

Associations between SLC2A9 Single Nucleotide Polymorphisms and Susceptibility to Pyrazinamide Induced Hyperuricemia
-
摘要:
目的 探讨云南地区汉族人群SLC2A9基因单核苷酸多态性与吡嗪酰胺致高尿酸血症(pyrazinamide induced hyperuricemia,PIHU)的易感性关系。 方法 应用Mass ARRAY法对294例PIHU患者(试验组)和220例非PIHU患者(对照组)的SLC2A9基因单核苷酸多态性位点rs2280205、rs3733591、rs3775948、rs10939650基因型进行检测,比较基因型及等位基因频率分布,分析不同遗传模型下4个位点多态性与PIHU的易感性关系。 结果 2组间rs2280205位点基因型频率及等位基因频率分布比较,差异有统计学意义(P < 0.05),携带等位基因A的患者PIHU风险增高;rs2280205位点多态性在共显性、显性、隐性模型下与PIHU显著相关(均P < 0.05)。rs3733591位点基因型频率及等位基因频率在2组间分布比较,差异有统计学意义(P < 0.05),携带等位基因T的患者PIHU风险增高;rs3733591位点多态性在共显性、显性、隐性模型下与PIHU显著相关(均P < 0.05)。rs3775948位点基因型频率及等位基因频率在2组间分布比较,差异有统计学意义(均P < 0.001),携带等位基因C的患者PIHU风险增高;rs3775948位点多态性在共显性和显性模型下与PIHU显著相关(均P < 0.05)。rs10939650位点基因型频率及等位基因频率在2组间分布比较,差异有统计学意义(均P < 0.001),携带等位基因C的患者PIHU风险增高;rs10939650位点多态性在共显性和隐性模型下与PIHU显著相关(均P < 0.05)。 结论 SLC2A9基因rs2280205、rs3733591、rs3775948、rs10939650位点多态性可能与云南地区汉族人群PIHU的易感性相关,rs2280205位点等位基因A、rs3733591位点等位基因T、rs3775948位点等位基因C、rs10939650位点等位基因T可能是发生PIHU的风险因素。 Abstract:Objective To explore the association between gene single nucleotide polymorphisms of SLC2A9 and susceptibility to pyrazinamide induced hyperuricemia (PIHU) in Yunnan Han population. Methods The polymorphisms of SLC2A9 gene rs2280205, rs3733591, rs3775948 and rs10939650 were detected by Mass ARRAY method. Genotype and allele frequency distribution were compared between the test group (n = 294) and the control group (n = 220) and analyzing the association between the polymorphisms of SLC2A9 with susceptibility to PIHU in different genetic models. Results There were significant differences in genotype frequency and allele frequency distribution of rs2280205 between the two groups (P < 0.05). Patients carrying allele A had an increased risk of PIHU; rs2280205 polymorphism was significantly correlated with PIHU in co-dominant, dominant and recessive models (all P < 0.05). rs3733591 genotype frequency and allele frequency distribution between the two groups, the difference was statistically significant (P < 0.05), the patients with allele T increased the risk of PIHU. rs3733591 polymorphism was significantly correlated with PIHU in co-dominant, dominant and recessive models (all P < 0.05). rs3775948 genotype frequency and allele frequency distribution between the two groups, the difference was statistically significant (all P < 0.001), the patients with allele C of PIHU increased risk; rs3775948 polymorphism was significantly associated with PIHU in both co-dominant and dominant models (P < 0.05). rs10939650 genotype frequency and allele frequency distribution between the two groups, the difference was statistically significant (all P < 0.001), the patients with allele C of PIHU increased risk; rs10939650 polymorphism was significantly associated with PIHU in both co-dominant and recessive models (P < 0.05). Conclusion SLC2A9 gene polymorphisms rs2280205, rs3733591, rs3775948 and rs10939650 may be associated with the susceptibility to PIHU in Yunnan Han population, and allele A of rs2280205, allele T of rs3733591, allele C of rs3775948 and allele T of rs10939650 may be risk factors for PIHU. -
Key words:
- Pyrazinamide /
- Hyperuricemia /
- SLC2A9 gene /
- Single nucleotide polymorphisms
-

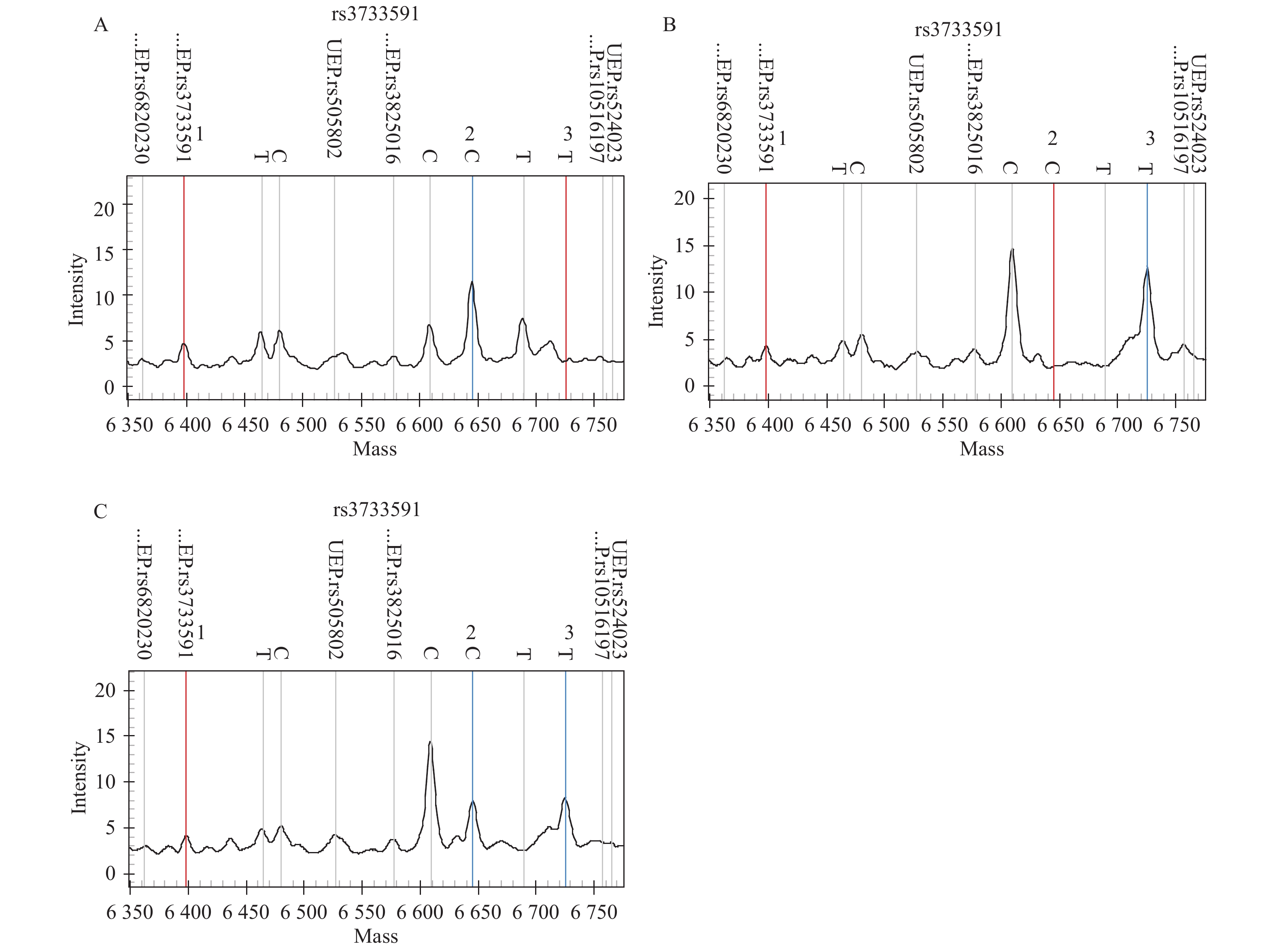
图 1 rs3733591位点基因分型图
A~C:rs3733591位点野生纯合型分型图、突变纯合型分型图、突变杂合型分型图;图中第1条标线为UEP相对分子质量,第2条标线为UEP+C碱基的相对分子量,第3条标线为UEP+T碱基的相对分子量。
Figure 1. Genotypes of rs3733591 loci
表 1 SLC2A9基因SNPs引物序列
Table 1. Primer sequences of SNPs with SLC2A9 gene
SNPs 引物序列 PCR扩增产物长度(bp) rs2280205 上游引物:5’ACGTTGGATGACTGACCATTCTCTCTGCTCC-3’ 135 下游引物:5’ACGTTGGATGTACTCAAGGTGACGTATGGG-3’ UEP引物:5’-gagggGACGTATGGGATCTTTGCC-3’ rs3733591 上游引物:5’-ACGTTGGATGTTTCCCAAGAGGTAGAGGAG-3’ 147 下游引物:5’-ACGTTGGATGATGGTGACAATCACGGTGAC-3’ UEP引物:5’-ctgaGGATGCTCCTCTGCACG-3’ rs3775948 上游引物:5’-ACGTTGGATGCTTCACAACAACCCTCTGAC-3’ 131 下游引物:5’-ACGTTGGATGAAGTCTGGGCTCCGATACAC-3’ UEP引物:5’-AGCTATGTGTTTCTTAAACTCTTT-3’ rs10939650 上游引物:5’-ACGTTGGATGTGACCTCCCAAGAACCTTTC-3’ 130 下游引物:5’-ACGTTGGATGACCCAGACACTCTGACTTTG-3’ UEP引物:5’-CGGTGGACTTGTGGGGAC-3’  下载: 导出CSV
下载: 导出CSV
表 2 PZA治疗4~5周后研究对象的基本情况[n(%)/
$ \bar x \pm s $ ]Table 2. The basic situation of the study subjects after 4~ 5 weeks of PZA treatment [n(%)/
$ \bar x \pm s $ ]指标 试验组(n = 294) 对照组(n = 220) χ2/t P 性别 0.065 0.573 男 155(52.7) 118(53.6) 女 139(47.3) 102(46.4) 年龄(岁) 46.80 ± 9.98 45.91 ± 10.76 0.042 0.837 血尿素氮(mmol/L) 3.92 ± 0.83 4.16 ± 0.91 −1.228 0.265 血肌酐(μmol/L) 62.52 ± 14.11 59.67 ± 15.43 −1.038 0.304 血尿酸(μmol/L) 648.32 ± 109.23 319.14 ± 52.64 −15.425 < 0.001* *P < 0.05。
下载: 导出CSV
表 3 SLC2A9基因SNPs位点基因型及等位基因频率分布比较[n(%)]
Table 3. The comparison of the genotype and allele frequencies of SLC2A9 gene SNPs [n(%)]
SNPs 基因型/等位基因 试验组(n = 294) 对照组(n = 220) χ2 P OR(95%CI) rs2280205 野生GG 152(51.7) 133(60.5) 6.568 0.037* AA 20(6.8) 6(2.7) AG 122(41.5) 81(36.8) A 162(27.5) 93(21.1) 5.552 0.018* 1.419(1.060~1.900) G 426(72.5) 347(78.9) HWE平衡P值 0.9000 0.478 rs3733591 野生CC 40(13.6) 54(24.5) 12.791 0.002* TT 122(41.5) 66(30.0) CT 132(44.9) 100(45.5) C 212(36.1) 208(47.3) 13.108 < 0.001* 1.590(1.236~2.045) T 376(63.9) 232(52.7) HWE平衡P值 0.938 0.633 rs3775948 野生GG 52(17.7) 79(35.9) 26.277 < 0.001* CC 118(40.1) 53(24.1) GC 124(42.2) 88(40.0) G 228(38.8) 246(55.9) 29.732 < 0.001* 2.002(1.558~2.573) C 360(61.2) 194(44.1) HWE平衡P值 0.383 0.153 rs10939650 野生CC 82(27.9) 69(31.4) 25.157 < 0.001* TT 92(31.3) 28(12.7) TC 120(40.8) 123(55.9) T 304(51.7) 179(40.7) 12.267 < 0.001* 1.561(1.216~2.003) C 284(48.3) 261(59.3) HWE平衡P值 0.089 0.259 OR:比值比;95%CI:95%置信区间。*P < 0.05。
下载: 导出CSV
表 4 SLC2A9基因SNPs与PIHU的风险相关性(经调整性别、年龄后)[n(%)]
Table 4. Association between SNPs of SLC2A9 gene and the risk for PIHU (after adjustment for gender and age) [n(%)]
SNPs 遗传模型 基因型 OR 95%CI P rs2280205 共显性 野生GG 1.000 AA 2.917 1.138~7.478 0.021* AG 1.318 0.915~1.898 0.138 显性 AA+AG vs. GG 1.428 1.002~2.035 0.048* 隐性 AA vs. GG+AG 2.603 1.028~6.596 0.037* rs3733591 共显性 野生CC 1.000 TT 2.495 1.503~4.142 0.000* CT 1.782 1.098~2.893 0.019* 显性 TT+CT vs. CC 2.066 1.313~3.250 0.002* 隐性 TT vs. CC+CT 1.655 1.143~2.396 0.007* rs3775948 共显性 野生GG 1.000 CC 3.382 2.099~5.450 <0.001* GC 2.141 1.373~3.337 0.001* 显性 CC+GC vs. GG 2.607 1.736~3.917 <0.001* 隐性 CC vs. GG+GC 1.297 0.883~1.906 0.185 rs10939650 共显性 野生CC 1.000 TT 2.765 1.627~4.700 <0.001* TC 0.821 0.546~1.233 0.342 显性 TT+TC vs. CC 1.181 0.806~1.731 0.392 隐性 TT vs. CC+TC 3.123 1.958~4.981 <0.001* *P<0.05。
下载: 导出CSV
-
[1] 韩珂卿,余林红,崔嘉佳,等. 202例患者应用吡嗪酰胺后的不良反应分析[J]. 临床医学研究与实践,2019,4(14):116-117. doi: 10.19347/j.cnki.2096-1413.201914046 [2] 杨东,闫京京,侯瑞军,等. 吡嗪酰胺引起高尿酸血症的危险因素分析[J]. 中国现代医生,2022,60(19):40-42. doi: 10.3969/j.issn.1673-9701.2022.19.zwkjzlml-yyws202219009 [3] 田娜妮,何青青,朱琳,等. 吡嗪酰胺相关高尿酸血症的影响因素分析[J]. 中国医药导刊,2022,24(4):389-392. doi: 10.3969/j.issn.1009-0959.2022.04.016 [4] Şişmanlar T,Aslan A T,Budakoğlu I. Is hyperuricemia overlooked when treating pediatric tuberculosis patients with pyrazinamide?[J]. J Trop Pediatr,2015,61(5):351-356. doi: 10.1093/tropej/fmv042 [5] 马瑛龙,叶强,杨正贵,等. 肺结核患者服用吡嗪酰胺引起血尿酸水平变化58例分析[J]. 宁夏医学杂志,2021,43(10):921-923. doi: 10.13621/j.1001-5949.2021.10.0921 [6] 彭惠,申恩瑞,马世武. 吡嗪酰胺诱导的高尿酸血症[J]. 传染病信息,2018,31(4):376-380. doi: 10.3969/j.issn.1007-8134.2018.04.019 [7] 申恩瑞,彭惠,陈青,等. 停用吡嗪酰胺对初治结核病患者血尿酸水平的影响[J]. 广东医学,2018,39(24):3701-3705. doi: 10.3969/j.issn.1001-9448.2018.24.027 [8] Enomoto A,Kimura H,Chairoungdua A,et al. Molecular identification of a renal urate anion exchanger that regulates blood urate levels[J]. Nature,2002,417(6887):447-452. doi: 10.1038/nature742 [9] Mandal A K,Mount D B. The molecular physiology of uric acid homeostasis[J]. Annu Rev Physiol,2015,77(1):323-345. doi: 10.1146/annurev-physiol-021113-170343 [10] Nakanishi T,Ohya K,Shimada S,et al. Functional cooperation of URAT1 (SLC22A12) and URATv1 (SLC2A9) in renal reabsorption of urate[J]. Nephrol Dial Transplant,2013,28(3):603-611. doi: 10.1093/ndt/gfs574 [11] Anzai N,Ichida K,Jutabha P,et al. Plasma urate level is directly regulated by a voltage-driven urate efflux transporter URATv1 (SLC2A9) in humans[J]. J Biol Chem,2008,283(40):26834-26838. doi: 10.1074/jbc.C800156200 [12] 姬志祥,蓝常贡. 尿酸盐转运蛋白在痛风中的多态性和治疗相关性[J]. 中国组织工程研究,2021,25(8):1290-1298. doi: 10.3969/j.issn.2095-4344.3039 [13] 彭江丽,陈洁,陈永刚,等. SLC22A12基因多态性与吡嗪酰胺诱导高尿酸血症的易感性研究[J]. 中国防痨杂志,2023,45(2):151-158. doi: 10.19982/j.issn.1000-6621.20220315 [14] 彭江丽,刘晖,朱江春,等. 云南地区结核病患者人尿酸盐转运蛋白1基因单核苷酸多态性与吡嗪酰胺导致高尿酸血症的相关性研究[J]. 抗感染药学,2022,19(1):17-21. [15] 中华人民共和国国家卫生健康委员会. 肺结核诊断WS 288—2017[J]. 中国感染控制杂志,2018,17(7):642-652. [16] 郭立新. 无症状高尿酸血症合并心血管疾病诊治建议中国专家共识解读[J]. 中国实用内科杂志,2011,31(4):271-273. [17] Merriman T R. An update on the genetic architecture of hyperuricemia and gout[J]. Arthritis Res Ther,2015,17(1):98. doi: 10.1186/s13075-015-0609-2 [18] Wang Z,Cui T,Ci X,et al. The effect of polymorphism of uric acid transporters on uric acid transport[J]. J Nephrol,2019,32(2):177-187. doi: 10.1007/s40620-018-0546-7 [19] Döring A,Gieger C,Mehta D,et al. SLC2A9 influences uric acid concentrations with pronounced sex-specific effects[J]. Nat Genet,2008,40(4):430-436. doi: 10.1038/ng.107 [20] Nkeck J R,Singwé N M,Ama M V,et al. Genetic analysis for rs2280205 (A>G) and rs2276961 (T>C) in SLC2A9 polymorphism for the susceptibility of gout in Cameroonians: A pilot study[J]. BMC Res Notes,2018,11(1):230. doi: 10.1186/s13104-018-3333-6 [21] Liu W C,Hung C C,Chen S C,et al. The rs1014290 polymorphism of the SLC2A9 gene is associated with type 2 diabetes mellitus in Han Chinese[J]. Exp Diabetes Res,2011,2011(1):527520. [22] 郑军. SLC2A9基因第九外显子rs2280205多态性与高尿酸血症合并糖尿病的易感性研究[D]. 青岛: 青岛大学硕士学位论文, 2012. [23] 李敏,杨静,周京国,等. 葡萄糖转运体9基因rs3733591(C>T)的单核苷酸多态性与我国汉族人群原发性痛风发病的相关性研究[J]. 中华风湿病学杂志,2014,18(10):655-660. [24] 霍晓聪,黄新翔,朱霞,等. 广西壮族人群SLC2A9基因多态性位点与原发性痛风的关联性研究[J]. 中国临床新医学,2021,14(11):1080-1086. doi: 10.3969/j.issn.1674-3806.2021.11.05 [25] 应颖,黄海燕,邹荣鑫,等. 尿酸转运蛋白相关基因多态性与原发性痛风遗传易感性关系的荟萃分析[J]. 浙江医学,2017,39(20):1763-1770. doi: 10.12056/j.issn.1006-2785.2017.39.20.2017-2019 [26] Zhang X,Yang X,Wang M,et al. Association between SLC2A9 (GLUT9) gene polymorphisms and gout susceptibility: An updated meta-analysis[J]. Rheumatol Int,2016,36(8):1157-1165. doi: 10.1007/s00296-016-3503-6 [27] 李瑞,秦丽岩,谢昆,等. SLC2A9基因R265H位点单核苷酸多态性与痛风易感性的Meta分析[J]. 新疆医科大学学报,2016,39(3):301-307. doi: 10.3969/j.issn.1009-5551.2016.03.010 [28] Tu H P,Chen C J,Tovosia S,et al. Associations of a non-synonymous variant in SLC2A9 with gouty arthritis and uric acid levels in Han Chinese subjects and Solomon Islanders[J]. Ann Rheum Dis,2010,69(5):887-890. doi: 10.1136/ard.2009.113357 [29] 蒲强红,李佳萌,李凡敏,等. 结核病化疗药物吡嗪酰胺致高尿酸血症的危险因素研究[J]. 中华全科医学,2021,19(12):2058-2060. doi: 10.16766/j.cnki.issn.1674-4152.002236 [30] Charles B A,Shriner D,Doumatey A,et al. A genome-wide association study of serum uric acid in African Americans[J]. BMC Med Genomics,2011,4(1):17. doi: 10.1186/1755-8794-4-17 [31] Rivera-Paredez B,Macías-Kauffer L,Fernandez-Lopez J C,et al. Influence of genetic and non-genetic risk factors for serum uric acid levels and hyperuricemia in mexicans[J]. Nutrients,2019,11(6):1336. doi: 10.3390/nu11061336 [32] Li Z,Zhou Z,Hou X,et al. Replication of gout/urate concentrations GWAS susceptibility loci associated with gout in a Han Chinese population[J]. Sci Rep,2017,7(1):4094. doi: 10.1038/s41598-017-04127-4 [33] Yan D,Wang J,Jiang F,et al. Association between serum uric acid related genetic loci and diabetic kidney disease in the Chinese type 2 diabetes patients[J]. J Diabetes Complications,2016,30(5):798-802. doi: 10.1016/j.jdiacomp.2016.02.018 [34] 孙雪. 尿酸与糖代谢的相关性及遗传关联分析[D]. 上海: 上海交通大学硕士学位论文, 2015. [35] 张亚弟. SLC2A9、ADRB3、GNB3基因多态性与高尿酸血症的关联研究[D]. 银川: 宁夏医科大学硕士学位论文, 2018. [36] Chittoor G,Haack K,Balakrishnan P,et al. Fine mapping and identification of serum urate loci in American Indians: The strong heart family study[J]. Sci Rep,2019,9(1):17899. doi: 10.1038/s41598-019-52924-w -



 点击查看大图
点击查看大图
计量
- 文章访问数: 4482
- HTML全文浏览量: 2766
- PDF下载量: 12
- 被引次数: 0
