

Characterization of Cardiac Color Ultrasonography and Carotid Ultrasonography in HIV/AIDS Patients in Different Age Groups
-
摘要:
目的 分析不同年龄组HIV/AIDS患者心脏彩超和颈动脉超声的特点。 方法 采用横断面研究方法,选取2020年12月1日至2021年11月30日在昆明市第三人民医院感染科就诊行心脏彩超和颈动脉超声检查的HIV/AIDS患者,根据WHO公布的年龄分组标准,分为青年组(≤44岁)98例(28.0%)、中年组(45~59岁)166例(47.4%)和老年组(≥60岁)86例(24.6%),采用 Excel和SPSS26.0对数据进行整理和分析。 结果 不同年龄组在民族、吸烟、传播途径、有高血压、有糖尿病及有肝炎及方面,差异有统计学意义(P < 0.05);心脏彩超和颈动脉超声的异常情况在不同年龄组中存在着差异(P < 0.05),且随着年龄的增加,超声检查的异常情况呈逐渐增加的趋势(χ2趋势分别为107.148、77.666,P趋势值均 < 0.05)。在心脏彩超和颈动脉超声检查的异常结果中,不同年龄组在左室舒张功能障碍、主动脉钙化、肺动脉收缩压升高、主动脉瓣反流、室间隔增厚、左右房内径增大、右室内径增大、二尖瓣钙化、颈部有无斑块、双侧颈动脉内膜中层厚度增厚、右侧颈内动脉峰值流速及双侧颈内动脉阻力指数方面差异有统计学意义(P < 0.05),其中左心室舒张功能障碍的发生最常见。 结论 不同年龄组HIV/AIDS患者心脏彩超和颈动脉超声的异常情况及异常的表现存在着差异,临床医生应根据患者的临床表现及超声的检查结果,对不同年龄组HIV/AIDS患者相关心血管疾病做出及时地诊断。 Abstract:Objective Cross-sectional study of the characteristics of cardiac color ultrasonography and carotid ultrasonography in different age groups of patients with HIV/AIDS. Methods This study collected data from HIV/AIDS patients, who attended the Department of Infection I at the Third People’s Hospital of Kunming from December 1, 2020 to November 30, 2021, and the patients underwent the cardiac color ultrasonography and carotid ultrasonography. Patients was divided into 98 cases (28.0%) in the young group (≤44 years old) and 166 cases (47.4%) in the middle-aged group (45-59 years old) and 86 cases (24.6%) in the elderly group (≥60 years old), according to the age grouping criteria published by WHO, and the data were organized and analyzed using Excel and SPSS26.0. Results In accordance with our study, there were statistically significant differences between age groups in terms of ethnicity, smoking, route of transmission, presence of hypertension, diabetes mellitus, and presence of hepatitis and (P < 0.05); the abnormalities of cardiac color ultrasonography and carotid ultrasonography were different in different age groups (P < 0.05). Additionally, there was a gradually increasing trend in the abnormalities of ultrasound examination (χ2 trend were 107.148, 77.666, all P trend values < 0.05). Among the abnormal findings of cardiac color ultrasonography and carotid ultrasonography in different age groups , there were statistically significant differences in the incidence rate of the following indicators (P < 0.05), such as left ventricular diastolic dysfunction, aortic calcification, elevated pulmonary artery systolic pressure, aortic regurgitation, ventricular septal thickening, increased right and left atrial internal diameter, increased right ventricular internal diameter, mitral valve calcification, presence of plaque in the neck, whether there was thickening of the intima-media thickness of the carotid arteries bilaterally, the peak flow velocity of the right internal carotid artery and bilateral internal carotid artery resistance index. Of those, the incidence rate of left ventricular diastolic dysfunction was most common. Conclusions For patients with HIV/AIDS in different age groups, differences in the abnormal findings and abnormal presentation of cardiac color ultrasonography and carotid ultrasonography. Based on the clinical manifestations and ultrasound findings of the patients, clinicians should make timely diagnosis of cardiovascular diseases associated with HIV/AIDS patients in different age groups. -
Key words:
- HIV/AIDS /
- Different age groups /
- Cardiac color ultrasonography /
- Carotid ultrasonography
-
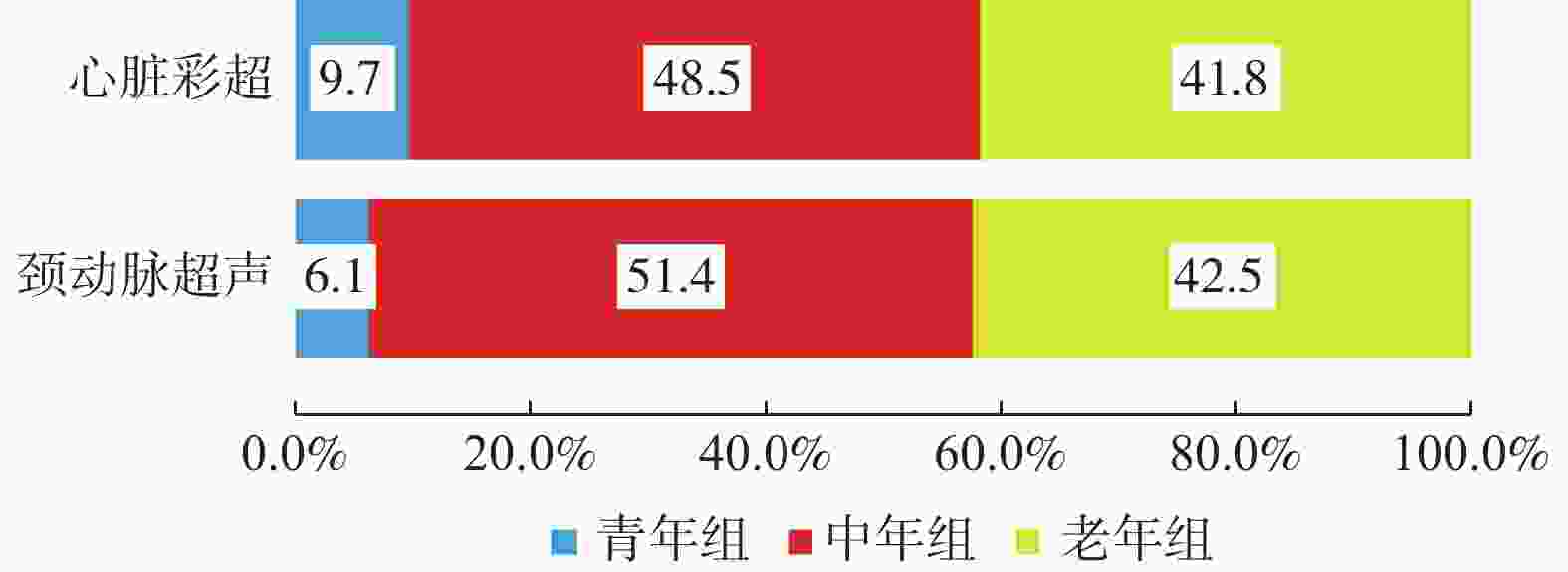
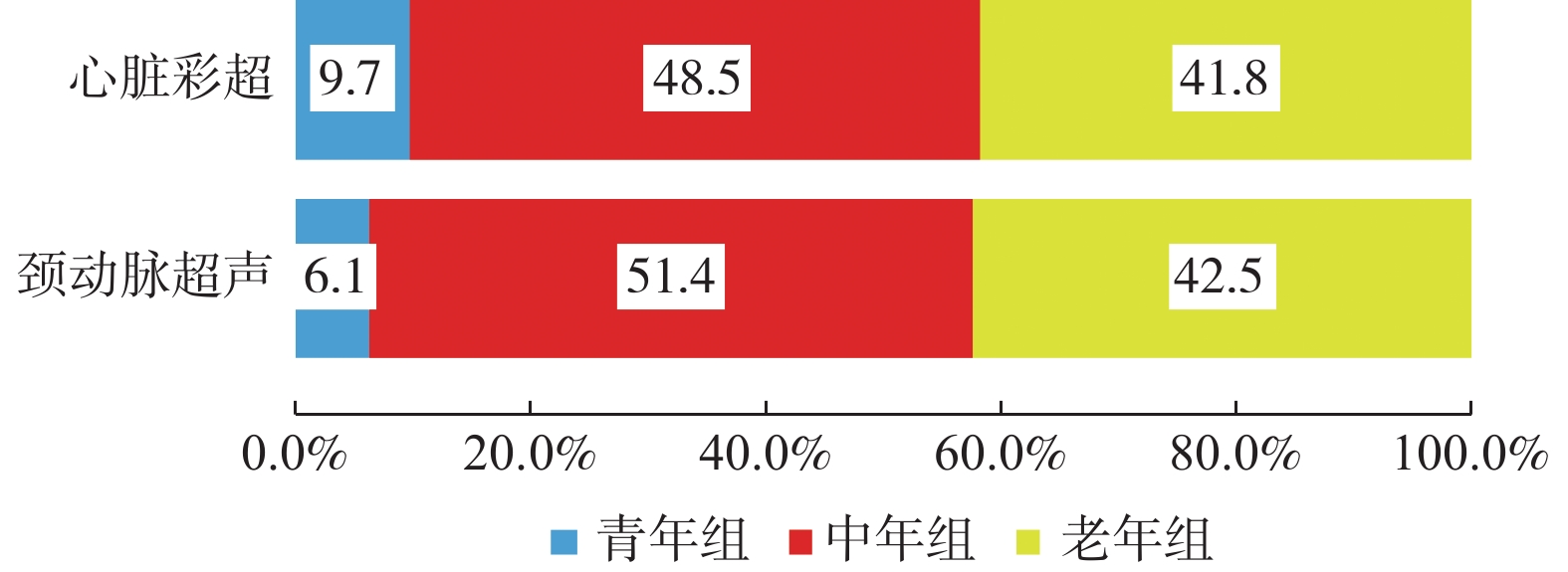
图 1 不同年龄组HIV/AIDS患者心脏彩超和颈动脉超声异常结果构成(%)
Figure 1. Composition of abnormal color ultrasonography and carotid ultrasonography findings in patients with HIV/AIDS in different age groups (%)
表 1 不同年龄组HIV/AIDS患者的一般资料分析[n(%)]
Table 1. Analysis of general information of HIV/AIDS patients in different age groups [n(%)]
一般资料 青年组(n = 98) 中年组(n = 166) 老年组(n = 86) χ2 P 性别 男 70(71.4) 109(65.7) 63(73.3) 1.864 0.394 女 28(28.6) 57(34.3) 23(26.7) 民族 汉族 85(86.7) 144(86.7) 84(97.7)#△ 8.200 0.017* 少数民族 13(13.3) 22(13.3) 2(2.3) 体重指数 20.8(18.5,22.2) 20.8(19.0,22.6) 21.1(18.9,23.5) 0.483 0.785 心血管危险因素 饮酒 有 38(38.8) 81(48.8) 35(40.7) 3.015 0.221 无 60(61.2) 85(51.2) 51(59.3) 吸烟 有 43(43.9) 104(62.7)* 45(52.3) 9.065 0.011* 无 55(56.1) 62(37.3) 41(47.7) 高血压 有 12(12.2) 46(27.7)* 24(27.9)# 9.491 0.009* 无 86(87.8) 120(72.3) 62(72.1) 糖尿病 有 17(17.3) 46(27.7) 33(38.4)# 10.185 0.006* 无 81(82.7) 120(72.3) 53(61.6) 高脂血症 有 26(26.5) 44(26.5) 15(17.4) 2.904 0.234 无 72(73.5) 122(73.5) 71(82.6) 肝炎 有 12(12.2) 46(27.7)* 1(1.2)#△ 30.554 < 0.001* 无 86(87.8) 120(72.3) 85(98.8) 传播途径 42.649 < 0.001* 性传播 56(57.1) 87(52.4) 46(53.5) 吸毒史 22(22.5) 48(28.9) 1(1.1) 其他 0(0.0) 6(3.6) 6(7.0) 不详 20(20.4) 25(15.1) 33(38.4) HIV病毒载量 6.970 0.137 < 100拷贝/mL 51(52.0) 110(66.3) 56(65.1) 100~5000拷贝/mL 9(9.2) 10(6.0) 3(3.5) > 5000拷贝/mL 38(38.8) 46(27.7) 27(31.4) CD4+T淋巴细胞计数 4.504 0.342 < 200个/μL 45(45.9) 65(39.2) 36(41.9) 200~500个/μL 28(28.6) 54(32.5) 34(39.5) > 500个/μL 25(25.5) 47(28.3) 16(18.6) 抗病毒治疗情况 未治疗 26(26.5) 30(18.1) 15(17.4) 3.297 0.192 已治疗 72(73.5) 136(81.9) 71(82.6) 与青年组比较,*P < 0.05;与中年龄组比较,△P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 不同年龄组HIV/AIDS患者心脏彩超和颈动脉超声异常情况比较 [n(%)]
Table 2. Comparison of cardiac color ultrasonography and carotid ultrasonography abnormalities in patients with HIV/AIDS in different age groups [n(%)]
项目 青年组(n = 98) 中年组(n = 166) 老年组(n = 86) 异常率(%) χ2 P χ2趋势 P趋势 心脏彩超 56.0 107.456 < 0.001* 107.148 < 0.001* 正常 79(80.6) 71(42.8) 4(4.6) 异常 19(19.4) 95(57.2)* 82(95.4)*△ 颈动脉超声 42.3 78.632 < 0.001* 77.666 < 0.001* 正常 89(90.8) 90(54.2) 23(26.7) 异常 9(9.2) 76(45.8)* 63(73.3)*△ 与青年组比较,*P < 0.05;与中年龄组比较,△ P < 0.05。
下载: 导出CSV
表 3 不同年龄组HIV/AIDS患者心脏彩超和颈动脉超声诊断结果分析[n(%);M(P25,P75)]
Table 3. Comparison of diagnostic results of color ultrasonography and carotid ultrasonography in patients with HIV/AIDS in different age groups [n(%);M(P25,P75)]
检查结果 青年组(98) 中年组(166) 老年组(86) χ2/H P 心脏彩超 左室舒张功能障碍 8(8.2) 72(43.4)* 67(77.9)*△ 91.706 < 0.001* 主动脉钙化 1(1.0) 18(10.8)* 38(44.2)*△ 69.460 < 0.001* 肺动脉收缩压升高 4(4.1) 18(10.8) 22(25.6)*△ 20.121 < 0.001* 主动脉瓣反流 1(1.0) 12(7.2) 26(30.2)*△ 44.362 < 0.001* 室间隔增厚 0(0.0) 12(7.2)* 13(15.1)* 15.784 < 0.001* 左房内径增大 2(2.0) 9(5.4) 12(14.0)* 11.267 0.004* 心包积液 6(6.1) 13(7.8) 5(5.8) 0.476 0.788 左室收缩功能障碍 3(3.1) 2(1.2) 3(3.5) - 0.373 室间隔向心性肥厚 2(2.0) 3(1.8) 2(2.3) - 1.000 左室内径增大 1(1.0) 2(1.2) 3(3.5) - 0.430 室壁运动减弱 1(1.0) 3(1.8) 2(2.3) - 0.875 房间隔膨出 1(1.0) 2(1.2) 1(1.2) - 1.000 二尖瓣钙化 0(0.0) 1(0.6) 4(4.7) - 0.023 二尖瓣反流 0(0.0) 2(1.2) 3(3.5) - 0.118 右房内径增大 0(0.0) 0(0.0) 5(5.8)△ - 0.001* 右室内径增大 0(0.0) 0(0.0) 4(4.7)△ - 0.003* 室间隔变薄 0(0.0) 1(0.6) 0(0.0) - 1.000 三尖瓣反流 0(0.0) 0(0.0) 1(1.2) - 0.246 全心扩大 0(0.0) 1(0.6) 0(0.0) - 1.000 颈动脉超声 颈部斑块 6(6.1) 68(41.0)* 58(67.4)*△ 74.737 < 0.001* 双侧颈动脉内膜中层增厚 1(1.0) 18(10.8)* 31(36.0)*△ 48.948 < 0.001* 左侧颈内动脉峰值流速(cm/s) 60.0(47.0,74.0) 53.0(43.0,68.3) 53.0(43.0,67.0) 5.214 0.074 右侧颈内动脉峰值流速(cm/s) 59.0(47.8,74.0) 52.0(43.0,67.3)* 54.5(39.0,69.3) 7.145 0.028 左侧颈内动脉阻力指数 0.6(0.5,0.7) 0.6(0.5,0.7) 0.6(0.6,0.7)*△ 10.594 0.005 右侧颈内动脉阻力指数 0.6(0.5,0.7) 0.6(0.6,0.7) 0.6(0.6,0.7)*△ 13.120 0.001 与青年组比较,*P < 0.01;与中年龄组比较,△P < 0.05;“-”为采用Fisher确切概率法,故无统计值。
下载: 导出CSV
-
[1] 王勇,黄匡时. 全球及中国艾滋病人口规模、空间分布和死亡特征[J]. 人口与社会,2018,34(4):78-88. [2] Jespersen N A,Axelsen F,Dollerup J,et al. The burden of non-communicable diseases and mortality in people living with HIV (PLHIV) in the pre-,early-and late-HAART era[J]. HIV Med,2021,22(6):478-490. doi: 10.1111/hiv.13077 [3] Shah A S V,Stelzle D,Lee K K,et al. Global burden of atherosclerotic cardiovascular disease in people living with HIV:systematic review and meta-analysis[J]. Circulation,2018,138(11):1100-1112. [4] 潘水水,白劲松. HIV/AIDS相关心血管疾病危险因素的研究进展[J]. 皮肤病与性病,2022,44(2):136-142. [5] Kasaie P,Weir B,Schnure M,et al. Integrated screening and treatment services for HIV,hypertension and diabetes in Kenya:assessing the epidemiological impact and cost-effectiveness from a national and regional perspective[J]. J Int AIDS Soc,2020,23(Suppl 1):e25499. [6] 中国艾滋病诊疗指南(2021年版)[J]. 中国艾滋病性病, 2021, 27(11): 1182-1201. [7] Wang R,Vetrano D L,Liang Y,et al. The age-related blood pressure trajectories from young-old adults to centenarians:a cohort study[J]. Int J Cardiol,2019,296(1):141-148. [8] 中国高血压防治指南修订委员会,高血压联盟(中国),中华医学会心血管病分会,等. 中国高血压防治指南(2018年修订版)[J]. 中国心血管杂志,2019,24(1):24-56. doi: 10.3969/j.issn.1007-5410.2019.01.002 [9] 中国医学会糖尿病学分会. 中国2型糖尿病防治指南(2017年版)[J]. 中国实用内科杂志,2018,38(4):292-344. doi: 10.19538/j.nk2018040108 [10] 诸骏仁,高润霖,赵水平,等. 中国成人血脂异常防治指南(2016年修订版)[J]. 中国循环杂志,2016,31(10):937-953. doi: 10.3969/j.issn.1000-3614.2016.10.001 [11] Lumsden R H,Bloomfield G S. The causes of HIV-associated cardiomyopathy:a tale of two worlds[J]. Biomed Res Int,2016,2016(1):8196560-8196568. [12] Kingery J R,Alfred Y,Smart L R,et al. Short-term and long-term cardiovascular risk,metabolic syndrome and HIV in Tanzania[J]. Heart,2016,102(15):1200-1205. doi: 10.1136/heartjnl-2015-309026 [13] McCrary A W,Nyandiko W M,Ellis A M,et al. Early cardiac dysfunction in children and young adults with perinatally acquired HIV[J]. AIDS(London, England),2020,34(4):539-548. [14] 李治军. 颈动脉超声检查在心血管疾病筛查的应用价值[J]. 中外女性健康研究,2018,26(5):186-187. doi: 10.3969/j.issn.2096-0417.2018.05.129 [15] 刘俊,黄瑛,金永梅,等. 昆明地区2013年艾滋病抗病毒治疗患者流行病学特点分析[J]. 皮肤病与性病,2014,36(6):347-348. doi: 10.3969/j.issn.1002-1310.2014.06.016 [16] Pangmekeh P J,Awolu M M,Gustave S,et al. Association between highly active antiretroviral therapy (HAART) and hypertension in persons living with HIV/AIDS at the Bamenda regional hospital,Cameroon[J]. Pan Afr Med J,2019,33:87. [17] McCann K,Shah S,Hindley L,et al. Implications of weight gain with newer anti-retrovirals:10-year predictions of cardiovascular disease and diabetes[J]. AIDS,2021,35(10):1657-1665. [18] Leone S,Lorenzini P,Cozzi-Lepri A,et al. Impact of diabetes on the risk of serious liver events and liver-related deaths in people living with HIV and hepatitis C co-infection:data from the ICONA Foundation Cohort Study[J]. Eur J Clin Microbiol Infect Dis,2019,38(10):1857-1865. doi: 10.1007/s10096-019-03618-8 [19] Mishra TK,Mishra SK,Singh S. Cardiovascular manifestations of people living with HIV/AIDS:Report from a hot spot in eastern India[J]. Indian Heart J,2019,71(4):338-343. doi: 10.1016/j.ihj.2019.09.006 [20] 马彩华,王磊,林雪,等. 人类免疫缺陷病毒感染/艾滋病患者169例的颈动脉超声检查特点及影响因素分析[J]. 中华传染病杂志,2021,39(3):145-151. [21] Sud K,Argulian E. Echocardiography in Patients with HIV Infection[J]. Curr Cardiol Rep,2020,22(9):100. doi: 10.1007/s11886-020-01347-5 [22] 何小清,沈银忠,刘莉,等. 人类免疫缺陷病毒/艾滋病患者心包积液的病因及临床特点分析[J]. 中华传染病杂志,2019,(4):220-222. doi: 10.3760/cma.j.issn.1000-6680.2019.04.006 [23] Badie S M,Rasoulinejad M,Salehi M R,et al. Evaluation of echocardiographic abnormalities in HIV positive patients treated with antiretroviral medications[J]. Infect Disord Drug Targets,2017,17(1):43-51. doi: 10.2174/1871526516666161205124309 [24] Butler J,Greene S J,Shah S H,et al. Diastolic dysfunction in patients with human immunodeficiency virus receiving antiretroviral therapy:results from the CHART study[J]. J Card Fail,2020,26(5):371-380. doi: 10.1016/j.cardfail.2019.10.011 [25] Wubayehu T,Abebe W,Tefera E. Echocardiographic abnormalities in children and adolescents living with human immunodeficiency virus on highly active antiretroviral treatment[J]. Cardiovasc J Afr,2020,31(5):236-240. [26] Woldu B,Temu T M,Kirui N,et al. Diastolic dysfunction in people with HIV without known cardiovascular risk factors in Western Kenya[J]. Open Hear,2022,9(1):e001814. doi: 10.1136/openhrt-2021-001814 [27] Roy Cardinal M H,Durand M,Chartrand-Lefebvre C,et al. Increased carotid artery wall stiffness and plaque prevalence in HIV infected patients measured with ultrasound elastography[J]. Eur Radiol,2020,30(6):3178-3187. doi: 10.1007/s00330-020-06660-9 [28] Godoi E T,Brandt C T,Lacerda H R,et al. Intima-media thickness in the carotid and femoral arteries for detection of arteriosclerosis in human immunodeficiency virus-positive individuals[J]. Arq Bras Cardiol,2017,108(1):3-11. [29] Hanna D B,Jee-Young M,Haberlen S A,et al. Carotid artery atherosclerosis is associated with mortality in HIV-positive women and men[J]. AIDS (London,England),2018,32(16):2393-2403. doi: 10.1097/QAD.0000000000001972 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3438
- HTML全文浏览量: 2085
- PDF下载量: 104
- 被引次数: 0
