

Clinical Study on the Effect of Multimedia Visual Function Training on Amblyopia in Children
-
摘要:
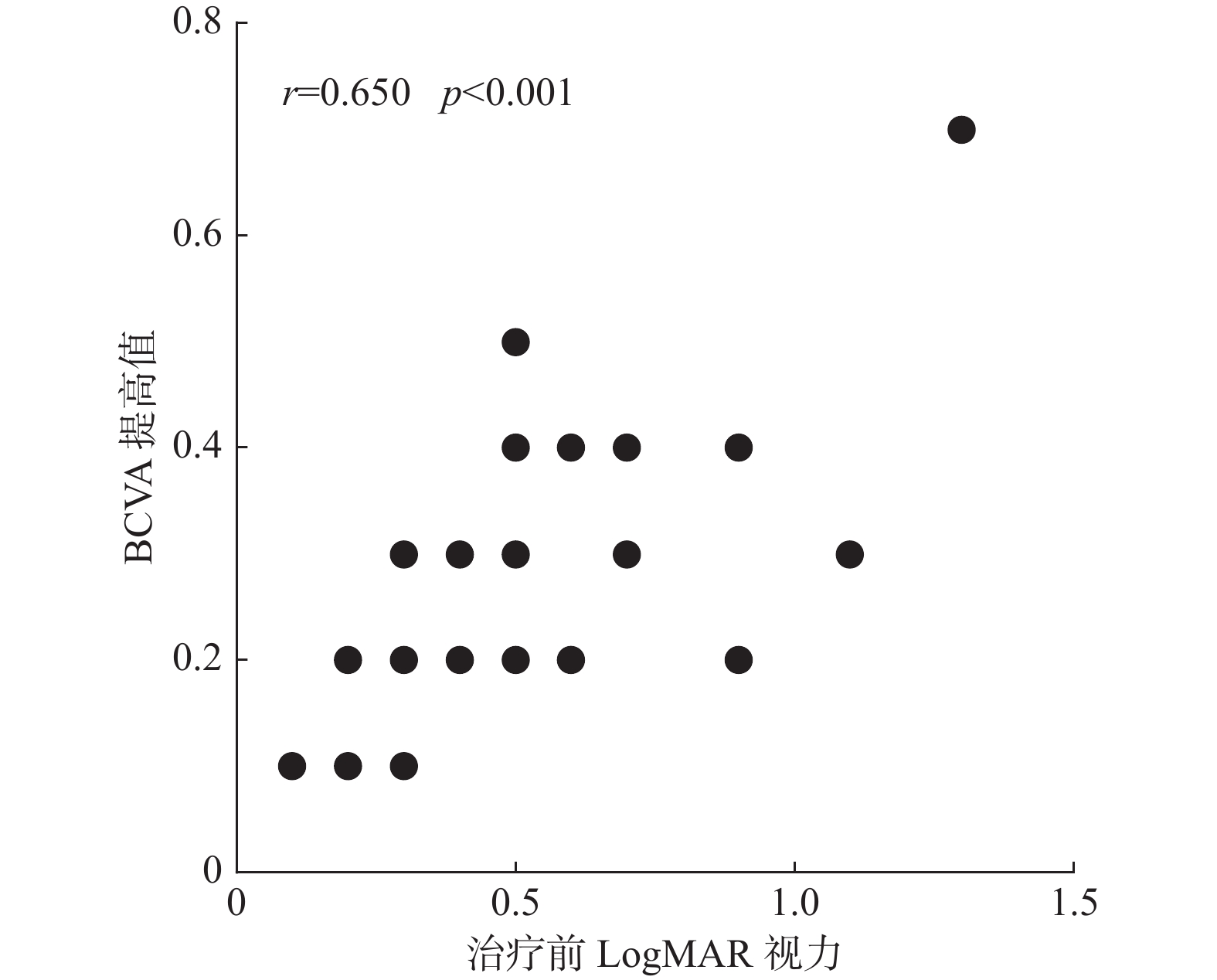
目的 研究多媒体视功能综合训练对儿童弱视的治疗效果并探讨影响治疗效果的因素。 方法 将3~12岁屈光性弱视患者63例(87眼)随机分为观察组与对照组,观察组予多媒体视功能综合训练,对照组予传统精细目力训练,训练时间均为30min/d,共随访6 个月。分别于治疗前、治疗后1月、3月、6月检查最佳矫正视力(BCVA)、Titmus近立体视、图形视觉诱发电位(pVEP)、Worth四点灯,对比2种训练方法在改善儿童弱视患者单眼视力及双眼视功能方面的差异,并采用相关性分析探讨影响多媒体视功能综合训练治疗效果的因素。 结果 (1)观察组及对照组治疗6月后BCVA均较治疗前提高,观察组提高值更大(P < 0.001)。对轻、中度儿童弱视、3~6岁及7~12岁儿童弱视、屈光不正及屈光参差性儿童弱视患者,观察组BCVA提高值均较对照组大(P < 0.05);(2)观察组Titmus近立体视及眼间抑制改善情况均优于对照组(P < 0.05)。(3)观察组治疗后pVEP P100波振幅(15′频率)较治疗前提高(P < 0.001)。(4)影响多媒体视功能综合训练治疗效果的因素:BCVA提高值与治疗前的LogMAR视力呈正相关,与年龄呈负相关;Titmus近立体视治愈率与治疗前的Titmus近立体视呈正相关,与双眼屈光参差量呈负相关。 结论 (1)多媒体视功能综合训练在提高弱视儿童单眼视力及改善双眼视功能方面疗效均优于传统精细目力训练。(2)影响多媒体视功能综合训练治疗效果的因素:BCVA提高值与患者治疗前的视力、年龄具有相关性;Titmus近立体视治愈率与患者治疗前的Titmus近立体视、双眼屈光参差量具有相关性。 -
关键词:
- 儿童弱视 /
- 多媒体视功能综合训练 /
- 传统精细目力训练
Abstract:Objective To study the therapeutic effect of multimedia visual function training on amblyopia in children and explore the factors influencing the therapeutic effect. Methods Sixty-three patients with refractive amblyopia aged 3-12 years (87 eyes) were randomly divided into the observation group and the control group. The observation group received multimedia comprehensive visual function training, and the control group received traditional fine visual training for 30 min/d. A total of 6 months of follow-up were performed. Best corrected visual acuity (BCVA), Titmus near-stereoscopic vision, pVEP and Worth four-point lamp were examined before treatment, 1 month, 3 months and 6 months after treatment, respectively. The differences of monocular visual acuity and binocular visual function in children with amblyopia were compared between the two training methods. Correlation analysis was used to explore the factors influencing the therapeutic effect of multimedia visual function training. Results 1. BCVA in the observation group and the control group increased 6 months after treatment compared with that before treatment, and the increase value in the observation group was greater (P < 0.001). For mild and moderate amblyopia, amblyopia, ametropia and anisometropia in children aged 3-6 years and 7-12 years, BCVA in observation group was higher than that in control group (P < 0.05). 2. The improvement of Titmus near stereo vision and interocular inhibition in the observation group was better than that in the control group (P < 0.05). 3. The amplitude of pVEP P100 wave (15’frequency) in the observation group increased after treatment compared with before treatment (P < 0.001). 4. Factors influencing the therapeutic effect of multimedia visual function training: BCVA increased value was positively correlated with LogMAR visual acuity before treatment, negatively correlated with age; The cure rate of Titmus near stereo was positively correlated with Titmus near stereo before treatment, but negatively correlated with binocular anisometropia. Conclusions 1. Multimedia comprehensive visual function training is better than traditional fine visual training in improving monocular vision and binocular visual function in amblyopia children. 2. Factors influencing the therapeutic effect of multimedia visual function training: BCVA improvement was correlated with the visual acuity before treatment and age; The cure rate of Titmus near stereo vision was correlated with the Titmus near stereo vision and binocular anisometropia before treatment. -
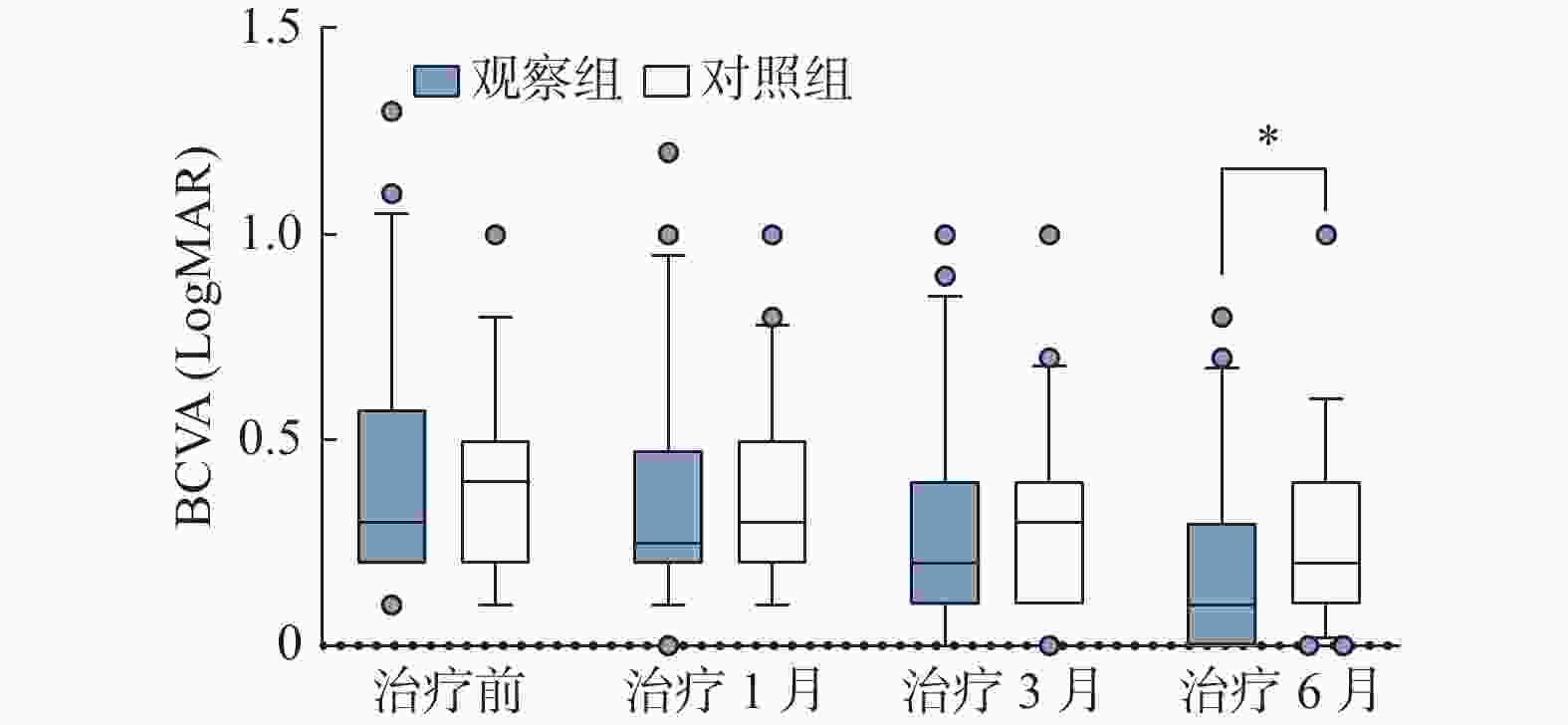
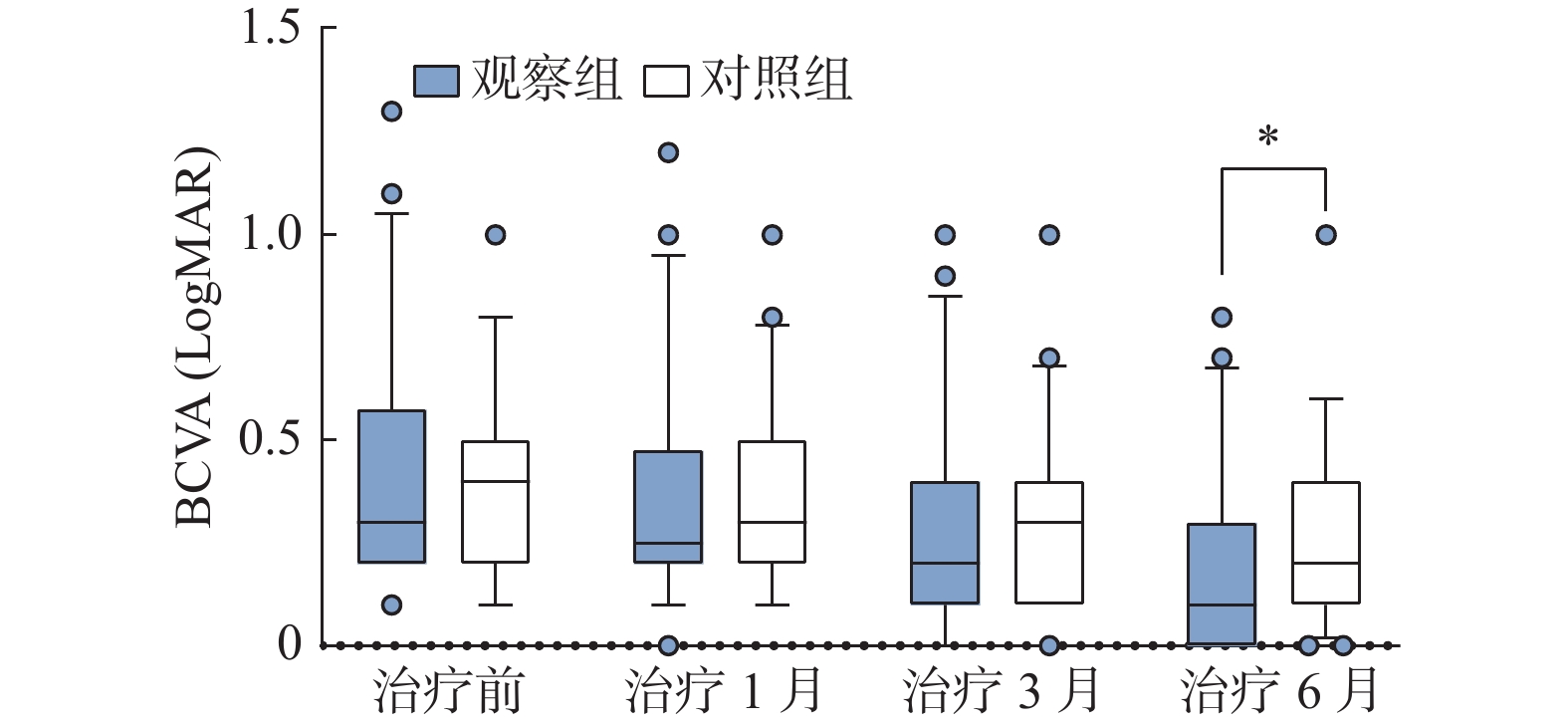
图 1 观察组与对照组BCVA变化图
*P < 0.05。
Figure 1. BCVA changes of observation group and control group
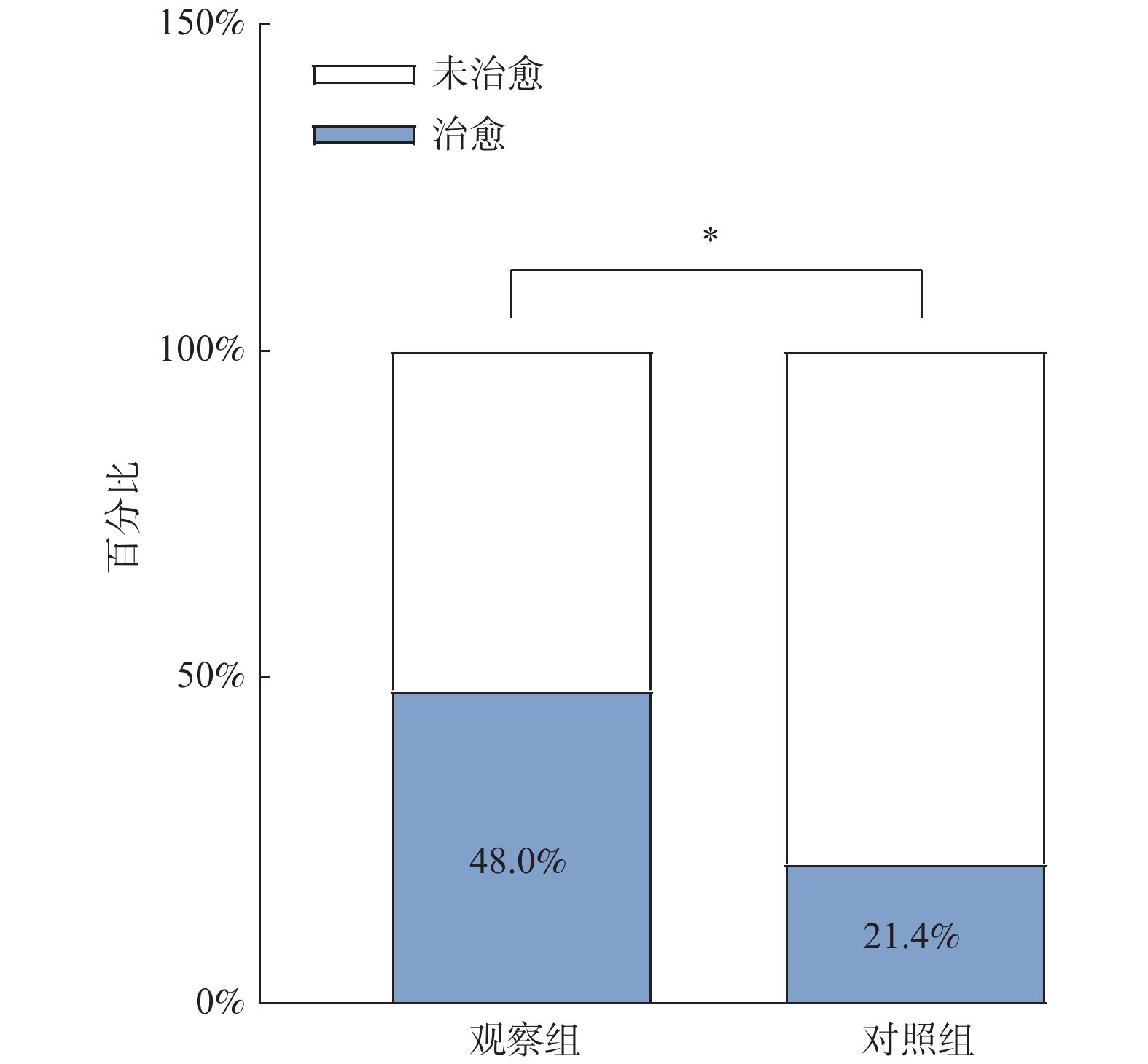
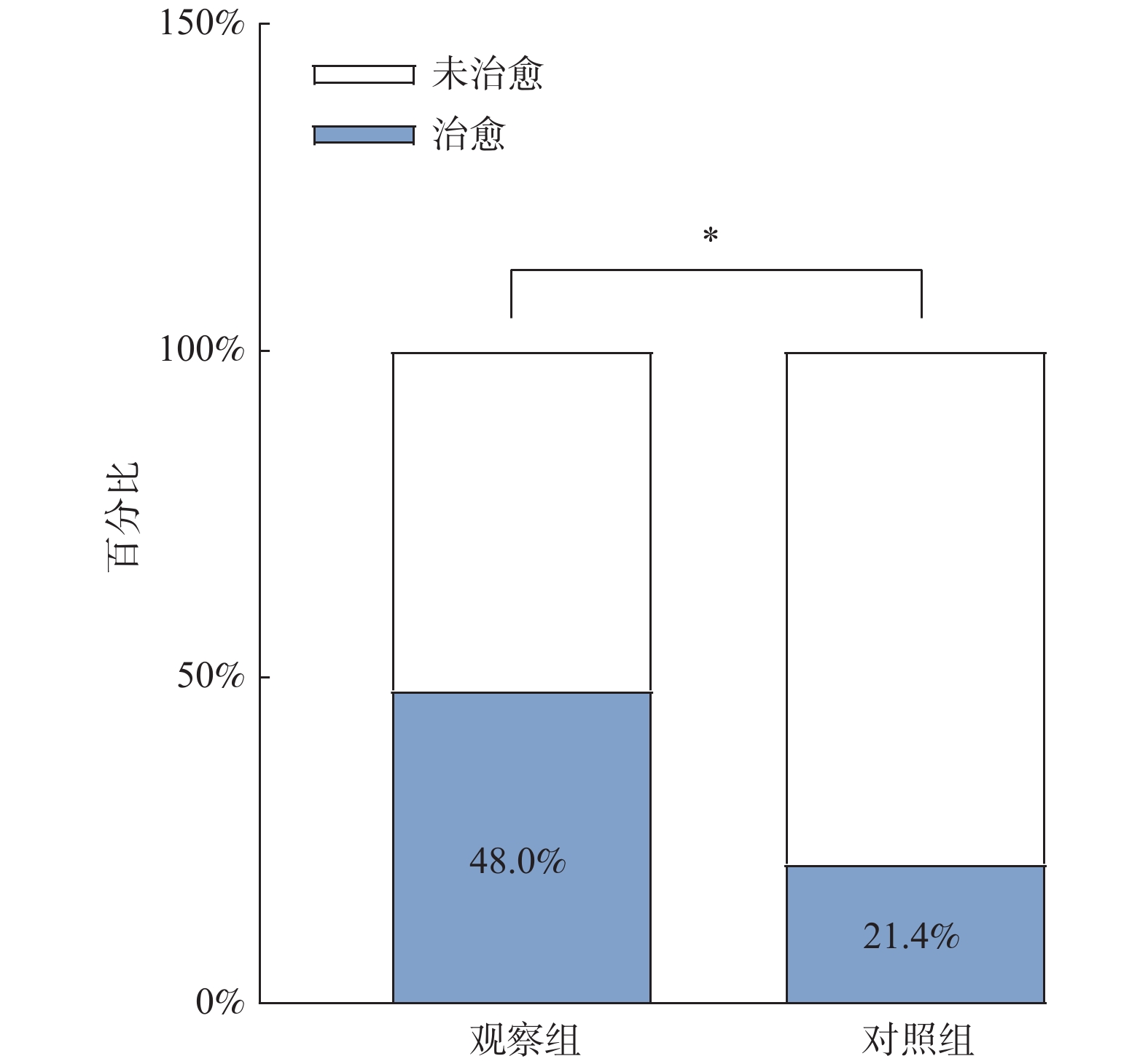
图 2 观察组与对照组立体视治愈率对比图
观察组立体视治愈率高于对照组,*P < 0.05。
Figure 2. Contrast chart of stereo cure rate between observation group and control
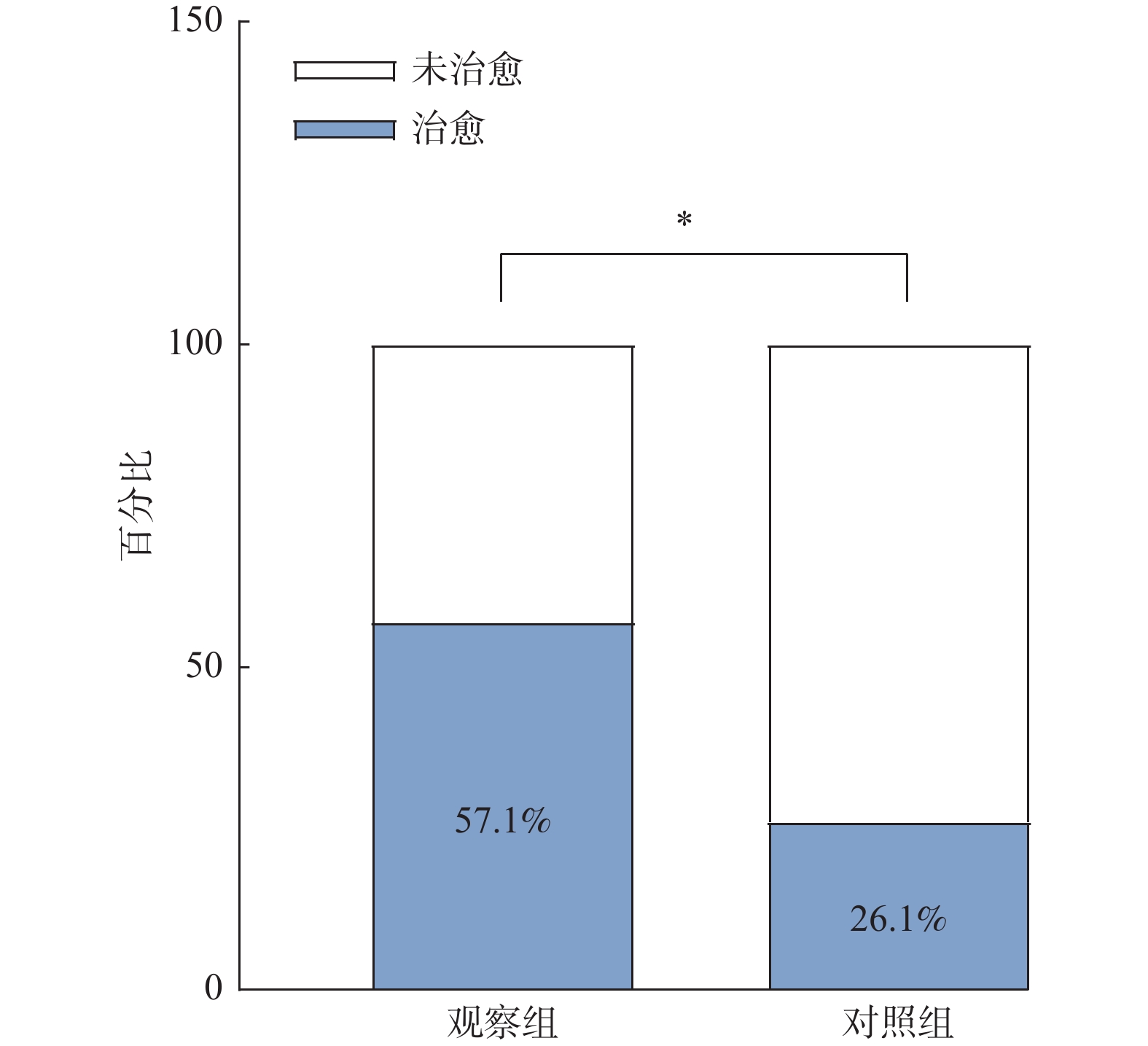
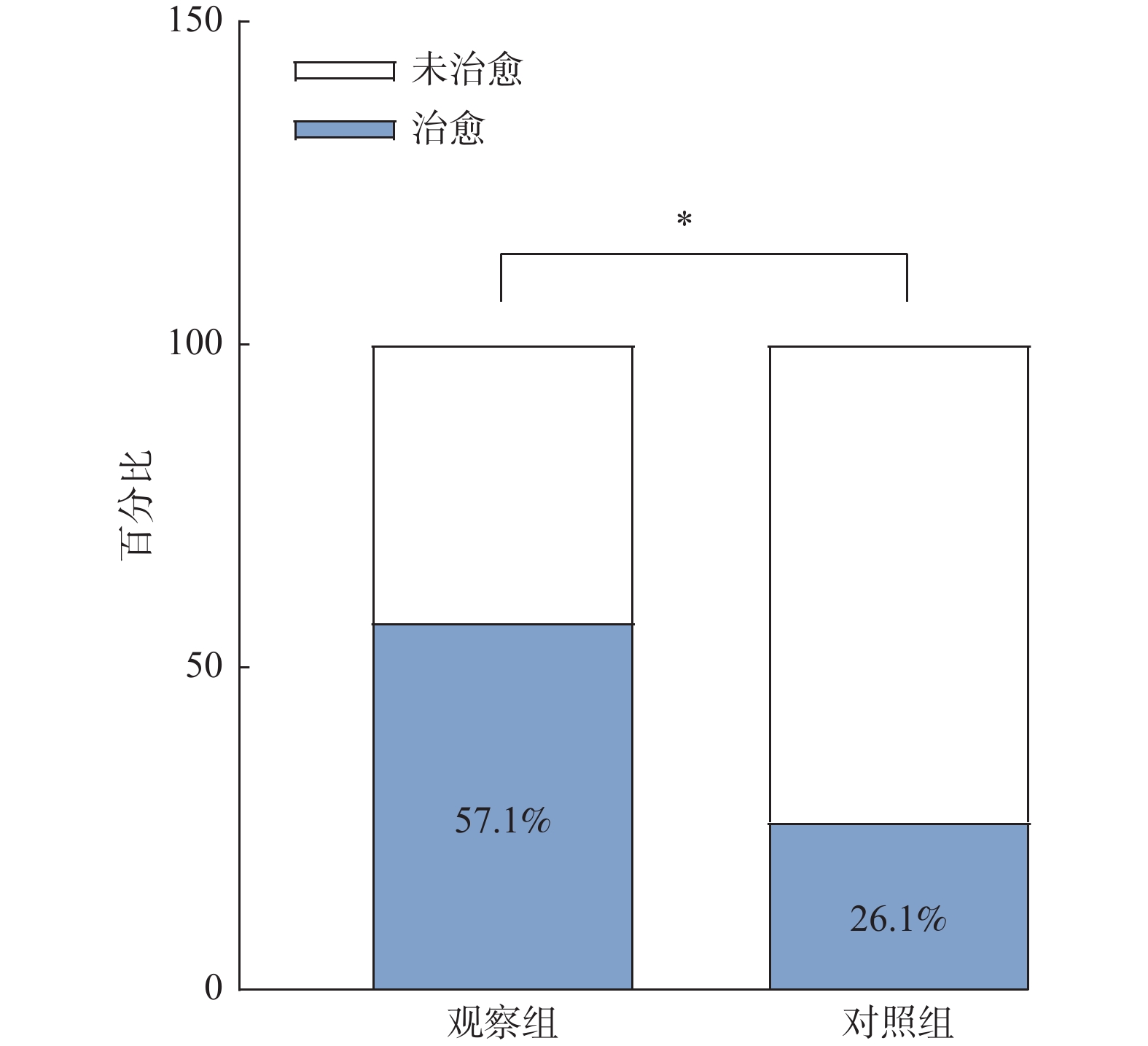
图 3 观察组与对照组眼间抑制治愈率比较图
观察组眼间治愈率高于于对照组,*P < 0.05。
Figure 3. Comparison of interocular inhibition cure rate between the observation group and the control
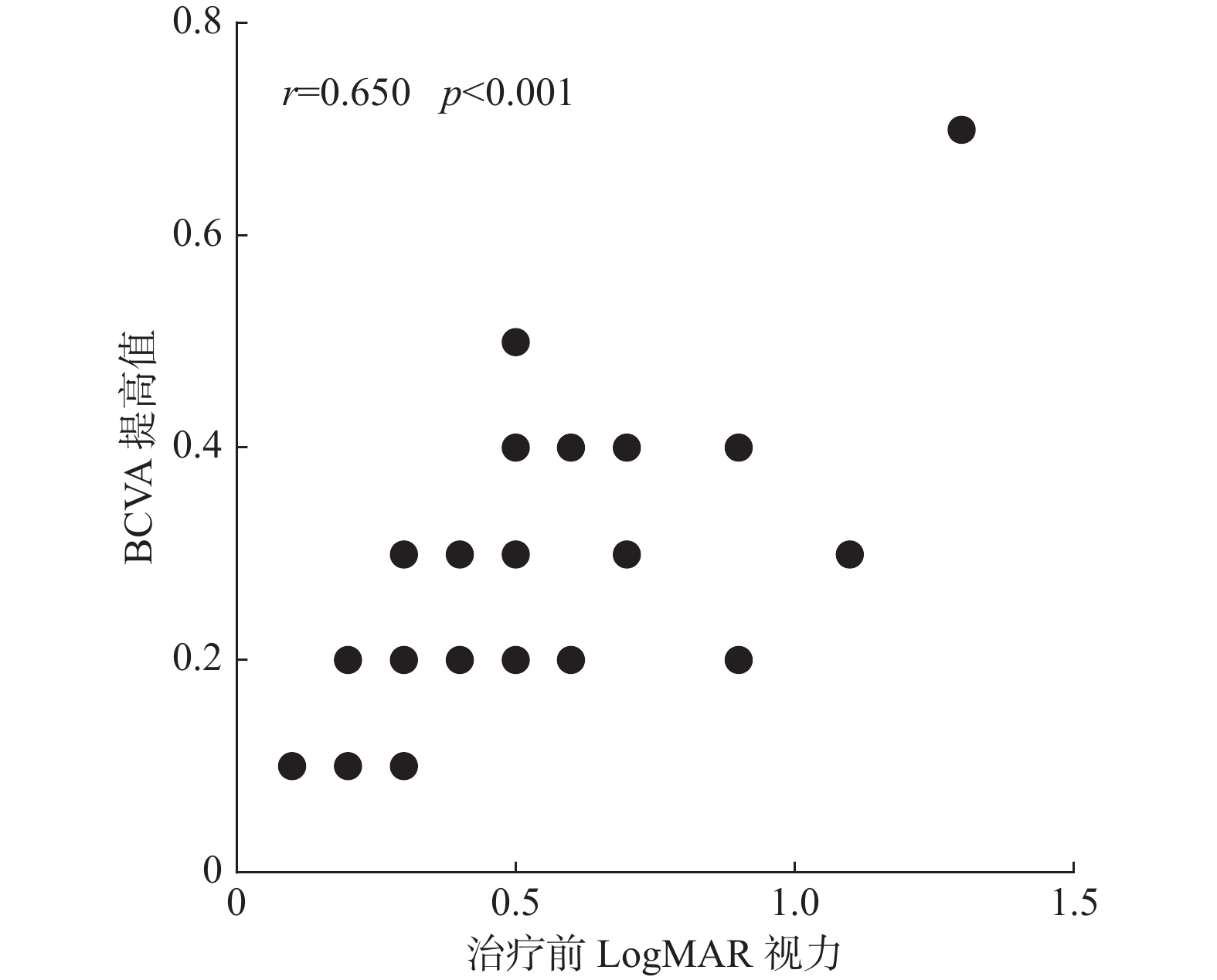
图 4 观察组BCVA提高值与治疗前LogMAR视力相关性视点图
Figure 4. Scatter plot of the correlation between BCVA improvement and LogMAR vision before treatment in the observation group
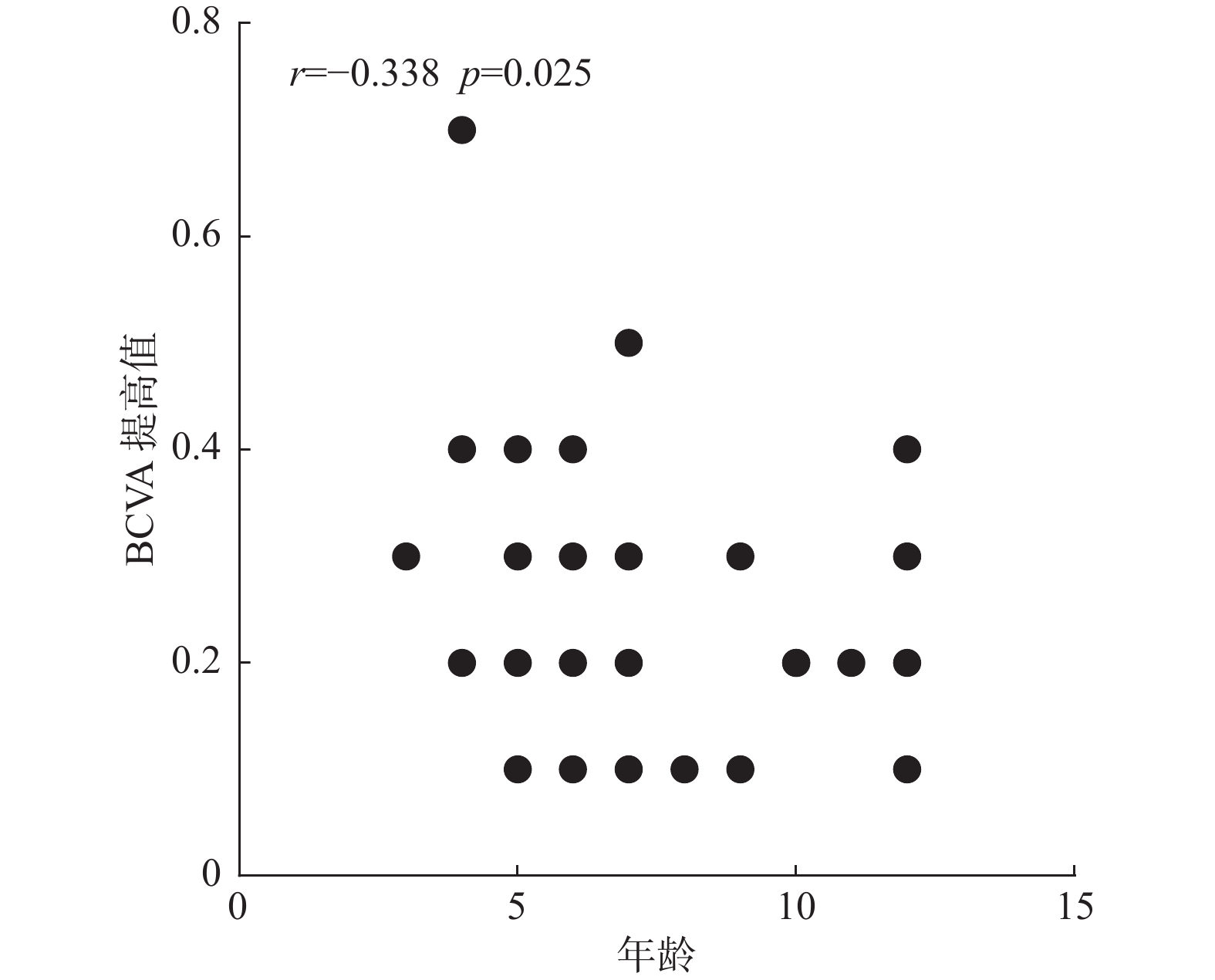
图 5 观察组BCVA提高值与年龄相关性散相关性散点图
Figure 5. Scatter plot of BCVA improvement and age in observation group
表 1 2组患者一般资料基线比较[n(%)]
Table 1. Baseline comparison of general data between the two groups [n(%)]
基线资料 观察组 对照组 χ2/Z P 性别(例) 男(n = 29) 12(37.5) 17(54.8) 1.905 0.167 女(n = 34) 20(62.5) 14(45.2) 年龄(岁) 3~6(n = 27) 15(46.9) 12(38.7) 0.429 0.513 7~14(n = 36) 17(53.1) 19(61.3) 弱视类型(眼数) 屈光不正性弱视(n = 52) 27(61.4) 25(58.1) 0.094 0.759 屈光参差性弱视(n = 35) 17(38.6) 18(41.9) 弱视程度(眼数) 轻度(n = 22) 12(27.3) 10(23.3) −0.196 0.845 中度(n = 56) 27(61.4) 29(67.4) 重度(n = 9) 5(11.3) 4(9.3)  下载: 导出CSV
下载: 导出CSV
表 2 2组患者视力恢复情况[M(P25,P75)]
Table 2. Visual acuity recovery in two groups [M(P25,P75)]
组别 时间 χ2 P 治疗前 治疗1月 治疗3月 治疗6月 观察组 0.30(0.20,0.58) 0.25(0.20,0.48) 0.20(0.20,0.40) 0.10(0.00,0.30) 191.607 < 0.001*** 对照组 0.40(0.20,0.50) 0.30(0.20,0.50) 0.30(0.10,0.40) 0.20(0.10,0.40) 68.719 < 0.001*** 统计量 0.572 0.199 0.905 4.866* − − P 0.449 0.656 0.341 0.027 − − *P < 0.05,***P < 0.001。
下载: 导出CSV
表 3 2组不同弱视程度BCVA提高值组间对比[M(P25,P75)]
Table 3. Comparison of BCVA enhancement value between two groups with different amblyopia degree[M(P25,P75)]
分组 轻度弱视 中度弱视 重度弱视 观察组(n = 44) 0.15(0.10,0.20) 0.30(0.20,0.30) 0.40(0.25,0.55) 对照组(n = 43) 0.10(0.00,0.10) 0.10(0.05,0.20) 0.20(0.05,0.35) Z −2.926** −4.625*** −1.521 P 0.003 < 0.001 0.128 Z值与P值为2组治疗6月较治疗前BCVA提高值比较所得,**P < 0.01,***P < 0.001。
下载: 导出CSV
表 4 2组不同年龄段BCVA提高值组间对比[M(P25,P75)]
Table 4. Comparison of BCVA increased value between two groups at different ages[M(P25,P75)]
组别 3-6岁 7-12岁 观察组(n = 44) 0.30(0.20,0.35) 0.20(0.10,0.30) 对照组(n = 43) 0.15(0.10,0.20) 0.10(0.00,0.10) Z −3.076** −4.145*** P 0.002 < 0.001 **P < 0.01,***P < 0.001。
下载: 导出CSV
表 5 2组不同弱视类型BCVA提高值组间对比[M(P25,P75)]
Table 5. Comparison of BCVA enhancement values between two groups with different amblyopia types[M(P25,P75)]
组别 屈光不正性弱视 屈光参差性弱视 观察组(n = 44) 0.20(0.20,0.30) 0.30(0.15,0.40) 对照组(n = 43) 0.10(0.00,0.20) 0.10(0.10,0.20) Z −3.808 −3.284 P < 0.001*** 0.001** **P < 0.01,***P < 0.001。
下载: 导出CSV
表 6 2组治疗前及治疗6月Titmus近立体视情况(n)
Table 6. The nearstereoscopic vision of Titmus in both groups before and 6 months after treatment (n)
组别 ≤60″ 100″ 160″ 200″ 400″ > 400″ Z P 观察组(n = 32) 治疗前 7 6 1 3 3 12 - - 治疗6月 19 6 1 1 2 3 −3.394** 0.001 对照组(n = 31) 治疗前 3 6 0 2 9 11 - - 治疗6月 9 10 0 1 6 5 −2.557* 0.011 *P < 0.05,**P < 0.01。
下载: 导出CSV
表 7 2组患者治疗前后P100波潜伏期变化[M(P25,P75)]
Table 7. Changes of P100 wave latency before and after treatment in two groups [M(P25,P75)]
刺激频率 组别 治疗前 治疗6月 Z P 1°刺激 观察组(n = 43) 106.30(103.30,108.60) 103.90(101.60,111.50) −0.688 0.491 对照组(n = 40) 107.75(101.53,112.85) 106.30(102.85,114.95) −0.021 0.983 15′刺激 观察组(n = 43) 115.70(108.60,121.50) 115.20(110.10,120.40) −0.924 0.355 对照组(n = 40) 115.45(108.68,122.60) 115.75(110.03,123.70) −0.773 0.440
下载: 导出CSV
表 8 2组患者治疗前与治疗6月后P100波振幅变化[M(P25,P75)]
Table 8. P100 wave amplitude changes before and 6 months after treatment in two groups [M(P25,P75)]
刺激频率 组别 治疗前 治疗6月 Z P 1°刺激 观察组(n = 43) 17.40(7.62,22.9) 18.60(8.12,26.20) −1.365 0.172 对照组(n = 40) 17.55(7.74,21.83) 18.70(11.38,21.43) −0.874 0.382 15′刺激 观察组(n = 43) 12.90(7.40,19.50) 17.10(12.80,27.50) −3.568 < 0.001*** 对照组(n = 40) 13.60(8.22,19.55) 14.45(8.62,21.43) −0.712 0.476 ***P < 0.001。
下载: 导出CSV
-
[1] 杨培增, 范先群. 眼科学[M]. 第9版, 北京: 人民卫生出版社, 2018: 253-254. [2] Fu Z,Hong H,Su Z,et al. Global prevalence of amblyopia and disease burden projections through 2040:a systematic review and meta-analysis[J]. Br J Ophthalmol,2020,104(8):1164-1170. doi: 10.1136/bjophthalmol-2019-314759 [3] Portela-Camino J A,Martín-González S,Ruiz-Alcocer J,et al. A Random Dot Computer Video Game Improves Stereopsis[J]. Optom Vis Sci,2018,95(6):523-535. doi: 10.1097/OPX.0000000000001222 [4] Barollo M,Contemori G,Battaglini L,et al. Perceptual learning improves contrast sensitivity,visual acuity,and foveal crowding in amblyopia[J]. Restor Neurol Neurosci,2017,35(5):483-496. [5] Li S L,Jost R M,Morale S E,et al. A binocular iPad treatment for amblyopic children[J]. Eye (Lond),2014,28(10):1246-1253. doi: 10.1038/eye.2014.165 [6] Pediatric Eye Disease Investigator Group. A randomized trial of binocular dig rush game treatment for amblyopia in children aged 7 to 12 years[J]. Ophthalmology,2019,126(3):456-466. doi: 10.1016/j.ophtha.2018.10.032 [7] Zhai J,Chen M,Liu L,et al. Perceptual learning treatment in patients with anisometropic amblyopia:a neuroimaging study[J]. Br J Ophthalmol,2013,97(11):1420-1424. doi: 10.1136/bjophthalmol-2013-303778 [8] Legge G E. Spatial frequency masking in human vision:binocular interactions[J]. J Opt Soc Am,1979,69(6):838-847. doi: 10.1364/JOSA.69.000838 [9] 李少敏. 双眼分别同时视训练治疗弱视进展[J]. 中国斜视与小儿眼科杂志,2020,28(2):33-37. doi: 10.3969/J.ISSN.1005-328X.2020.02.014 [10] Baker D H,Meese T S,Mansouri B,et al. Binocular summation of contrast remains intact in strabismic amblyopia[J]. Invest Ophthalmol Vis Sci,2007,48(11):5332-5338. doi: 10.1167/iovs.07-0194 [11] Kelly K R,Jost R M,Wang Y Z,et al. Improved Binocular Outcomes Following Binocular Treatment for Childhood Amblyopia[J]. Invest Ophthalmol Vis Sci,2018,59(3):1221-1228. doi: 10.1167/iovs.17-23235 [12] Birch E E,Li S L,Jost R M,et al. Binocular iPad treatment for amblyopia in preschool children[J]. J AAPOS,2015,19(1):6-11. doi: 10.1016/j.jaapos.2014.09.009 [13] Murray S J,Codina C J. The Role of Binocularity in Anisometropic Amblyopia[J]. J Binocul Vis Ocul Motil,2019,69(4):141-152. doi: 10.1080/2576117X.2019.1656034 [14] 韦仕岗,蓝剑青,谢文娟,等. 虚拟现实视感知觉平台在近视性屈光参差性弱视患者立体视功能可塑性的临床应用研究[J]. 中国斜视与小儿眼科杂志,2019,27(4):13-15. doi: 10.3969/J.ISSN.1005-328X.2019.04.004 [15] Hess R F,Mansouri B,Thompson B. Restoration of binocular vision in amblyopia[J]. Strabismus,2011,19(3):110-118. doi: 10.3109/09273972.2011.600418 [16] 黄杰,叶翔,李国平,等. 屈光参差性弱视儿童治疗后双眼视觉输入平衡分析[J]. 眼科新进展,2016,36(7):626-629,633. doi: 10.13389/j.cnki.rao.2016.0166 -


 点击查看大图
点击查看大图
计量
- 文章访问数: 3616
- HTML全文浏览量: 2038
- PDF下载量: 28
- 被引次数: 0
