

Diagnostic Value of MSCT Combined With MRI in T Staging of Gastric Cancer
-
摘要:
目的 探索MSCT(multislice spiral CT,MSCT)联合MRI(magnetic resonance imaging,MRI)成像对胃癌术前T分期的诊断价值。 方法 收集57例经手术病理证实为胃癌患者的术前影像资料,所有患者术前2周内均行MSCT及MRI检查,分别采用3种方式进行T分期,即(1)MSCT,CT轴位联合多平面重组(multi-planner reformation,MPR);(2)MRI;(3)MSCT联合MRI。以上术前T分期结果与术后病理结果进行对照,计算胃癌病灶T分期诊断的准确率、敏感度、特异度、阳性预测值及阴性预测值,分析比较3种方式T分期诊断准确率之间的差异,采用Kappa值检验3种方式术前T分期诊断结果与病理结果一致性。 结果 MSCT、MRI、MSCT联合MRI术前T分期与病理结果一致性分析Kappa值分别为0.583(一致性中等),0.646(一致性较强),0.848(一致性强)。总体准确率分别为70.18%、75.44%、89.47%,分析比较发现MSCT与MRI、MSCT与MSCT联合MRI术前T分期诊断准确率比较差异有统计学意义(P < 0.05),MRI与MSCT联合MRI术前T分期诊断准确率比较差异无统计学意义(P > 0.05)。 结论 MRI术前T分期准确率高于MSCT,将二者联合使用可有效提高胃癌术前T分期诊断准确率,从而有利于胃癌患者术前评估以及治疗方案的选择。 Abstract:Objective To explore the diagnostic value of multispiral computed tomograpay (MSCT) combined with magnetic resonance imaging (MRI) in preoperative T staging of gastric cancer. Methods The preoperative imaging data of 57 patients with gastric cancer confirmed by surgery and pathology were collected. All patients were examined by MSCT and MRI within two weeks before surgery. Three methods were used for T staging: (1) MSCT, CT axial position and multiplanar reformation (MPR); (2)MRI; (3) MSCT combined with MRI. The above preoperative T staging results were compared with the postoperative pathological results to calculate the accuracy, sensitivity, specificity, positive predictive value and negative predictive value of the T staging diagnosis of gastric cancer lesions, analyze and compare the differences between the three methods of T staging diagnosis accuracy, and use Kappa value to test the consistency of the three methods of preoperative T staging diagnosis and pathological results. Results The Kappa values of preoperative T staging and pathological results of MSCT, MRI and MSCT combined MRI were 0.583 (moderate consistency), 0.646 (strong consistency) and 0.848 (strong consistency), respectively. The overall accuracy rates were 70.18%, 75.44% and 89.47%, respectively. Analysis and comparison showed that there were statistically significant differences in the accuracy rates of preoperative T staging diagnosis between MSCT and MRI, MSCT and MSCT combined MRI (P < 0.05). There was no statistically significant difference in the accuracy rates of preoperative T staging diagnosis between MRI and MSCT combined MRI (P > 0.05). Conclusions The accuracy of preoperative T staging with MRI is higher than that with MSCT. The combined use of MRI and MSCT can effectively improve the accuracy of preoperative T staging diagnosis, which is conducive to the preoperative evaluation of gastric cancer patients and the selection of treatment plans. -
Key words:
- Gastric cancer /
- Neoplasm staging /
- Magnetic resonance imaging /
- Tomography /
- X-ray computer
-

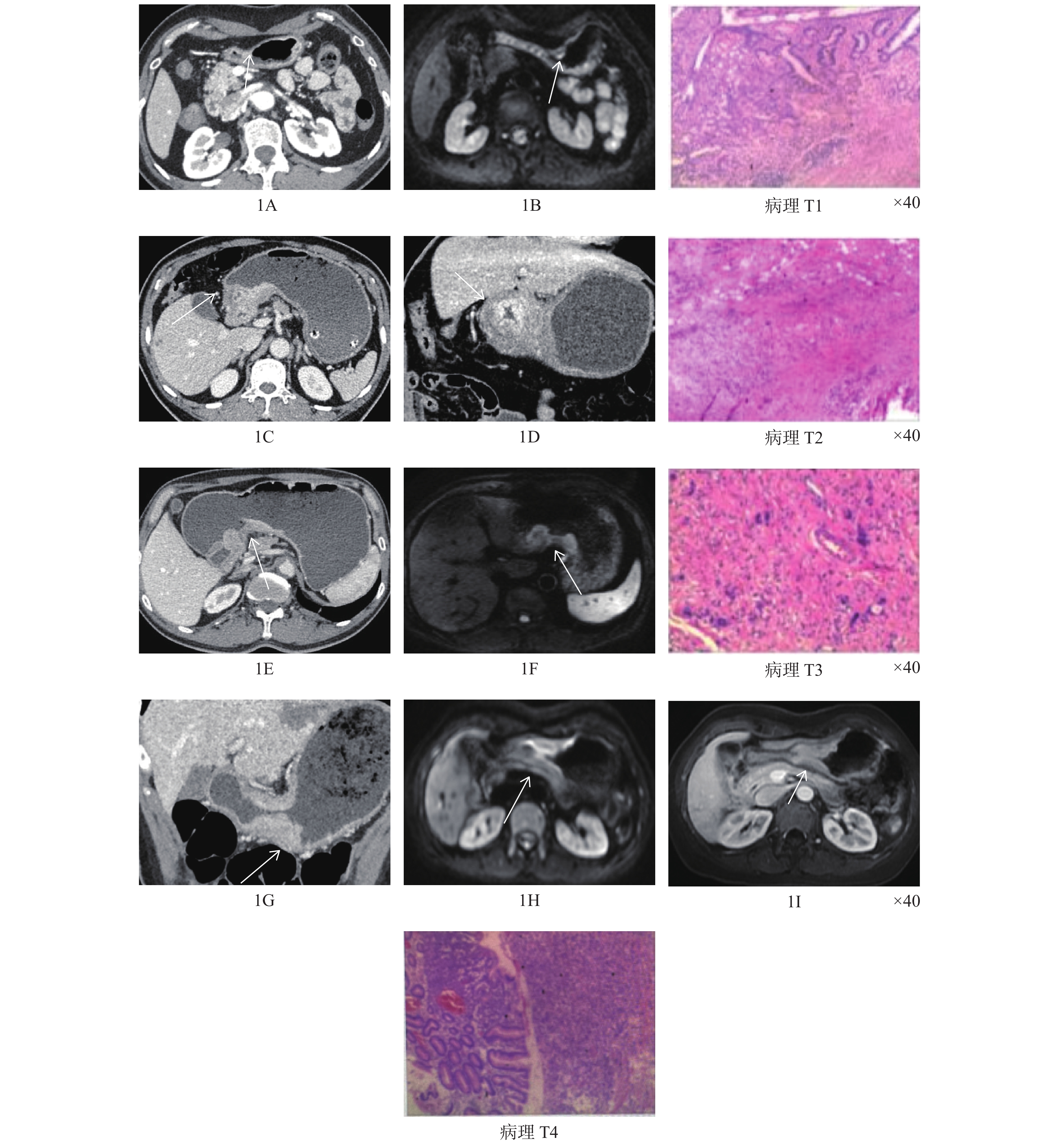
图 1 MSCT及MRI成像对胃癌T1~T4期各分期的诊断结果
Figure 1. Results of MSCT and MRI in the diagnosis of T1-T4 stages of gastric cancer
表 1 MSCT胃癌术前T分期与病理结果对照(n)
Table 1. Comparison between preoperative T staging and pathological results of MSCT gastric cancer (n)
MSCT
分期病理分期
总计T1 T2 T3 T4 T1 8 1 0 0 9 T2 1 3 5 1 10 T3 2 1 11 5 19 T4 0 0 1 18 19 总计 11 5 17 24 57  下载: 导出CSV
下载: 导出CSV
表 2 MRI胃癌术前T分期与病理结果对照(n)
Table 2. Comparison of preoperative T staging and pathological results of gastric cancer on MRI (n)
MRI
分期病理分期
总计T1 T2 T3 T4 T1 6 1 0 0 7 T2 5 2 1 1 9 T3 0 2 13 1 16 T4 0 0 3 22 25 总计 11 5 17 24 57
下载: 导出CSV
表 3 MSCT联合MRI胃癌术前T分期与病理结果对照(n)
Table 3. Comparison of preoperative T staging and pathological results of gastric cancer by MSCT combined with MRI (n)
MSCT联合MRI分期 病理分期
总计T1 T2 T3 T4 T1 9 1 0 0 10 T2 2 4 1 1 7 T3 0 0 15 1 16 T4 0 0 1 23 24 总计 11 5 17 24 57
下载: 导出CSV
表 4 MSCT诊断T分期与MRI诊断T分期交叉表(n)
Table 4. Cross table of MSCT diagnosis T staging and MRI diagnosis T staging (n)
MSCT
分期MRI分期
总计
P值
Kappa值T1 T2 T3 T4 T1 4 5 0 0 9 0.010* 0.410 T2 0 3 4 3 10 T3 3 0 10 6 19 T4 0 1 2 16 19 总计 7 9 16 25 57 *P < 0.05。
下载: 导出CSV
表 5 MSCT诊断T分期与MSCT联合MRI诊断T分期交叉表(n)
Table 5. Cross table of MSCT diagnosis T staging and MSCT combined MRI diagnosis T staging (n)
MSCT
分期MSCT联合MRI分期 总计 P值 Kappa
值T1 T2 T3 T4 T1 7 2 0 0 9 0.046* 0.584 T2 0 5 3 2 10 T3 3 0 11 5 19 T4 0 0 2 17 19 总计 10 7 16 24 57 *P < 0.05。
下载: 导出CSV
表 6 MRI诊断T分期与MSCT联合MRI诊断T分期交叉表(n)
Table 6. Cross table of MRI diagnosis T staging and MSCT combined MRI diagnosis T staging (n)
MRI
分期MSCT联合MRI分期
总计
P值
Kappa值T1 T2 T3 T4 T1 7 0 0 0 7 0.092 0.798 T2 3 5 0 1 9 T3 0 2 14 0 16 T4 0 0 2 23 25 总计 10 7 16 24 57
下载: 导出CSV
表 7 MSCT诊断胃癌T分期的评价指标(%)
Table 7. Evaluation indexes of T staging of gastric cancer diagnosed by MSCT (%)
病理分期 敏感度 特异度 阳性预测值 阴性预测值 准确率 T1 72.73 97.83 88.89 93.75 92.98 T2 60.00 86.54 30.00 95.74 84.21 T3 64.71 80.00 57.89 84.21 75.44 T4 75.00 96.97 94.74 84.21 87.72
下载: 导出CSV
表 8 MRI诊断胃癌T分期的评价指标(%)
Table 8. Evaluation index of T stage of gastric cancer diagnosed by MRI (%)
病理分期 敏感度 特异度 阳性预测值 阴性预测值 准确率 T1 54.55 97.83 85.71 90.00 89.47 T2 40.00 84.54 22.22 93.75 82.46 T3 76.47 92.50 81.25 90.24 87.72 T4 91.67 90.91 88.00 93.75 91.23
下载: 导出CSV
表 9 MSCT联合MRI诊断胃癌T分期的评价指标(%)
Table 9. Evaluation indexes of MSCT combined with MRI in diagnosing T stage of gastric cancer (%)
病理分期 敏感度 特异度 阳性预测值 阴性预测值 准确率 T1 81.82 97.83 90.0 95.74 94.74 T2 80.00 94.23 57.14 98.00 92.98 T3 88.24 97.5 93.75 93.75 94.74 T4 95.83 96.97 95.83 96.97 96.49
下载: 导出CSV
-
[1] 段纪俊,严亚琼,杨念念,等. 中国恶性肿瘤发病与死亡的国际比较分析[J]. 中国医学前沿杂志(电子版),2016,8(7):17-23. [2] Ono H,Yao K,Fujshro M,et al. Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer[J]. Digestive Endoscopy,2016,28(1):3-15. doi: 10.1111/den.12518 [3] 何文琪,伍兵. 胃癌术前cTN分期的影像研究进展[J]. 国际医学放射学杂志,2019,42(1):76-80. [4] 付英杰,顾程,李欣,等. 多层螺旋CT扫描多平面重组技术在胃癌术前T、N分期中的应用[J]. 山东医药,2020,60(15):92-94. doi: 10.3969/j.issn.1002-266X.2020.15.025 [5] 梁建晓. 高场磁共振弥散加权成像在可切除胃癌术前评价和预后评估中的应用研究[D]. 济南: 山东大学, 2018. [6] Yan Y T,Liang Y P,You B T,et al. Value of 3.0T MRI Routine Sequence Combined with DWI in Diagnosis of Preoperative T and N Staging in Patients with Gastric Cancer[J]. Medical & Pharmaceutical Journal of Chinese People’s Liberation Army,2018,30(9):28-30. [7] 国家卫生健康委员会. 胃癌诊疗规范(2018年版)[J]. 中华消化病与影像杂志(电子版),2019,9(3):118-144. doi: 10.3877/cma.j.issn.2095-2015.2019.03.008 [8] 耿晓丹,于丽娟,陈慕楠,等. MRI平扫结合DWI在胃癌术前T分期及淋巴结转移上的价值[J]. 中国癌症杂志,2016,26(7):629-634. [9] SungH,Ferlay J,Siegel R L,et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries[J]. CA:a cancer journal for Clinicians,2021,71(3):209-249. doi: 10.3322/caac.21660 [10] 中华人民共和国国家卫生健康委员会医政医管局. 胃癌诊疗指南(2022年版)[J]. 中华消化外科杂志,2022,21(9):1137-1164. doi: 10.3760/cma.j.cn115610-20220726-00432 [11] 左婷婷,郑荣寿,曾红梅,等. 中国流行病学现状[J]. 中国肿瘤临床,2017,44(1):52-58. doi: 10.3969/j.issn.1000-8179.2017.01.881 [12] Isobe Y,Nashimoto A,Akazawa K,et al. Gastric cancer treatment in Japan: 2008 annual report of the JGCA nationwide registry[J]. Gastric Cancer,2011,14(4):301-316. doi: 10.1007/s10120-011-0085-6 [13] Ajani J A,Bentrem D J,Besh S,et al. Gastric cancer,version 2.2013: featured updates to the NCCN Guidelines[J]. J Natl Compr Canc Netw,2013,11(5):531-546. doi: 10.6004/jnccn.2013.0070 [14] 张义,颜小航. MRI与CT对胃癌术前分期诊断的作用研究[J]. 影像研究与医学应用,2019,3(16):49-50. [15] 秦书敏,刘亚良,黄光建,等. 3.0T MRI与MSCT对胃癌术前T分期的诊断价值[J]. 解放军医药杂志,2018,30(12):19-22. doi: 10.3969/j.issn.2095-140X.2018.12.005 [16] 朱海涛,赵宜良,吴云飞,等. 不同浆膜反应类型胃癌淋巴结转移特点及其对实施合理根治术的指导意义[J]. 中华肿瘤杂志,2009,31(6):474-477. doi: 10.3760/cma.j.Issn.0253-3766.2009.06.019 [17] 王嵩,任克,孙文阁,等. MRI与MSCT对胃癌术前T分期的比较[J]. 放射学实践,2011,26(4):426-429. doi: 10.3969/j.issn.1000-0313.2011.04.021 [18] 唐磊. 胃癌术前影像学精准分期存在的争议与困惑[J]. 中华胃肠外科杂志,2016,19(2):165-169. doi: 10.3760/cma.j.issn.1671-0274.2016.02.009 [19] 刘松,何健,管文贤,等. MRI弥散加权成像在进展期胃癌T分期中的应用[J]. 实用放射学杂志,2013,29(4):565-568. doi: 10.3969/j.issn.1002-1671.2013.04.015 [20] 张良云. VIBE RADIAL序列在提高上腹部图像质量上的应用研究[D]. 秦皇岛: 燕山大学, 2017. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 4116
- HTML全文浏览量: 2308
- PDF下载量: 7
- 被引次数: 0
