

Analysis of Clinical Data of 471 Elderly Patients Hospitalized with Burns
-
摘要:
目的 通过对老年烧伤患者临床资料回顾性分析,为老年烧伤防治领域提供切实依据。 方法 回顾性分析昆明医科大学第二附属医院2014年1月至2020年12月收治的符合入选标准的老年烧伤患者的病历资料,包括性别、年龄、慢性病、居住地点、致伤地点、院前急救创面处理方式、就医途径、致伤原因、发病季节、烧伤部位、烧伤面积、烧伤深度、烧伤严重程度、治疗方式、住院时间、临床转归、死亡患者分析、住院费用等情况。对数据行卡方拟合优度检验、χ2检验、线性关联、Fisher确切概率检验、秩和检验、多因素Cox回归分析、多元线性回归分析。 结果 (1)符合入选标准的患者共471例,随年份增长,老年患者占同期住院患者比例总体呈上升趋势(P < 0.01)。男女比例为1.75∶1(300/171),男性明显多于女性(P < 0.001);患者年龄分布为69(64,77)岁。总计247例(52.44%)患者合并慢性病,常见慢性病依次为高血压141例次(33.41%)、糖尿病71例次(16.82%)、陈旧性脑梗死51例次(12.09%)。(2)居于农村者显著多于城市,家中烧伤显著多于公共场所(P < 0.05)。院前急救中有381例(80.89%)患者创面未经任何处理;经120救治仅34例;常见致伤原因为火焰烧伤274例(58.17%)、热液烫伤155例(32.91%)。7 a间入院人数最多的是冬季(168例,35.67%)和春季(130例,27.60%)。常见烧伤部位依次为下肢350例次(74.31%)、上肢230例次(48.83%)。烧伤总面积≤10%TBSA 272例(57.75%),其中合并Ⅲ度烧伤170例(占总人数的36.09%)。烧伤严重程度由多到少依次为中度234例(49.68%)、轻度102例(21.66%)、重度80例(16.99%)、特重度55例(11.68%)。(3)入组患者最终治愈好转288例(61.15%)、自动出院164例(34.82%)、死亡19例(4.03%)。年龄、烧伤总面积、Ⅲ度烧伤面积、吸入性损伤、伤后并发症、合并慢性病是影响老年患者死亡的独立危险因素(P < 0.05)。住院时间11(5,22) d,住院费用14 320.62(6 347.92,39 638.06)元,因住院费用呈偏态分布,取其对数后受住院时间、烧伤总面积、Ⅲ度烧伤面积、治疗方式、并发症影响。 结论 老年烧伤好发于冬春季农村家中,男性居多,以火焰烧伤、热液烫伤为主。患者多为年轻老人(60~74岁),小面积深度烧伤多见,集中于下肢和上肢,治疗费用高。多数家庭烧伤急救知识匮乏,120急救人员关于烧伤创面应急处理相对不充分,应优化老年烧伤具体应急防治策略,加大烧伤急救及慢性病防治宣教力度,强化社会支持,以降低老年烧伤发病率、病死率,减少经济损失。 Abstract:Objective To provide a practical basis for the field of elderly burn injury prevention and treatment by retrospectively analyzing the clinical data of elderly burn patients. Methods We retrospectively analyse the medical records of elderly burn patients who met the inclusion criteria admitted to the Second Affiliated Hospital of Kunming Medical University (hereafter referred to as the author’s unit) from January 2014 to December 2020, including gender, age, chronic disease, place of residence, place of injury, prehospital emergency trauma treatment, route of medical treatment, cause of injury, season of onset, burn site, burn area, and depth of burn. The data were analyzed by cardinality fit to optimize the data. The data were subjected to chi-square goodness-of-fit test, c2 test, linear association, Fisher’s exact probability test, rank sum test, one-way and multi-way Cox regression analysis, and multiple linear regression analysis. Results (1) A total of 471 patients met the inclusion criteria, there was an overall increasing trend of the proportion of elderly patients to inpatients in the same period with the increase of years (P < 0.01). The male to female ratio was 1.75∶1 (300/171), significantly more males than females (P < 0.001); the age distribution of patients was 69 (64, 77) years. In total, 247 patients (52.44%) had combined chronic diseases, and the common chronic diseases were hypertension 141 times (33.41%), diabetes mellitus 71 times (16.82%), old cerebral infarction 51 times (12.09%) in that order. (2) There were significantly more patients living in rural areas than in urban areas, and significantly more burns at home than in public places (all P < 0.05). There were 381 (80.89%) patients with untreated wounds in the prehospital emergency; only 34 were treated by 120; the common causes of injury were flame burns 274 (58.17%), hot liquid burns 155 (32.91%) in that order. The most frequent seasons were winter (168 cases, 35.67%) and spring (130 cases, 27.60%). The common burn sites were lower extremity 350 cases (74.31%) and upper extremity 230 cases (48.83%) in that order. The total burn area ≤10% TBSA was 272 cases (57.75%), of which 170 cases (36.09% of the total) were combined with third-degree burns. The severity of burns, in descending order, was moderate in 234 cases (49.68%), mild in 102 cases (21.66%), severe in 80 cases (16.99%), and extra-severe in 55 cases (11.68%). (3) In this group, 288 patients (61.15%) were finally cured and improved, 164 (34.82%) were automatically discharged, and 19 (4.03%) died. The age, total burn area, third-degree burn area, inhalation injury, post-injury complications, and combined chronic diseases were independent risk factors for the death in elderly patients (all P < 0.05). The duration of hospitalization was 11 (5, 22) d, and the hospitalization cost was 14320.62 (6347.92, 39638.06) yuan, which was influenced by the duration of hospitalization, total burn area, third-degree burn area, treatment modality, and complications after taking its logarithm because of the skewed distribution of hospitalization cost. Conclusions Elderly burns often occur in rural homes in winter and spring, with a male predominance, and flame burns and hydrothermal burns are the main causes. Patients are mostly young elderly people, and small-area deep burns are common, mainly concentrated in the lower and upper limbs, with high treatment costs. Most families lack knowledge of first aid for burns, and 120 emergency personnel are relatively inadequate regarding emergency treatment of burn trauma. Specific emergency prevention and treatment strategies for elderly burns should be optimized, education on first aid for burns and prevention of chronic diseases should be increased, and social support should be strengthened to reduce the incidence and morbidity of elderly burns and reduce economic losses. -
Key words:
- Elderly people /
- Burns /
- Hospitalized patients /
- Epidemiology
-

图 1 7 a间老年烧伤患者占同期住院患者比例趋势
*P < 0.05。
Figure 1. Trend of the proportion of elderly patients to hospitalized patients in the same period during the seven-year period

图 2 359例次老年烧伤患者合并慢性病构成分布
Figure 2. Distribution and composition of chronic diseases suffered by 359 cases of elderly patients with burns

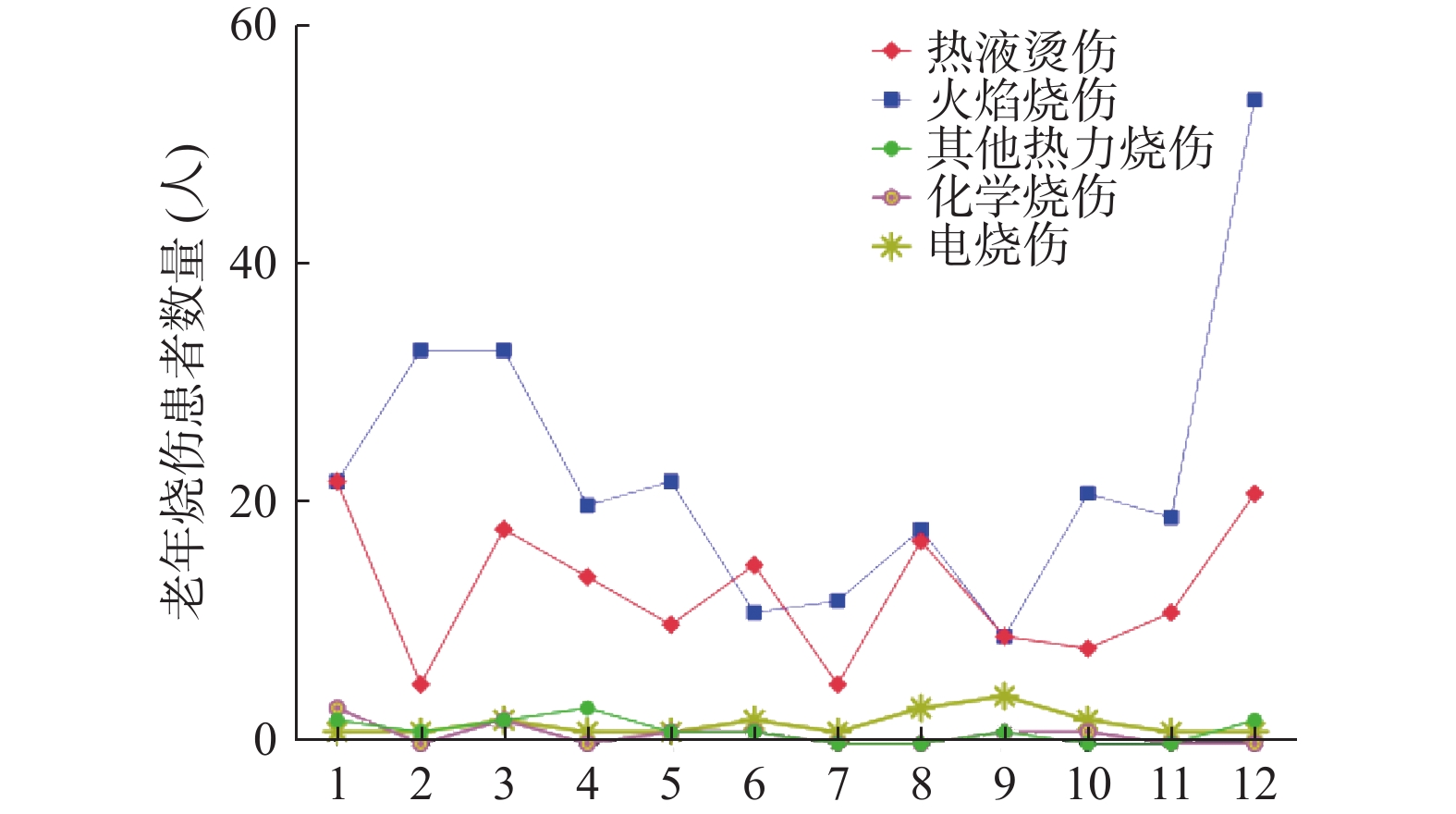
图 3 1~12月份老年烧伤患者分布情况
Figure 3. Distribution of elderly patients with burns form January to December

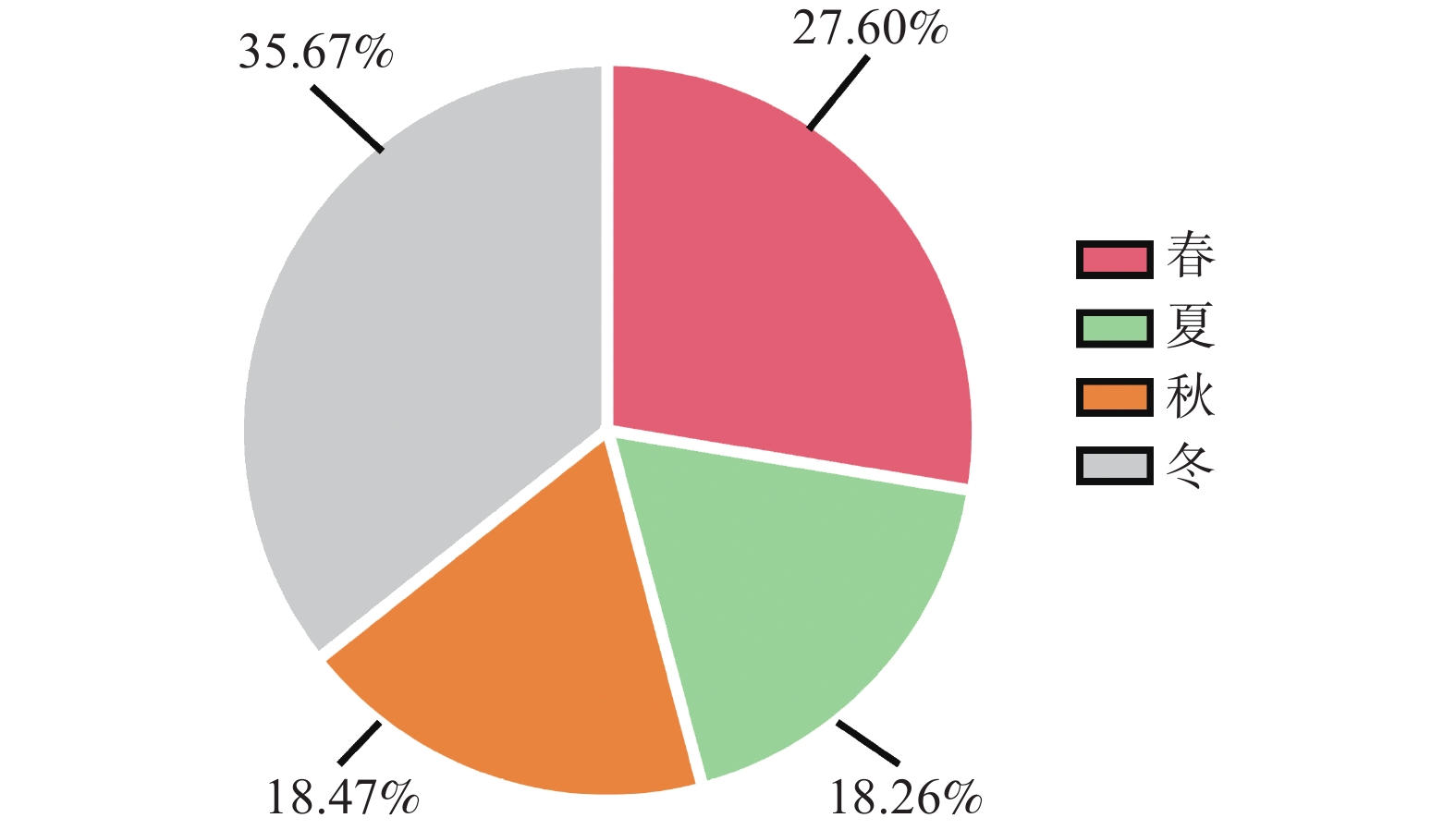
图 4 471例老年烧伤患者的季节分布
Figure 4. Seasonal distribution of 471 elderly patients with burns

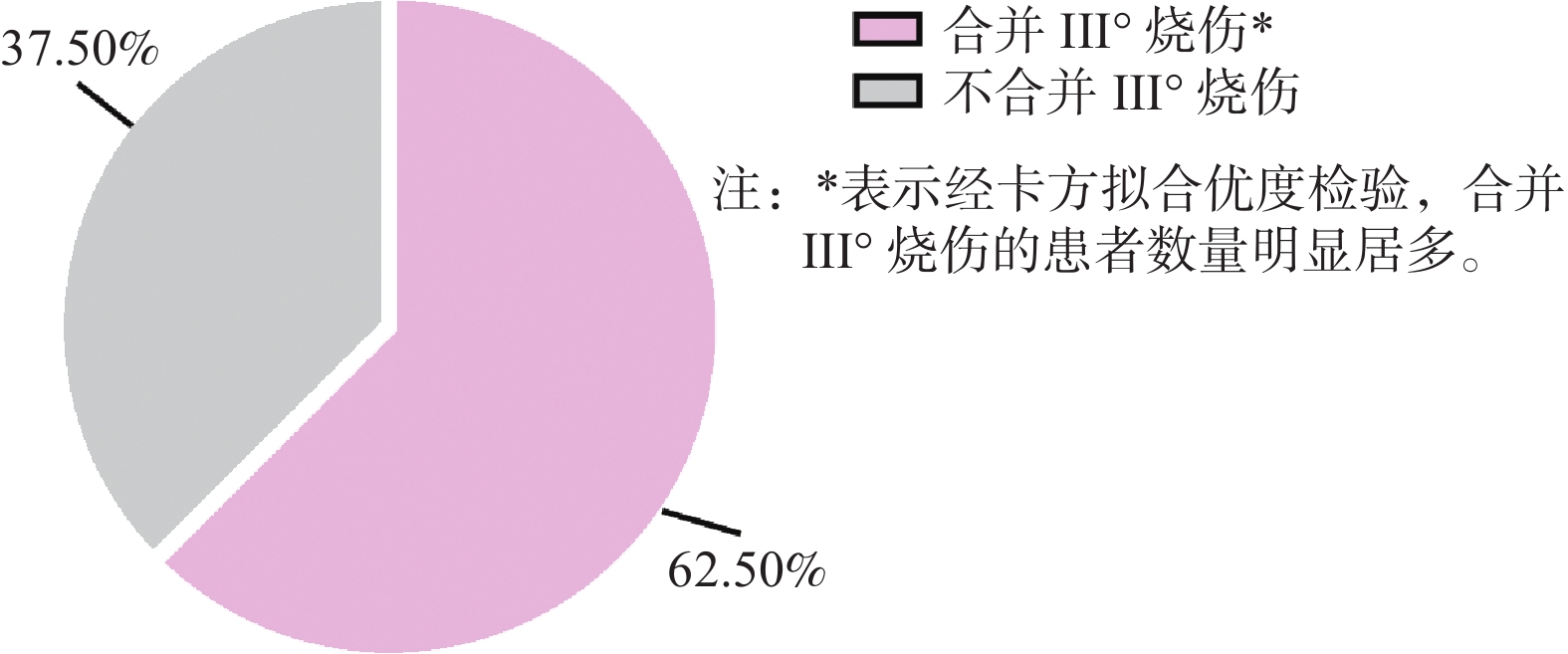
图 5 烧伤总面积≤10%TBSA的患者分布情况(total = 272)
Figure 5. distribution of patients with total burn area ≤10% TBSA (total = 272)

图 6 7 a间老年患者创面感染率趋势变化
*P < 0.05。
Figure 6. Trend of trauma infection rate in elderly patients over 7years
表 1 471例老年烧伤患者的性别和年龄段分布
Table 1. Gender and age distribution of 471 elderly burn patients
基本特征与分类 人数(n) 百分比(%) 性别 男 300 63.69 女 171 36.36 年龄段 年轻老人 325 69.00 老老人 136 28.88 长寿老人 10 2.12  下载: 导出CSV
下载: 导出CSV
表 2 农村和城市的致伤地点构成比、创面处理方式构成比[n(%)]
Table 2. Composition ratio of injury-causing locations and composition ratio of trauma management methods in rural and urban areas [n(%)]
居住地点 总计 受伤场所 院前创面处理不当处理 冷水冲 家中 公共场所 未处理 土办法 涂药膏 农村 295 284(96.27) 11(3.73) 247(83.73) 22(7.46) 4(1.36) 22(7.46) 城市 176 167(94.89) 9(5.11) 134(76.14) 14(7.95) 7(3.98) 21(11.93) χ2 0.520 6.482 P 0.471 0.090
下载: 导出CSV
表 3 7 a间471例老年烧伤住院患者致伤原因分布[n(%)]
Table 3. Distribution of causes of injury in 471 elderly patients hospitalized with burns during 7 years [n(%)]
致伤因素 2014年 2015年 2016年 2017年 2018年 2019年 2020年 热力烧伤 火焰烧伤 31(11.31) 22(8.03) 40(14.59) 37(14.60) 51(18.61) 44(16.06) 49(17.88) 热液烫伤 12(7.74) 8(5.16) 26(16.77) 26(16.77) 35(22.58) 25(16.12) 23(14.84) 其他热力 0 0 2(15.38) 2(15.38) 2(15.38) 6(46.15) 1(7.69) 电烧伤 2(10.00) 3(15.00) 3(15.00) 2(10.00) 4(20.00) 6(30.00) 0 化学烧伤 1(11.11) 0 1(11.11) 1(11.11) 1(11.11) 5(55.56) 0 合计 46(9.77) 33(7.01) 72(15.29) 68(14.44) 93(19.75) 86(18.26) 73(15.50) Fisher 25.760 P 0.243 注:其它热力烧伤包括热压伤、炽热金属烫伤、艾灸烫伤,电火花烧伤。
下载: 导出CSV
表 4 471例不同致伤原因住院患者性别分布[n(%)]
Table 4. Gender distribution of 471 patients hospitalized for different causative causes of injury [n(%)]
致伤原因 n 男 女 χ2 P 热力烧伤 火焰烧伤 274 180(65.69) 94(34.31) 10.732 0.03 热液烫伤 155 87(56.13) 68(43.87) 其他热力 13 8(61.54) 5(38.46) 电烧伤 20 17(85.00) 3(15.00) 化学烧伤 9 8(88.89) 1(11.11) 合计 471 300(63.69) 171(36.31)
下载: 导出CSV
表 5 471例老年烧伤患者烧伤面积和烧伤深度的分布情况[n(%)]
Table 5. Distribution of burn area and burn depth in 471 elderly patients with burns [n(%)]
烧伤总面积 n 三度烧伤累计 否 是 ≤10%TBSA 272 102(37.50) 170(62.50) 10%<X≤30% 124 56(45.16) 68(54.84) 30%<X≤50% 44 16(36.36) 28(63.64) >50% 31 6(19.35) 25(80.65)
下载: 导出CSV
表 6 ≤10%TBSA的272例患者不同就医途径的院前处理方式构成比比较[n(%)]
Table 6. Comparison of the composition ratio of prehospital management in 272 patients with ≤10% TBSA with different access routes [n(%)]
就医途径 总计 冷水冲洗 不当处理 未处理 土办法 涂药膏 120急救 8 0 8 0 0 自行前往医院 264 21 205 27 11 Fisher 0.632 P 0.851
下载: 导出CSV
表 7 老年烧伤中生存患者与病死患者一般情况比较[n(%)]
Table 7. Comparison of general conditions of surviving patients and patients who died of disease in elderly burns [n(%)]
患者类型 结局 χ2 Z P 生存 死亡 性别 男 254(62.56) 46(70.77) 1.632 0.201 女 152(37.44) 19(29.23) 冷水冲 冷水 34(8.37) 9(13.85) 2.022 0.155 其他 372(91.63) 56(86.15) 烧伤原因 热力烧伤 381(93.84) 61(93.85)
0.779
0.677电烧伤 18(4.43) 2(3.08) 化学烧伤 7(1.72) 2(3.08) 手术与否 是 139(34.24) 15(23.08) 3.171 0.075 否 267(65.76) 50(76.92) 慢性病 是 204(50.25) 43(66.15) 5.685 0.017* 否 202(49.75) 22(33.85) 并发症 是 78(19.21) 36(55.38) 39.962 < 0.001* 否 328(80.79) 29(44.62) 吸入性损伤 是 23(5.67) 19(29.23) 38.31 < 0.001* 否 383(94.33) 46(70.77) 年龄(岁,M) 68(63,76) 73(66,80) −3.131 0.002* 烧伤总面积(%TBSA,M) 8(3,15) 34(15,52.5) −8.499 < 0.001* Ⅲ度烧伤面积(%TBSA,M) 1(0,5) 20(7,36) −8.66 < 0.001* *P < 0.05。
下载: 导出CSV
表 8 影响老年严重烧伤患者病死的多因素Cox回归分析
Table 8. Multifactorial Cox regression analysis affecting morbidity and mortality in elderly patients with severe burns
变量 病死患者 P值 HR 95%CI 年龄 1.108 1.072~1.144 < 0.001* 烧伤总面积 1.026 1.009~1.044 0.003* Ⅲ度烧伤面积 1.022 1.005~1.04 0.013* 基础疾病 1.745 1.021~2.98 0.042* 并发症 1.835 1.036~3.25 0.037* 吸入性损伤 1.875 1.014~3.467 0.045* *P < 0.05。
下载: 导出CSV
表 9 老年烧伤住院患者费用多元线性回归分析
Table 9. Multiple linear regression analysis of costs for elderly burn inpatients
变量 偏回归系数 偏回归系数标准误 标准回归系数 t P 住院天数 0.015 0.001 0.481 13.998 < 0.001 烧伤总面积 0.012 0.001 0.395 9.494 < 0.001 Ⅲ度烧伤面积 −0.007 0.002 −0.184 −4.493 < 0.001 有无手术 −0.383 0.041 −0.329 −9.384 < 0.001 有无并发症 −0.079 0.037 −0.062 −2.157 0.032
下载: 导出CSV
-
[1] 熊飞,鲁彦良,张慧. 云南省社会化养老发展问题研究[J]. 经济研究导刊,2021,(16):47-49. doi: 10.3969/j.issn.1673-291X.2021.16.015 [2] 吴文瑶,张谨,郑华. 世界医学协会《赫尔辛基宣言》: 涉及人类受试者的医学研究伦理原则[J]. 中华疼痛学杂志,2020,(2):92-93. doi: 10.3760/cma.j.cn101658-20191025-1910-149 [3] 殷磊. 老年护理学[J]. 护士进修杂志,2001,16(10):726-727. doi: 10.3969/j.issn.1002-6975.2001.10.002 [4] 黎鳌杨宗城. 烧伤学[M]. 上海: 科学技术出版社, 2001. [5] 江丽姣,于倩倩,尹文强,等. 我国居民慢性病变化趋势分析——基于国家五次卫生服务调查报告[J]. 中国卫生事业管理,2018,35(11):874-876. [6] 刘萌,张勤,刘健,等. 2005年至2016年上海交通大学医学院附属瑞金医院老年严重烧伤特点分析[J]. 中华损伤与修复杂志(电子版),2018,13(3):195-202. doi: 10.3877/cma.j.issn.1673-9450.2018.03.008 [7] 陈习琼. 基于六次人口普查数据的云南省人口老龄化分析[J]. 中国老年学杂志,2018,38(12):3054-3057. doi: 10.3969/j.issn.1005-9202.2018.12.090 [8] 耳玉亮,段蕾蕾,叶鹏鹏,等. 2014年全国伤害监测系统老年人非故意伤害病例特征分析[J]. 中国健康教育,2016,32(4):312-317. doi: 10.16168/j.cnki.issn.1002-9982.2016.04.005 [9] 龚慧云,张庆军,张岚,等. 2008-2015年湖北省老年人伤害死亡流行现状及趋势[J]. 公共卫生与预防医学,2017,28(4):77-80. [10] 徐薇,吕渊,庞国防,等. 影响老年人健康的主要疾病[J]. 中国老年保健医学,2021,19(4):13-15. doi: 10.3969/j.issn.1672-2671.2021.04.004 [11] 赵瑾,叶怡,庄园,等. 老年烧伤患者心理状况多维度调查及影响因素分析[J]. 国际老年医学杂志,2022,43(1):31-35. doi: 10.3969/j.issn.1674-7593.2022.01.008 [12] 吴直惠,黄建琼,周敏,等. 老年烧伤原因的调查与分析[J]. West China Medical Journal,2010,25(7):1235-1237. [13] 尚新志,唐乾利,张力,等. 280例老年烧伤住院患者流行病学调查[J]. 中华烧伤杂志,2008,(2):128. [14] 张建明王玉莲邓诗琳高志刚魏琴. 1960例老年人烧伤流行病学调查[J]. 解放军预防医学杂志,2001,(4):258-260. doi: 10.3969/j.issn.1001-5248.2001.04.008 [15] Liu Y,Chen J,Crook N,et al. Epidemiologic investigation of burns in the elderly in Sichuan Province[J]. Burns,2013,39(3):389-394. doi: 10.1016/j.burns.2012.04.012 [16] 付倩倩,张苗苗,杨晓宇,等. 甘肃省某地区老年烧伤患者流行病学调查及分析[J]. 感染、炎症、修复,2021,22(4):195-198. doi: 10.3969/j.issn.1672-8521.2021.04.001 [17] 苏青青. 中国高原和日本平原老年人身体素质的比较研究[J]. 山东体育科技,2018,40(6):89-94. doi: 10.14105/j.cnki.1009-9840.2018.06.017 [18] Ji S Z,Luo P F,Kong Z D,et al. Pre-hospital emergency burn management in Shanghai: analysis of 1868 burn patients[J]. Burns,2012,38(8):1174-1180. doi: 10.1016/j.burns.2012.03.010 [19] Klein M B,Hayden D,Elson C,et al. The association between fluid administration and outcome following major burn: a multicenter study[J]. Ann Surg,2007,245(4):622-628. doi: 10.1097/01.sla.0000252572.50684.49 [20] 曹胜军,王凌峰,巴特,等. 严重烧伤事故批量患者的救治[J]. 中华卫生应急电子杂志,2017,3(3):143-146. doi: 10.3877/cma.j.issn.2095-9133.2017.03.004 [21] 杨宗城. 加强对烧伤休克综合防治的研究[J]. 中华烧伤杂志,2006,(5):331-332. [22] 张元海,田鹏飞,张惟,等. 急救网络建设在危重氢氟酸烧伤患者早期救治中的作用[J]. 中华烧伤杂志,2021,37(10):921-928. [23] Savetamal A. Infection in Elderly Burn Patients: What Do We Know?[J]. Surg Infect (Larchmt),2021,22(1):65-68. doi: 10.1089/sur.2020.322 [24] 王国军. 烧伤患者住院期间生存质量评估[J]. 中国医药导报,2015,12(10):94-97. [25] 胡利娟,王霞,王艳霞,等. 烧伤患者心理应激反应与社会支持相关性研究[J]. 中国护理管理,2012,12(2):35-38. doi: 10.3969/j.issn.1672-1756.2012.02.011 [26] 黄艳. 老年烧伤病人的护理体会[J]. 航空航天医学杂志,2012,23(4):458-459. doi: 10.3969/j.issn.2095-1434.2012.04.044 [27] Yin Z,Qin Z,Xin W,et al. The characteristics of elderly burns in Shanghai[J]. Burns,2010,36(3):430-435. doi: 10.1016/j.burns.2009.06.204 [28] 张中原. 老年烧伤原因与治疗探讨[J]. 医药论坛杂志,2008,29(21):107-108. [29] 杨义,郝岱峰,褚万立,等. 2017年度北京市某三甲医院创面修复专科住院病例回顾分析[J]. 中华损伤与修复杂志(电子版),2019,14(5):344-349. doi: 10.3877/cma.j.issn.1673-9450.2019.05.005 [30] Reddy M. Skin and wound care: important considerations in the older adult[J]. Adv Skin Wound Care,2008,21(9):424-436,437-438. doi: 10.1097/01.ASW.0000323547.12358.b8 [31] Thombs B D,Singh V A,Halonen J,et al. The effects of preexisting medical comorbidities on mortality and length of hospital stay in acute burn injury: evidence from a national sample of 31,338 adult patients[J]. Ann Surg,2007,245(4):629-634. doi: 10.1097/01.sla.0000250422.36168.67 [32] 曹志,程杨杨,王媛,等. 高发慢性病对老年人全因死亡影响的前瞻性研究[J]. 中国慢性病预防与控制,2020,28(1):20-23. doi: 10.16386/j.cjpccd.issn.1004-6194.2020.01.005 [33] Youngmin K, Dohern K, Jun H, et al. Does inhalation injury predict mortality in burns patients or require redefinition?[J]. PLoS ONE, 2017, 12(9): 185195. [34] 张慧君,赵筱卓,王成,等. 223例成人严重烧伤住院患者的流行病学调查[J]. 中国医刊,2022,57(2):184-190. doi: 10.3969/j.issn.1008-1070.2022.02.019 [35] 雷高峰. 院前急救对烧伤患者的近期预后影响[J]. 航空航天医学杂志,2019,30(8):934-935. doi: 10.3969/j.issn.2095-1434.2019.08.017 [36] 崔亚,杨轶男,赵美韬,等. 2017年甘肃省0~6岁儿童伤害住院患者直接经济负担分析[J]. 伤害医学(电子版),2019,8(2):12-16. [37] 张勤, 张寅, 廖镇江. 老年烧伤预防和治疗的现状和问题: 中华医学会烧伤外科学分会2009年学术年会[C], 中国江西南昌, 2009. [38] 唐钧,冯凌. 长期照护的全球共识和概念框架[J]. 社会政策研究,2021,1:18-38. doi: 10.19506/j.cnki.cn10-1428/d.2021.01.003 -



 点击查看大图
点击查看大图

计量
- 文章访问数: 4367
- HTML全文浏览量: 2103
- PDF下载量: 21
- 被引次数: 0
