760/cma.j.issn.2095-428X.2017.18.016 [6] Urushihara N,Hamada Y,Kamisawa T,et al. Classification of pancreaticobiliary maljunction andclinical features in children[J]. J Hepatobiliary Pancreat Sci,2017,24(8):449-455. doi: 10.1002/jhbp.485 [7] Kamisawat,Kurumas,Chibak. Congenital biliaryDilatation and pancreaticobiliary maljunction[J]. Nihon Shokakibyogakkai Zasshi,2016,113(12):1991-1997. [8] Hamada Y,Ando H,Kamisawa T,et al. Diagnosticcriteria for congenital biliary dilatation 2015[J]. J Hepatobiliary Pancreat Sci,2016,23(6):342-346. doi: 10.1002/jhbp.346 [9] 智发朝,朱建新,陈村龙,等. 磁共振胰胆管成像和直接胰胆管造影对胆胰疾病诊断价值自身对比的前瞻性研究[J]. 中华消化杂志,2001,10:25-27. doi: 10.3760/j.issn:0254-1432.2001.01.008 [10] Siles P,Aschero A,Gorincour G,et al. Aprospectivepilotstudy:Can the biliary tree be visualized in children younger than 3 months on magnetic resonance cholangiopancreatography?[J]. PediatrRadiol,2014,44(9):1077-1084. [11] Huang S G,Guo W L,Wang J,et al. Factors interfering with delineation on MRCP of pancreaticobiliary maljunction in paediatric patients[J]. PLoS One,2016,11(4):e0154178. doi: 10.1371/journal.pone.0154178 [12] Kamisawa T,Ando H,Hamada Y,et al. Diagnosticcriteria for pancreaticobiliary maljunction 2013[J]. J Hepatobiliary Pancreat Sci,2014,21(3):159-161. -

 点击查看大图
点击查看大图

图(3) / 表(1)
计量
- 文章访问数: 3987
- HTML全文浏览量: 2212
- PDF下载量: 100
- 被引次数: 0
