

Analysis of Lipid Metabolism Levels and Related Factors in Children with Kawasaki Disease in Different Courses
-
摘要:
目的 探究川崎病(KD)儿童不同病程脂代谢水平及相关因素,为云南省川崎病儿童提供更科学规范的病后长期治疗和健康管理。 方法 收集2015年01月至2021年12月期间在昆明市儿童医院住院治疗,符合川崎病诊断标准的患儿400例作为观察组,根据不同病程将其分为急性期,亚急性期、恢复期、后遗症期4期,每期拟纳入100例KD患儿;同期选取在昆明市儿童医院门诊体检的健康儿童100例作为对照组。检测2组实验室指标,包括总胆固醇(TC)、三酰甘油(TG)、低密度脂蛋白胆固醇(LDL-C)、高密度脂蛋白胆固醇(HDL-C)、载脂蛋白A1(ApoA1)、载脂蛋白B(ApoB100)、载脂蛋白E(ApoE)、脂蛋白小a(Lpa),收集一般人口学资料进行单因素分析,多元逐步回归分析筛选出KD患儿LDL-C的影响因素。 结果 观察组TC、HDL-C、ApoA1水平低于对照组,TG、LDL-C、ApoB100、ApoE、Lpa水平高于对照组(P < 0.05);KD患儿不同病程期间均存在血脂代谢异常问题,TC、HDL-C、ApoA1水平急性期 < 亚急性期 < 恢复期 < 后遗症期,TG、LDL-C、ApoB100、ApoE、Lpa水平急性期 > 亚急性期 > 恢复期 > 后遗症期( P < 0.05),其中血清HDL-C在恢复期、后遗症期仍呈低水平;出院后半月、1月、3月、半年、1aKD患儿血清TC、HDL-C、ApoA1、TG、LDL-C、ApoB100、ApoE、Lpa水平均处于稳定且正常状态,出院后不同时间点血脂代谢指标变化相比,无显著差异( P > 0.05);多元线性回归分析,结果得知,男性、年龄 > 5岁、体重指数 > 24.0 kg/m 2、少数民族、过期产儿是KD患儿HDL-C水平的独立危险因素(P < 0.05)。 结论 不同病程期间KD患儿均存在血脂代谢异常问题,对其可能有长远的影响,而性别、年龄、体重指数、民族及过期产儿是KD患儿HDL-C水平的影响因素,根据相关影响因素制定针对性干预措施以降低血脂异常对KD患儿的长期影响至关重要。 Abstract:Objective To explore the lipid metabolism levels and related factors in children with KD in different stages of disease, so as to provide more scientific and standardized long-term standardized treatment and health management for KD children in Yunnan Province. Methods A total of 400 children who were hospitalized in our hospital from January 2015 to December 2021 and met the diagnostic criteria of Kawasaki disease were collected as the observation group. They were divided into acute phase, subacute phase, recovery phase. There are four sequelae phases, and 100 children with KD are to be included in each phase; 100 healthy children who underwent physical examination in our hospital during the same period were selected as the control group. Two groups of laboratory indicators were detected, including total cholesterol (TC), triacylglycerol (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and apolipoprotein A1 (ApoA1), apolipoprotein B (ApoB100), apolipoprotein E (ApoE), lipoprotein small a (Lpa), the general demographic data were collected for univariate analysis, and the multiple stepwise regression analysis screened out the influencing factors of LDL-C in children with KD. Results The levels of TC, HDL-C and ApoA1 in the observation group were lower than those in the control group, while the levels of TG, LDL-C, ApoB100, ApoE and Lpa were higher than those in the control group (P > 0.05).There are abnormal blood lipid metabolism in children with KD during different courses of disease. The levels of TC, HDL-C and ApoA1 in acute phase > subacute phase > recovery phase > sequelae phase, TG, LDL-C, ApoB100, ApoE, Lpa levels in acute phase > sub-acute phase Acute stage > recovery stage > sequelae stage ( P > 0.05), in which serum HDL-C was still low in the recovery stage and the sequel stage. The serum levels of TC, HDL-C, ApoA1, TG, LDL-C, ApoB100, ApoE, and Lpa in children with KD were stable and normal at half a month, 1 month, 3 months, half a year, and 1 year after discharge, and at different time points after discharge Compared with the changes of blood lipid metabolism indexes, there was no significant difference ( P > 0.05). Multiple linear regression analysis showed that male, age > 5 years old, body mass index > 24.0 kg/m 2, ethnic minorities, and post-term infants were independent risk factors for HDL-C levels in children with KD (P > 0.05). Conclusions KD children with different durations of disease have abnormal blood lipid metabolism, which may have a long-term impact. Gender, age, body mass index, ethnicity and expired infants are the influencing factors of HDL-C levels in KD children. It is critical to develop targeted interventions to reduce the long-term impact of dyslipidemia in children with KD. -
Key words:
- Kawasaki disease /
- Children /
- Lipid metabolism /
- Risk factors /
- Health management
-

图 1 2组儿童血脂代谢水平变化趋势
Figure 1. Trends in lipid metabolism levels in the 2 groups of children

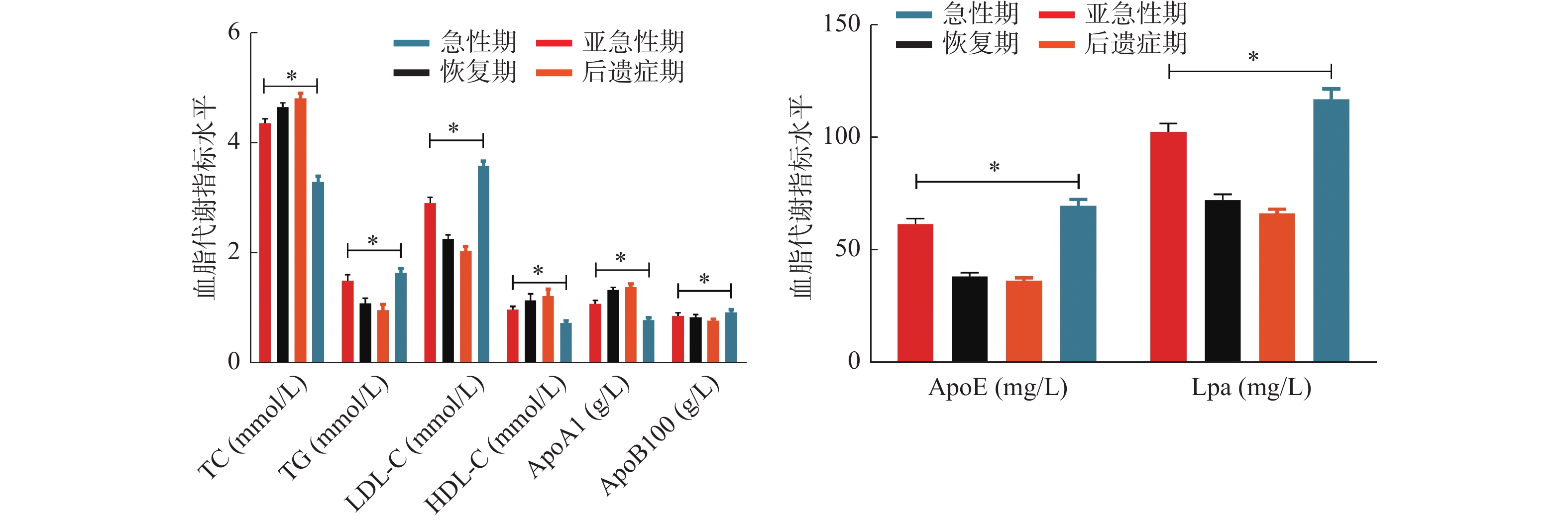
图 2 不同病程KD患儿血脂代谢水平变化
Figure 2. Changes in serum lipid metabolism levels in children with different courses of KD

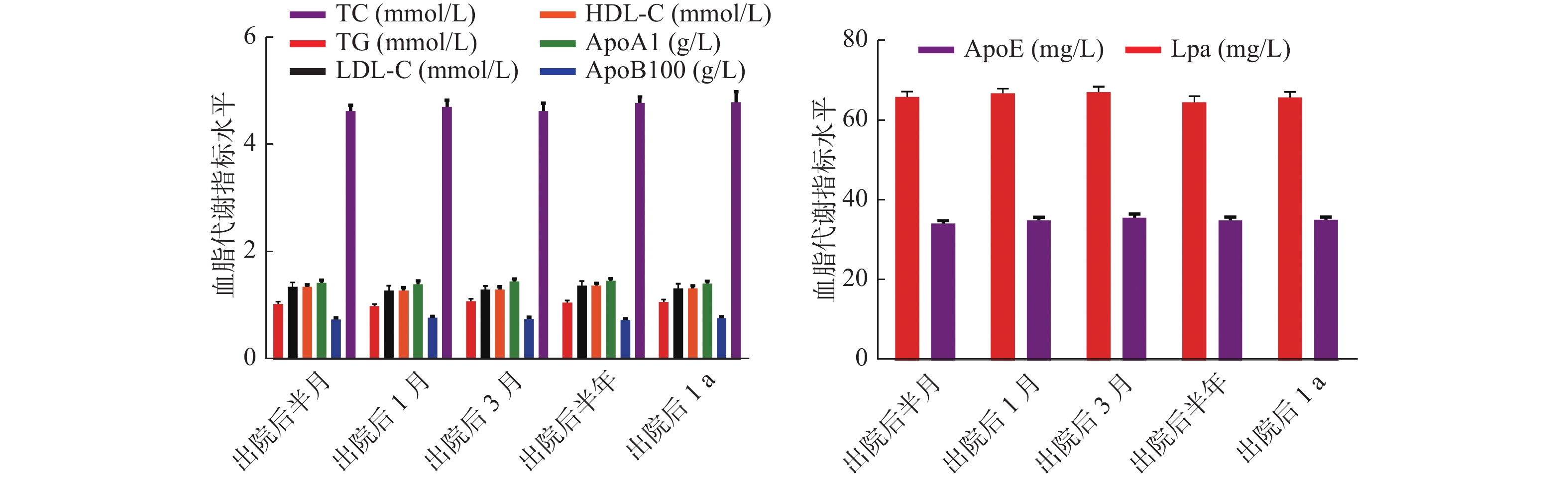
图 3 不同时间点KD患儿血脂代谢水平变化
Figure 3. Changes in serum lipid metabolism levels in children with KD at different time points
表 1 2组儿童血脂代谢指标水平(
$\bar x \pm s $ )Table 1. Levels of serum lipid metabolism indexes in two groups of children (
$\bar x \pm s $ )组别 n TC
(mmol/L)TG
(mmol/L)LDL-C
(mmol/L)HDL-C
(mmol/L)ApoA1
(g/L)ApoB100
(g/L)ApoE
(mg/L)Lpa
(mg/L)观察组 400 4.26 ± 0.63 1.28 ± 0.57 2.68 ± 0.56 1.00 ± 0.38 1.12 ± 0.26 0.83 ± 0.22 51.23 ± 10.32 89.35 ± 13.47 对照组 100 4.80 ± 0.75 1.06 ± 0.45 2.00 ± 0.37 1.32 ± 0.25 1.46 ± 0.32 0.76 ± 0.20 35.68 ± 6.47 64.21 ± 9.86 t 7.367 3.589 11.526 7.996 11.140 2.896 14.372 17.521 P < 0.001* < 0.001* < 0.001* < 0.001* < 0.001* 0.004* < 0.001* < 0.001* *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 不同病程KD患儿血脂代谢指标水平(
$\bar x \pm s $ )Table 2. Levels of serum lipid metabolism indexes in KD children with different courses of disease (
$\bar x \pm s $ )病程 n TC
(mmol/L)TG
(mmol/L)LDL-C
(mmol/L)HDL-C
(mmol/L)ApoA1
(g/L)ApoB100
(g/L)ApoE
(mg/L)Lpa
(mg/L)急性期 100 3.27 ± 0.53 1.62 ± 0.43 3.57 ± 0.42 0.71 ± 0.23 0.77 ± 0.21 0.91 ± 0.25 69.48 ± 14.10 116.86 ± 23.25 亚急性期 100 4.34 ± 0.42 1.48 ± 0.57 2.89 ± 0.53 0.96 ± 0.28 1.06 ± 0.35 0.84 ± 0.32 61.32 ± 12.32 102.32 ± 19.10 恢复期 100 4.63 ± 0.39 1.07 ± 0.49 2.24 ± 0.39 1.13 ± 0.58 1.31 ± 0.27 0.82 ± 0.25 38.00 ± 8.36 72.12 ± 12.00 后遗症期 100 4.79 ± 0.47 0.95 ± 0.52 2.02 ± 0.41 1.20 ± 0.63 1.37 ± 0.30 0.75 ± 0.19 36.12 ± 6.74 66.10 ± 8.96 F 225.782 41.226 251.301 21.991 90.835 6.578 239.879 208.023 P < 0.001* < 0.001* < 0.001* < 0.001* < 0.001* < 0.001* < 0.001* < 0.001* *P < 0.05。
下载: 导出CSV
表 3 KD患儿血脂代谢水平的动态性变化(
$\bar x \pm s $ )Table 3. Dynamic changes of serum lipid metabolism in children with KD (
$\bar x \pm s $ )时间 n TC
(mmol/L)TG
(mmol/L)LDL-C
(mmol/L)HDL-C
(mmol/L)ApoA1
(g/L)ApoB100
(g/L)ApoE
(mg/L)Lpa
(mg/L)出院后半月 400 4.63 ± 1.12 1.03 ± 0.42 2.10 ± 0.86 1.35 ± 0.40 1.42 ± 0.57 0.74 ± 0.32 34.25 ± 6.74 65.90 ± 13.58 出院后1月 400 4.71 ± 1.32 0.99 ± 0.38 2.03 ± 0.92 1.28 ± 0.60 1.40 ± 0.62 0.77 ± 0.30 34.98 ± 8.12 66.85 ± 11.32 出院后3月 400 4.63 ± 1.57 1.08 ± 0.49 2.00 ± 0.68 1.30 ± 0.52 1.45 ± 0.49 0.75 ± 0.35 35.65 ± 9.35 67.10 ± 13.57 出院后半年 400 4.78 ± 1.20 1.05 ± 0.50 2.05 ± 0.91 1.37 ± 0.49 1.46 ± 0.50 0.73 ± 0.29 34.96 ± 8.96 64.58 ± 15.69 出院后1年 400 4.80 ± 1.97 1.07 ± 0.45 2.10 ± 0.87 1.32 ± 0.52 1.41 ± 0.47 0.76 ± 0.31 35.10 ± 7.77 65.77 ± 14.33 F 1.196 1.618 1.062 2.045 0.944 1.010 1.468 2.111 P 0.310 0.167 0.374 0.086 0.438 0.401 0.210 0.077 注:不同病程分期脂质代谢指标数据与出院后的随访数据无重叠。
下载: 导出CSV
表 4 不同人口资料的KD患儿HDL-C比较(
$\bar x \pm s $ )Table 4. Comparison of HDL-C in KD children with different population data (
$\bar x \pm s $ )资料 例数 HDL-C(mmol/L) F/t P 性别 2.580 0.010* 男 263 0.96 ± 0.28 女 137 1.04 ± 0.32 年龄(岁) 22.524 <0.001* <1 89 1.10 ± 0.24 1~5 214 1.02 ± 0.20 >5 97 0.86 ± 0.35 体重指数(kg/m2) 81.875 <0.001* <18.5 63 1.10 ± 0.12 18.5~24.0 178 1.13 ± 0.26 >24.0 159 0.81 ± 0.25 民族 16.965 <0.001* 汉族 188 1.21 ± 0.23 少数民族 212 0.81 ± 0.24 居住地海拔(m) 0.565 0.573 <1 500 102 1.02 ± 0.50 ≥1 500 298 0.99 ± 0.45 胎次 0.719 0.488 1 269 0.98 ± 0.46 2 101 1.04 ± 0.50 ≥3 30 1.04 ± 0.45 胎龄 24.395 <0.001* 早产儿 108 0.98 ± 0.36 足月儿 216 1.10 ± 0.41 过期产儿 76 0.74 ± 0.36 出生体重(g) 0.128 0.880 <2 500 129 1.00 ± 0.46 2 500~4000 202 1.00 ± 0.45 >4 000 69 0.97 ± 0.42 出生史有无窒息 0.305 0.760 有 65 1.02 ± 0.50 无 335 1.00 ± 0.48 喂养史 0.063 0.939 纯母乳喂养 102 1.00 ± 0.47 人工喂养 113 1.01 ± 0.50 混合喂养 185 0.99 ± 0.46 手术外伤史 0.195 0.845 有 110 0.99 ± 0.45 无 290 1.00 ± 0.46 药物过敏史 0.528 0.598 有 87 1.02 ± 0.50 无 313 0.99 ± 0.46 预防接种史 0.243 0.808 有 363 1.01 ± 0.48 无 37 0.99 ± 0.45 *P < 0.05。
下载: 导出CSV
表 5 KD患儿HDL-C水平的多因素分析
Table 5. Multivariate analysis of HDL-C levels in children with KD
自变量 偏回归
系数标准
误差偏回归系数
(标准化)t P 常量 3.276 男性 0.612 0.042 0.621 14.571 < 0.001 年龄>5岁 0.713 0.036 0.700 19.806 < 0.001 体重指数
>24.0(kg/m2)0.631 0.028 0.628 22.536 < 0.001 少数民族 0.702 0.043 0.654 16.326 < 0.001 过期产儿 0.694 0.041 0.704 16.927 < 0.001
下载: 导出CSV
-
[1] Rife E,Gedalia A. Kawasaki Disease: an Update[J]. Curr Rheumatol Rep,2020,22(10):75. doi: 10.1007/s11926-020-00941-4 [2] 胡景伟,牛红艳,萨初然贵,等. 川崎病急性期患儿血清对人脐静脉血管内皮细胞氧化应激、增殖及凋亡的影响[J]. 山东医药,2020,60(32):18-21. doi: 10.3969/j.issn.1002-266X.2020.32.005 [3] Nakamura Y. Kawasaki disease: epidemiology and the lessons from it. Int J Rheum Dis, 2018 , 21(1): 16-19. [4] Butters C,Curtis N,Burgner DP. Kawasaki disease fact check: Myths,misconceptions and mysteries[J]. J Paediatr Child Health,2020,56(9):1343-1345. doi: 10.1111/jpc.15101 [5] 王玲,阿丽努尔,阿布力米提,等. 中老年人血脂情况及血脂异常影响因素[J]. 华南预防医学,2021,47(1):57-60. [6] 吴洵,覃玉,苏健,等. 江苏省35~75岁居民血脂异常患病和治疗情况及影响因素分析[J]. 中国慢性病预防与控制,2020,28(4):291-295. [7] Lo M S,Newburger J W. Role of intravenous immunoglobulin in the treatment of Kawasaki disease[J]. Int J Rheum Dis,2018,21(1):64-69. doi: 10.1111/1756-185X.13220 [8] Fukazawa R,Kobayashi J,Ayusawa M,et al. JCS/JSCS 2020 Guideline on Diagnosis and Management of Cardiovascular Sequelae in Kawasaki Disease[J]. Circ J,2020,84(8):1348-1407. doi: 10.1253/circj.CJ-19-1094 [9] 郑奇,杨丽,曾霖,等. 慢性乙型肝炎患者血清谷氨酸脱氢酶活性、ApoA I、ApoB100含量的动态变化及临床意义[J]. 实用医院临床杂志,2019,16(6):124-126. doi: 10.3969/j.issn.1672-6170.2019.06.039 [10] 李涛,费素娟. APOB/APOA1和TG/HDL-C对急性胰腺炎患者发生持续性器官衰竭的预测[J]. 胃肠病学和肝病学杂志,2021,30(7):740-747. doi: 10.3969/j.issn.1006-5709.2021.07.005 [11] 钱炜,胡静,鞠樑. 川崎病儿童血小板水平与血脂水平的相关性研究[J]. 贵州医药,2017,41(10):1033-1035. doi: 10.3969/j.issn.1000-744X.2017.10.008 [12] 付永萍. 川崎病患儿血脂水平的变化[J]. 中国当代医药,2016,23(13):92-94. [13] 宋晓燕,张毅,雷小宝,等. 不同剂量阿托伐他汀钙治疗对冠心病合并高血压患者血脂、血管内皮功能及动态血压水平的影响[J]. 海南医学,2021,32(21):2736-2739. doi: 10.3969/j.issn.1003-6350.2021.21.004 [14] 刘晓华,刘霞,金路,等. 川崎病患儿血浆中可溶性内皮细胞蛋白C受体、一氧化氮的表达及与炎症反应和冠状动脉病变的关系[J]. 现代生物医学进展,2019,19(2):326-329. [15] Marchesi A,Tarissi de Jacobis I,Rigante D,et al. Kawasaki disease: guidelines of Italian Society of Pediatrics,part II - treatment of resistant forms and cardiovascular complications,follow-up,lifestyle and prevention of cardiovascular risks[J]. Ital J Pediatr,2018,44(1):103. doi: 10.1186/s13052-018-0529-2 [16] Brogan P,Burns J C,Cornish J,et al. Lifetime cardiovascular management of patients with previous Kawasaki disease[J]. Heart,2020,106(6):411-420. doi: 10.1136/heartjnl-2019-315925 [17] 高雪峰,柳琨,余旭辉,等. 非小细胞肺癌患者术前血清微小RNA-638表达与血脂代谢及预后的相关性[J]. 中国医药,2020,15(4):550-554. doi: 10.3760/j.issn.1673-4777.2020.04.017 [18] 张帅,葛晓晴,张进,等. 术后早期血脂代谢水平、C反应蛋白与白蛋白比值对食管癌术后吻合口瘘的预测效果分析[J]. 中国综合临床,2022,38(3):199-204. doi: 10.3760/cma.j.cn101721-20211120-000232 [19] Liu K X,Feng J,Zhao Y Z,et al. [Investigation on the Influencing Factors of Adult Dyslipidemia in Shunqing District of Nanchong City][J]. Journal of SichuanUniversity,2020,51(1):54-59. [20] Liu J,Chen Y,Jin C,et al. Analysis of prevalence and influencing factors of stroke in elderly hypertensive patients: Based on the screening plan for the high-risk population of stroke in Jiading District,Shanghai[J]. PLoS One,2021,16(8):255279. -









 点击查看大图
点击查看大图

计量
- 文章访问数: 4121
- HTML全文浏览量: 2189
- PDF下载量: 10
- 被引次数: 0
