

Relationship between Bile Duct Uneven Dilation and Postoperative Pancreatitis after ERCP
-
摘要:
目的 探讨胆管不均匀扩张与ERCP术后胰腺炎的关系。 方法 选择昆明医科大学第二附属医院2018年1月到2021年12月共247例因胆总管结石行内镜逆行胰胆管造影(endoscopic retrograde cholangiopancreatography ,ERCP) + 内镜下乳头括约肌切开术(endoscopic sphincterotomy,EST)+内镜下鼻胆管引流术(endoscopic nasobiliary drainage,ENBD)的患者,分扩张组(胆管直径≥10 mm)(A组 = 84)与无扩张组(胆管直径 < 10 mm)(B组 = 163,对照组)进行统计学处理并比较。 结果 A组84例,其中女性45例;可疑的Oddi括约肌功能障碍(sphincter of oddi dysfunction ,SOD)患者9例;困难插管者30例,其中插到胰管者22例,胰管显影者8例;胆胰管汇合异常(anomalous pancreaticobiliary ductal junction ,APBDJ)者9例。A组患者中ERCP术后发生轻度胰腺炎10例,中度胰腺炎8例,重度胰腺炎3例。B组163例,其中女性72例;可疑的SOD患者11例;困难插管者63例,其中插到胰管者61例,胰管显影者2例;APBDJ患者1例。B组患者中ERCP术后发生轻度胰腺炎10例,中度胰腺炎1例,重度胰腺炎者4例。A组行吲哚美辛肛栓患者数为30例,B组为57例。A组ERCP术后胰腺炎(post-ERCP pancreatitis,PEP)发生率为25%,B组PEP发生率为9.20%,两者比较差异具有统计学意义(P = 0.001);将247例患者整体进行Logistic单因素回归分析显示,胆管扩张(OR = 3.289,95%CI = 1.593~6.792,P = 0.001)是PEP的独立危险因素。 结论 女性患者且伴有胆管不均匀扩张患者(胆管直径≥10 mm)比无扩张患者(胆管直径 < 10 mm)在ERCP术后更容易患PEP。因此,在对这部分患者行ERCP+EST+ENBD手术时需谨慎处理,尽量避免行内镜下复杂的手术操作。 Abstract:Objective To investigate the relationship between bile duct uneven dilatation and postoperative pancreatitis after ERCP. Methods A total of 247 cases of ERCP+EST + ENBD due to bile duct stone were performed in the Second Affiliated Hospital of Kunming Medical University from January 2018 to December 2021. They were divided into the bile duct dilation group (bile duct diameter ≥10 mm) (group A = 84) and the nondilated group (bile duct diameter < 10 mm) (group B = 163) as control group for statistical processing and comparison. Results There were 84 patients in group A, including 45 females; 9 cases of suspected SOD; there are 30 patients with difficult cannulation, including 22 patients with pancreatic guidewire passages and 8 patients with development of the pancreatic duct; 9 cases of APBDJ.In group A, there were 10 cases of mild pancreatitis, 8 cases of moderate pancreatitis, and 3 cases of severe pancreatitis. There were 163 patients in group B, including 72 females; 11 cases of suspected SOD; there were 63 patients with difficult cannulation, including 61 pancreatic guidewire passages and 2 patients with development of the pancreatic duct; 1 case of APBDJ. In group B, there are 10 cases of mild pancreatitis, 1 case of moderate pancreastitis, and 4 cases of severe pancreatitis. There were 30 patients in group A and 57 patients in group B who received indomethacin anal embolus. The incidence of PEP was 25% in group A and 9.2% in group B, and the difference between the two groups was statistically significant (P = 0.001). Logistic univariate regression analysis of 247 patients showed that bile duct dilatation (OR = 3.289, 95%CI = 1.593~6.792, P = 0.001) was an independent risk factor for PEP. Conclusions Female patient with uneven bile duct dilation (bile duct diameter ≥10 mm) is more likely to develop PEP than nondilated patient (bile duct diameter < 10 mm). Therefore, ERCP + EST + ENBD should be carefully handled in these patients, and complex endoscopic surgical operations should be avoided as far as possible. -

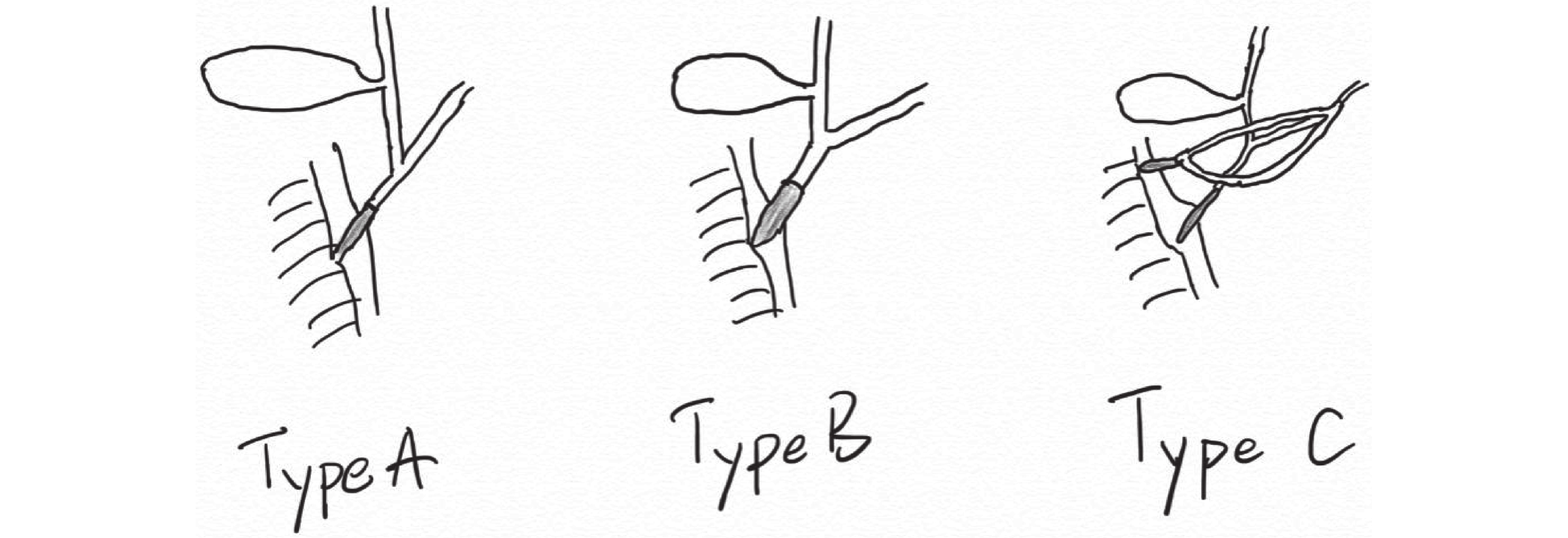
图 2 胆胰管汇合异常的3种方式
Figure 2. Three types of anomalous pancreaticobiliary ductal junction
表 1 A、B2组患者术前相关危险因素统计分析情况[n(%)]
Table 1. Preoperative statistical analysis of related risk factors in group A and group B [n(%)]
相关危险因素 A组发生率(n = 84) B组发生率(n = 163) χ2 P 插到胰管 22(26.19) 61(37.42) 3.135 0.077 胰管显影 8(9.52) 2(1.23) − 0.005* 可疑的SOD 9(10.71) 11(6.75) 1.173 0.279 女性 45(53.57) 72(44.17) 1.965 0.161 APBDJ 9(10.71) 1(0.61) − 0.001* 吲哚美辛肛栓 30(35.71) 57(34.97) 0.013 0.908 *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 A、B2组术后胰腺炎统计情况及数据分析[n(%)]
Table 2. Statistical situation and data analysis of postoperative pancreatitis in group A and B [n(%)]
项目 扩张组(n = 84) 无扩张组(n = 163) χ2/t P PEP例数及发生率 21(25.00) 15(9.20) 11.111 0.001* 重症胰腺炎患者平均住院时间(d) 312 66 20.860 < 0.001* *P < 0.05。
下载: 导出CSV
表 3 ERCP术后胰腺炎相关因素的Logistic单因素分析结果
Table 3. Logistic univariate analysis of factors associated with pancreatitis after ERCP surgery
相关因素 B 标准误 Wald OR 95%CI P 胰管显影 3.396 0.816 17.334 29.857 6.035~147.721 < 0.001* 插到胰管 0.130 0.377 0.119 1.139 0.544~2.381 0.730 可疑的SOD 0.746 0.551 1.828 2.108 0.715~6.210 0.176 胆管扩张 1.191 0.370 10.352 3.289 1.593~6.792 0.001* 女性 1.232 0.397 9.622 3.429 1.574~7.468 0.002* APBDJ 4.248 1.074 15.656 70 8.534~574.201 < 0.001* *P < 0.05。
下载: 导出CSV
表 4 ERCP术后胰腺炎相关因素的Logistic多因素分析结果
Table 4. Logistic multivariate analysis of pancreatitis related factors after ERCP surgery
相关因素 总数(n) PEP数(n) B 标准误 Wald OR 95%CI P 胰管显影 84 13 2.183 1.156 3.563 8.871 0.920~85.573 0.059 插到胰管 10 8 0.232 0.455 0.261 1.262 0.518~3.076 0.609 可疑的SOD 20 5 1.084 0.651 2.776 2.957 0.826~10.584 0.096 胆管扩张 84 21 0.662 0.428 2.389 1.939 0.837~4.489 0.122 女性 117 26 1.372 0.472 8.435 3.944 1.562~9.954 0.004* APBDJ 10 9 3.208 1.291 6.173 24.724 1.969~310.520 0.013* *P < 0.05。
下载: 导出CSV
-
[1] 李鹏,王拥军,王文海. 中国经内镜逆行胰胆管造影术指南(2018版)[J]. 临床肝胆病杂志,2018,34(12):2537-2554. doi: 10.3969/j.issn.1001-5256.2018.12.009 [2] Kawai K,Akasaka Y,Murakami K,et al. Endoscopic sphincterotomy of the ampulla of Vater[J]. Gastrointest Endosc,1974,20(4):148-151. doi: 10.1016/S0016-5107(74)73914-1 [3] Andriulli A,Loperfido S,Napolitano G,et al. Incidence rates of post-ERCP complications: a systematic survey of prospective studies[J]. Am J Gastroenterol,2007,102(8):1781-1788. doi: 10.1111/j.1572-0241.2007.01279.x [4] Wang A Y,Strand D S,Shami V M. Prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: Medications and techniques[J]. Clin Gastroenterol Hepatol,2016,14(11):1521-1532,1523. [5] 中国医师协会介入医师分会. 经皮经肝十二指肠乳头肌扩张顺行排石术治疗胆总管结石诊治规范[J]. 中华内科杂志,2022,61(3):263-268. doi: 10.3760/cma.j.cn112138-20210823-00578 [6] Itoi T,Kamisawa T,Fujii H,et al. Extrahepatic bile duct measurement by using transabdominal ultrasound in Japanese adults: multi-center prospective study[J]. J Gastroenterol,2013,48(9):1045-1050. doi: 10.1007/s00535-012-0702-0 [7] Cotton P B,Lehman G,Vennes J,et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus[J]. Gastrointest Endosc,1991,37(3):383-393. doi: 10.1016/S0016-5107(91)70740-2 [8] Banks P A,Bollen T L,Dervenis C,et al. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus[J]. Gut,2013,62(1):102-111. doi: 10.1136/gutjnl-2012-302779 [9] Dumonceau J M,Kapral C,Aabakken L,et al. ERCP-related adverse events:European society of gastrointestinal endoscopy (ESGE) Guideline[J]. Endoscopy,2020,52(2):127-149. doi: 10.1055/a-1075-4080 [10] Baiu I,Visser B. Endoscopic retrograde cholangiopancreatography[J]. Jama,2018,320(19):2050. doi: 10.1001/jama.2018.14481 [11] Talukdar R. Complications of ERCP[J]. Best Pract Res Clin Gastroenterol,2016,30(5):793-805. doi: 10.1016/j.bpg.2016.10.007 [12] Ding X,Zhang F,Wang Y. Risk factors for post-ERCP pancreatitis: A systematic review and meta-analysis[J]. Surgeon,2015,13(4):218-229. doi: 10.1016/j.surge.2014.11.005 [13] Chen J J,Wang X M,Liu X Q,et al. Risk factors for post-ERCP pancreatitis:A systematic review of clinical trials with a large sample size in the past 10 years[J]. Eur J Med Res,2014,19(1):26. doi: 10.1186/2047-783X-19-26 [14] El Nakeeb A,El Hanafy E,Salah T,et al. Post-endoscopic retrograde cholangiopancreatography pancreatitis: Risk factors and predictors of severity[J]. World J Gastrointest Endosc,2016,8(19):709-715. doi: 10.4253/wjge.v8.i19.709 [15] Ishibashi H,Shimada M,Kamisawa T,et al. Japanese clinical practice guidelines for congenital biliary dilatation[J]. J Hepatobiliary Pancreat Sci,2017,24(1):1-16. doi: 10.1002/jhbp.415 [16] Kamisawa T,Kaneko K,Itoi T,et al. Pancreaticobiliary maljunction and congenital biliary dilatation[J]. Lancet Gastroenterol Hepatol,2017,2(8):610-618. doi: 10.1016/S2468-1253(17)30002-X [17] Singham J,Yoshida E M,Scudamore C H. Choledochal cysts: part 1 of 3:Classification and pathogenesis[J]. Can J Surg,2009,52(5):434-440. [18] Vater A,Ezler C. Dissertatio de Scirrhis viscerum occasione sectionis viri tympanite defunte[J]. Wittenburgae,1723,881:22. [19] Hamada Y,Ando H,Kamisawa T,et al. Diagnostic criteria for congenital biliary dilatation 2015[J]. J Hepatobiliary Pancreat Sci,2016,23(6):342-346. doi: 10.1002/jhbp.346 [20] Drenth J P,Chrispijn M,Bergmann C. Congenital fibrocystic liver diseases[J]. Best Pract Res Clin Gastroenterol,2010,24(5):573-584. doi: 10.1016/j.bpg.2010.08.007 [21] Dabbas N,Davenport M. Congenital choledochal malformation: not just a problem for children[J]. Ann R Coll Surg Engl,2009,91(2):100-105. doi: 10.1308/003588409X391947 [22] Sato Y,Ren X S,Nakanuma Y. Caroli's disease: Current knowledge of its biliary pathogenesis obtained from an orthologous rat model[J]. Int J Hepatol,2012,2012:107945. [23] 董家鸿,郑秀海,夏红天,et al. 胆管囊状扩张症: 新的临床分型与治疗策略[J]. 中华消化外科杂志,2013,12(5):370-377. doi: 10.3760/cma.j.issn.1673-9752.2013.05.012 [24] Kim H J,Kim M H,Lee S K,et al. Normal structure,variations,and anomalies of the pancreaticobiliary ducts of Koreans: a nationwide cooperative prospective study[J]. Gastrointest Endosc,2002,55(7):889-896. doi: 10.1067/mge.2002.124635 [25] Yoshimoto K,Kamisawa T,Kikuyama M,et al. Classification of pancreaticobiliary maljunction and its clinical features in adults[J]. J Hepatobiliary Pancreat Sci,2019,26(12):541-547. doi: 10.1002/jhbp.691 [26] Zhang Z,Li Y,Li K,et al. Value of multidisciplinary team (MDT) in minimally invasive treatment of complex intrahepatic bile duct stones[J]. Biosci Trends,2021,15(3):161-170. doi: 10.5582/bst.2021.01169 [27] 郭志唐,魏东,李伟思,等. 全麻仰卧位下同步双镜联合在Ⅰ型Mirizzi综合征并胆总管结石手术中的应用价值[J]. 中华普通外科杂志,2020,9(35):681-684. [28] 郭志唐,王琳,魏东,等. 同步双镜联合在继发性胆总管结石治疗中的应用价值[J]. 重庆医学,2020,3(49):345-348. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 4106
- HTML全文浏览量: 2542
- PDF下载量: 16
- 被引次数: 0
