

Imaging Measurement of Intramedullary Nail Design for Proximal Fifth Metatarsal Fracture
-
摘要:
目的 采用X线测量正常成人第5跖骨髓腔大小、髓内钉长度及第5跖骨长度,为第5跖骨近端骨折髓内钉直径与长度选择提供依据。 方法 回顾性选择120例至云南省中医医院就诊,男女各60例,(19~79)岁,符合纳入标准并行足部X片检查的患者,测量第5跖骨正斜位髓腔直径,正位长度、髓内钉长度(从第5跖骨基底部至跖骨干弯曲的距离)。测量结果使用SPSS26.0统计学软件包进行统计学分析,正态分布计量资料2组组间比较采用两独立样本t检验,相关性分析采用Pearson相关性分析,P < 0.05表示差异有统计学意义。 结果 正位髓腔直径平均值为4.15 mm范围(2.24~5.64) mm,斜位第5跖骨髓腔直径平均值为4.31 mm范围(3.18~5.81) mm,髓内钉长度平均值为39.74 mm范围(28.07~53.46) mm,第5跖骨长度平均值71.64 mm范围(59.73~85.44) mm,髓内钉长度与第5跖骨长度比值平均值为55.48%范围(41.12~68.05)%。经t检验证实男性与女性年龄差异无统计学意义(P > 0.05),男性和女性正斜位髓腔直径、跖骨长度、髓内钉长度,差异有统计学意义(P < 0.05),髓内钉长度与第5跖骨长度比值无统计学意义(P > 0.05)。Pearson相关性分析:男性和女性在跖骨长度与髓内钉长度和第5跖骨长度的比值均无相关性(P > 0.05)。 结论 通过保持髓内钉长度小于第5跖骨长度的55.48%,可以避免髓内钉长度过长。由于大多数患者正斜位髓腔直径 > 4 mm,因此可能需要一个直径 > 4 mm的髓内钉来提供足够的固定和减少并发症。 Abstract:Objective To measure the size of the fifth metatarsal bone marrow cavity, the length of the intramedullary nail and the length of the fifth metatarsal bone in normal adults by X-ray, and to provide a basis for the selection of the diameter and length of the intramedullary nail for the proximal fifth metatarsal fracture. Methods 120 patients, 60 males and 60 females, aged from 19 to 79 years old, who met the inclusion criteria and underwent foot X-ray examination, were selected from Yunnan Traditional Chinese Medicine Hospital. The diameter of the medullary cavity, the length of the anteroposterior position, and the length of the intramedullary nail (the distance from the base of the fifth metatarsal bone to the bending of the metatarsal shaft) were measured. SPSS26.0 statistical software package was used for statistical analysis of measurement results. Two independent samples of t-test were used for comparison between two groups of normal distribution measurement data. Pearson correlation analysis was used for correlation analysis. P < 0.05 indicated that there was a statistically significant difference. Results The average diameter of the medullary cavity in the anteroposterior position was 4.15 mm (2.24 mm~5.64 mm), the average diameter of the fifth metatarsal cavity in the oblique position was 4.31 mm (3.18 mm~5.81 mm), the average length of intramedullary nails was 39.74 mm (28.07 mm~53.46 mm), the average length of the fifth metatarsal was 71.64 mm (59.73 mm~85.44 mm), and the average ratio of the length of intramedullary nails to the length of the fifth metatarsal was 55.48% (41.12%~68.05%). The t-test confirmed that there was no significant difference in ages between men and women (P > 0.05). The diameter of the medullary cavity, the length of the metatarsal bone, and the length of the intramedullary nail in the positive and oblique positions of men and women were statistically significant (P < 0.05). The ratio of the length of the intramedullary nail to the length of the fifth metatarsal bone was not statistically significant (P > 0.05). Pearson correlation analysis: There was no correlation between the metatarsal length and the ratio of intramedullary nail length to the fifth metatarsal length in men and women (P > 0.05). Conclusion By keeping the length of the intramedullary nail less than 55.48% of the length of the fifth metatarsal bone, the excessive length of the intramedullary nail can be avoided. Since the diameter of the medullary cavity in the positive and oblique position of most patients is greater than 4 mm, an intramedullary nail with a diameter greater than 4 mm may be required to provide adequate fixation and reduce complications. -
Key words:
- Fifth metatarsal proximal fracture /
- Intramedullary nail /
- Imaging /
- Measure
-

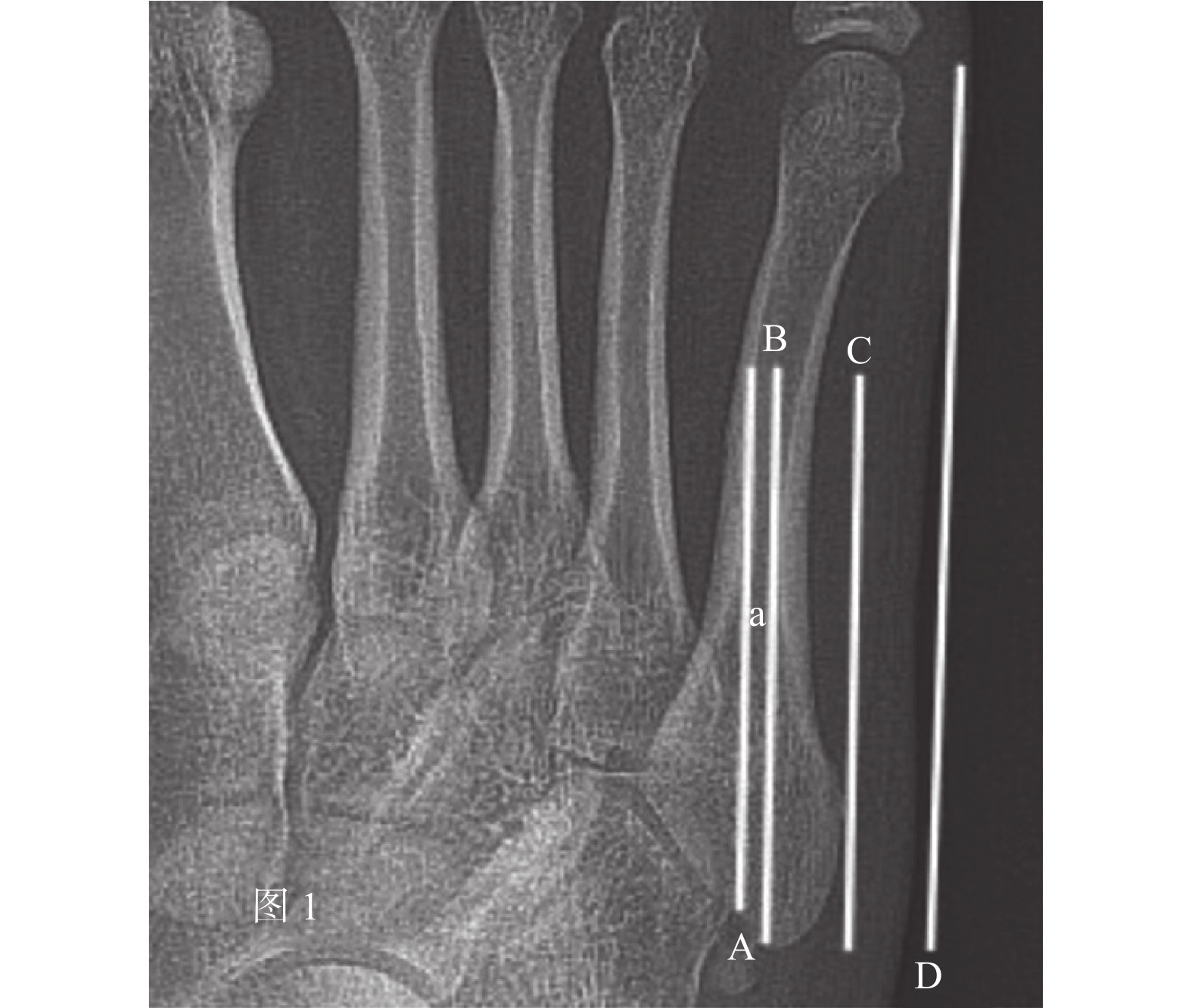
图 1 正位第5跖骨髓腔直径、髓内钉长度、第5跖骨长度测量
A:第5跖骨髓腔直径内侧线;B:第5跖骨髓腔直径外侧线;C:髓内钉长度线;D:第5跖骨长度线。
Figure 1. Measurement of the diameter of the medullary cavity,the length of intramedullary nail and the length of the fifth metatarsal bone

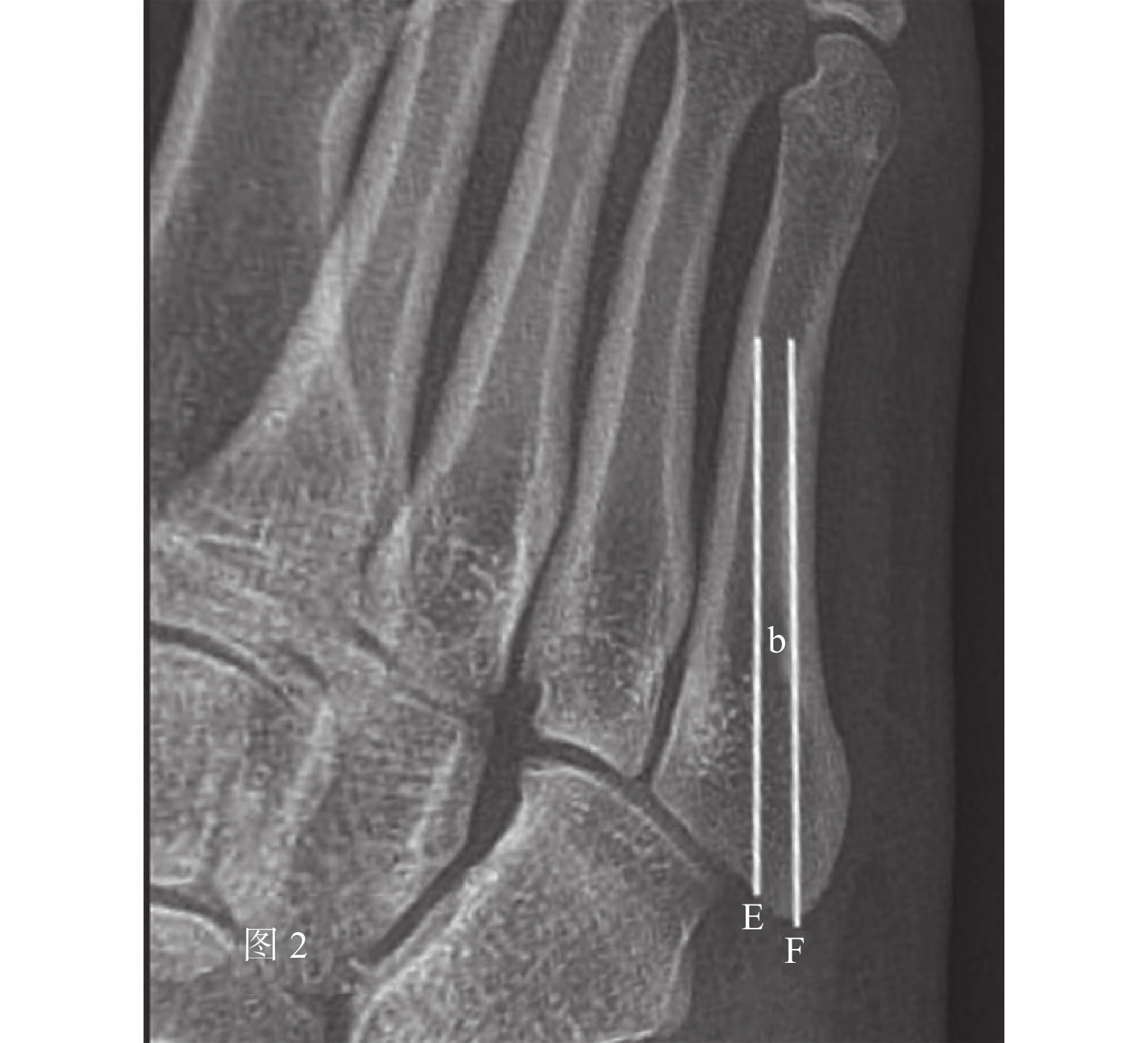
图 2 斜位第 5 跖骨髓腔直径测量
E:第5跖骨髓腔直径内侧线;F:第5跖骨髓腔直径外侧线。
Figure 2. Measurement of the diameter of the fifth metatarsal medullary cavity in oblique position
表 1 基础数据描述
Table 1. Description of basic data
指标 平均值 中位数 最大值 最小值 标准差 年龄 43.79 40.00 79 19 16.40 a(mm) 4.15 4.10 5.64 2.24 0.58 b(mm) 4.31 4.26 5.81 3.18 0.69 c(mm) 39.74 39.58 53.46 28.07 4.80 d(mm) 71.64 71.42 85.44 59.73 5.78 e(%) 55.48 55.07 68.05 41.12 5.10 a:正位第5跖骨髓腔直径;b:斜位第5跖骨髓腔直径;c:髓内钉长度;d:第5跖骨长度;e:髓内钉长度与第5跖骨长度比值。  下载: 导出CSV
下载: 导出CSV
表 2 男性和女性各资料比较(
$ \bar x \pm s $ )Table 2. Comparison of male and female data (
$ \bar x \pm s $ )指标 男性组 女性组 t P 年龄 46.03 ± 17.92 41.55 ± 14.53 1.505 0.135 a(mm) 4.31 ± 0.56 3.99 ± 0.56 3.082 0.003* b(mm) 4.46 ± 0.64 4.17 ± 0.50 2.717 0.008 c(mm) 41.25 ± 4.64 38.23 ± 4.51 3.609 < 0.001* d(mm) 75.04 ± 4.68 68.23 ± 4.68 7.977 < 0.001* e(%) 54.95 ± 4.99 56.01 ± 5.30 −1.139 0.257 a:正位第5跖骨髓腔直径;b:斜位第5跖骨髓腔直径;c:髓内钉长度;d:第5跖骨长度;e:髓内钉长度与第5跖骨长度比值。*P < 0.05。
下载: 导出CSV
表 3 男性和女性d与e相关性分析
Table 3. Correlation analysis of d and e between men and women
性别 r P 男 0.03 0.799 女 0.05 0.694
下载: 导出CSV
-
[1] Bušková K,Bartoníček J,Rammelt S. Fractures of the base of the fifth metatarsal bone: A critical analysis review[J]. JBJS Rev,2021,9(10):10. [2] Lawrence S J,Botte M J. Jones' fractures and related fractures of the proximal fifth metatarsal[J]. Foot Ankle,1993,14(6):358-365. doi: 10.1177/107110079301400610 [3] Coleman M M,Guyton G P. Jones fracture in the nonathletic population[J]. Foot Ankle Clin,2020,25(4):737-751. doi: 10.1016/j.fcl.2020.08.012 [4] Ruta D J,Parker D. Jones fracture management in athletes[J]. Orthop Clin North Am,2020,51(4):541-553. doi: 10.1016/j.ocl.2020.06.010 [5] Zhang Z,Lyu X,Duan J H. Diagnosis and treatment of proximal fifth metatarsal fracture[J]. Zhongguo Gu Shang,2019,32(1):88-91. [6] Porter D A,Klott J. Proximal fifth metatarsal fractures in Athletes: Management of acute and chronic conditions[J]. Foot Ankle Clin,2021,26(1):35-63. doi: 10.1016/j.fcl.2020.10.007 [7] Ochenjele G,Ho B,Switaj P J,et al. Radiographic study of the fifth metatarsal for optimal intramedullary screw fixation of Jones fracture[J]. Foot Ankle Int,2015,36(3):293-301. doi: 10.1177/1071100714553467 [8] 刘宇航,王建华. 钩钢板与空心螺钉固定第五跖骨基底Ⅰ区骨折的比较[J]. 中国矫形外科杂志,2021,29(14):1286-1290. [9] Patel K A,Christopher Z K,Hubbard C E,et al. Stress fractures of the fifth metatarsal in athletes[J]. J Am Acad Orthop Surg,2021,29(12):507-517. doi: 10.5435/JAAOS-D-20-01060 [10] Ryan T J,Tarrant S M,Fraser E J,et al. Jones fracture treatment: A novel surgical technique and case series[J]. Foot Ankle Spec,2022,15(4):354-360. doi: 10.1177/1938640020953029 [11] Metzl J A,Bowers M W,Anderson R B. Fifth metatarsal Jones fractures: Diagnosis and treatment[J]. J Am Acad Orthop Surg,2022,30(4):e470-e479. doi: 10.5435/JAAOS-D-21-00542 [12] 邓晋京,黄敬,王庆华. 经皮空心螺钉固定治疗第5跖骨基底部骨折[J]. 临床骨科杂志,2020,23(5):722. doi: 10.3969/j.issn.1008-0287.2020.05.040 [13] 桑辉,陈永忠,刘业伟,等. 跗跖关节正斜位摄影技术临床初步应用研究[J]. 实用放射学杂志,2020,36(11):1849-1852. doi: 10.3969/j.issn.1002-1671.2020.11.036 [14] 潘斯学,保超宇,夏吉良,等. 正常成人喙突的64排128层螺旋CT数字影像资料的回顾性研究[J]. 昆明医科大学学报,2022,43(10):84-89. doi: 10.12259/j.issn.2095-610X.S20221017 -



 点击查看大图
点击查看大图
计量
- 文章访问数: 5483
- HTML全文浏览量: 2513
- PDF下载量: 11
- 被引次数: 0
