

Comparative Study of Multiple Models Based on Baseline T2WI Images for Predicting Pathological Complete Remission of Progressive Rectal Cancer after Neo-adjuvant Chemoradiotherapy
-
摘要:
目的 探究基于基线T2WI联合机器学习影像组学,预测进展期直肠癌(locally advanced rectal cancer,LARC)患者对新辅助同期放化疗(neo-adjuvant chemoradiotherapy,nCRT)后病理完全缓解的有效性及多种模型预测效能比较。 方法 回顾性分析了2017年1月至2021年12月期间131例非转移性进展期直肠癌的患者资料,患者均在治疗前后进行盆腔MRI检查,并接受标准nCRT治疗后进行直肠全系膜切除术(total mesorectal excision,TME)。采用AK软件(Analysis Kit,GE Healthcare)在新辅助治疗前在轴向T2WI图上手动勾画感兴趣区(region of interest,ROI),通过AK软件提取影像组学特征。运用双样本t检验+LASSO回归对影像组学特征进行特征筛选,将筛选的影像组学数据,分别采用随机森林(random forest,RF)、支持向量机 (support vector machine,SVM)、逻辑回归(logistic regression,LR)方法构建预测模型。采用受试者工作特征(ROC)曲线来分别检验三种模型预测效能。 结果 131例患者中,26例(19.8%)达到病理完全缓解(pathologic complete response,pCR)。通过AK软件共提取1 308个影像组学特征,经筛选保留12个特征对pCR进行预测,3个预测模型在测试集上都展现了不错的预测效能,支持向量机(SVM)预测模型的曲线下面积(area under curve,AUC)为0.8810,准确率为81.48%,灵敏度和特异度分别为90.48%和50%;随机森林(RF)预测模型AUC为0.7579,准确率为81.48%,灵敏度和特异度分别为95.24%和33.33%;逻辑回归(LR)预测模型AUC为0.9206,准确率为92.59%,灵敏度和特异度分别为95.24%和83.33%。 结论 所构建的3种机器学习模型,在预测局部进展期直肠癌放化同期治疗后病理完全缓解方面有可观的准确率,其中采用逻辑回归(LR)方法建立的机器学习模型较其他机器学习模型诊断效能更高,有潜力应用于临床实践。 Abstract:Objective To investigate the predictive effectiveness of different models and the efficacy of baseline T2WI combined with machine learning imaging and to predict the pathological complete remission after the neo-adjuvant chemoradiotherapy (nCRT) in patients with locally advanced rectal cancer (LARC). Methods A retrospective analysis was conducted on the data of 131 patients with non metastatic advanced rectal cancer from January 2017 to December 2021. All patients underwent the pelvic MRI examination before and after the treatment, received standard nCRT treatment, and then underwent the total mesorectal resection (TME). AK software (Analysis Kit, GE Healthcare) was used to manually draw the regions of interest (ROI) on the pre-treatment axial T2WI maps, and AK software also extracted the imaging omics features. The imaging omics data were used to build the prediction models by using the support vector machine (SVM), random forest (RF), and logistic regression (LR) methods after the the imaging omics features were feature-screened using a two-sample t-test + LASSO regression. The effectiveness of the model prediction was evaluated using the receiver operating characteristic curve (ROC). Results 26 (19.8%) of the 131 patients had a pathologic complete response (pCR). The AK software extracted 1308 imaging omics features in total, and after the screening, 12 features were selected for pCR prediction. The SVM model had an AUC, accuracy of 0.8810 and 81.48%, sensitivity and specificity of 90.48% and 50%. The RF model had an AUC, accuracy of 0.7579 and 81.48%, sensitivity and specificity of accuracy 95.24% and 33.33%. The LR model had an AUC, accuracy of 0.9206 and 92.59%, sensitivity and specificity of 95.24% and 83.33%. Conclusion The three machine learning models constructed have the considerable accuracy in predicting complete pathological remission after the concurrent radiotherapy and chemotherapy for locally advanced rectal cancer. Among them, the machine learning model established with the use of logistic regression (LR) method has the higher diagnostic efficiency than other machine learning models, and has the potential to be applied in the clinical practice. -

图 1 患者基线轴位T2WI图上ROI绘制、病理学表现和病理完全缓解病理学表现
A:患者基线病理学表现 (H-E×400); B:患者病理完全缓解病理学表现(H-E×400); C:患者基线轴位T2W1图上ROI绘制。
Figure 1. ROI on patient baseline T2WI、pathological manifestations and pathological complete response of pathological manifestations

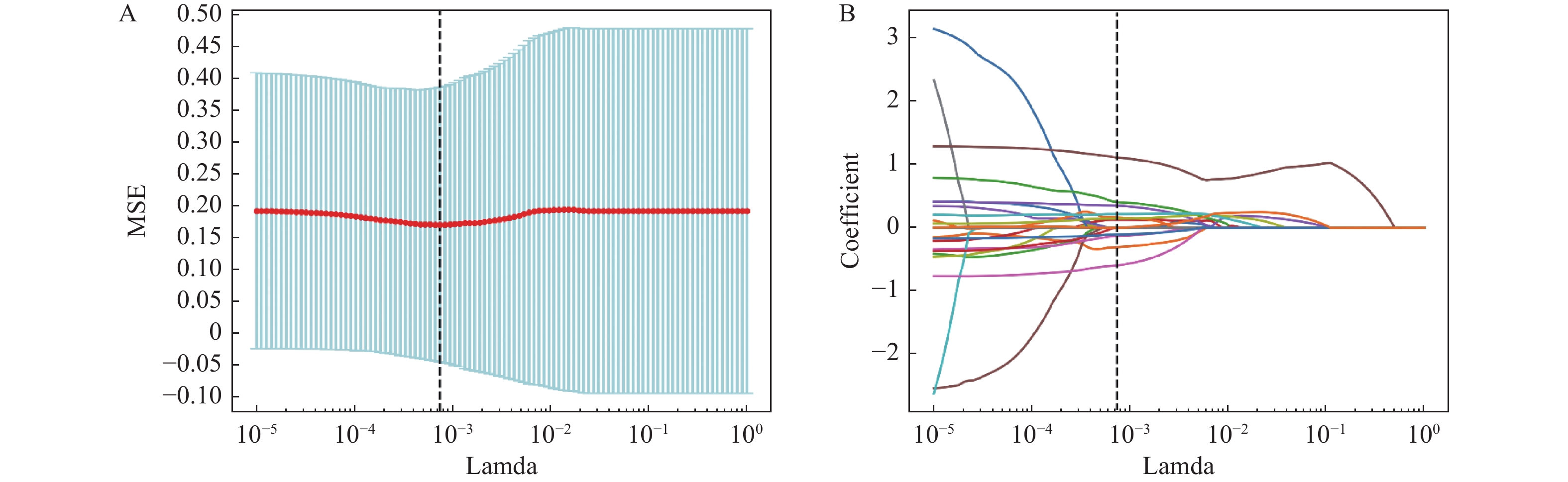
图 2 LASSO回归筛选特征参数系数图
A:通过10次交叉验证寻找LASSO的超参数Lamda(λ),模型偏差最低点对应的横坐标为最优的Lamda(λ)值,即虚线所在位置;B:图示彩线代表特征系数随λ值的变化曲线,通过Lamda(λ)值(虚线代表的位置)来确定最终非零系数特征,并将这些特征用于最后的模型构建。
Figure 2. LASSO regression screening feature parameter coefficient map

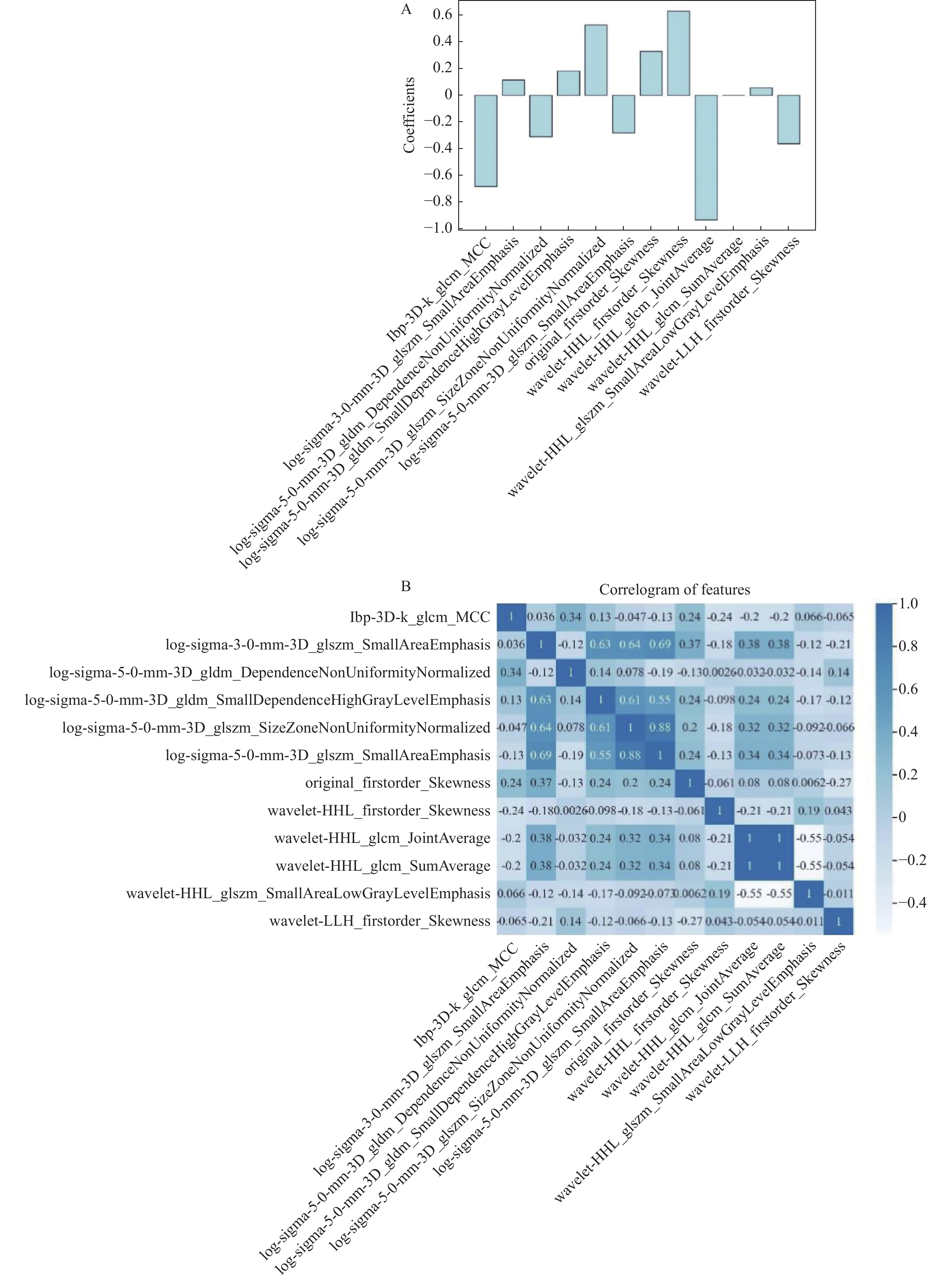
图 3 影像特征及影像组学标签
A:12个筛选出的影像特征权重图;B:该矩阵图显示了预测模型中所用特征之间的相关性。
Figure 3. Image features and radiomics labels

图 4 基线T2WI预测LARC患者nCRT治疗后达pCR预测模型ROC曲线
Figure 4. Baseline T2WI predicts the ROC curve of the pCR prediction model for LARC patients after nCRT treatment
表 1 直肠癌MRI扫描序列及参数
Table 1. MRI scan series and parameters of rectal cancer
扫描序列 TR/ms TE/ms 层厚/mm 层间隔/mm 视野 激励次数 矩阵 轴位T2WI 4101 90 3 0.3 220 mm×220 mm 2 264×240 冠状位T2WI 4101 90 3 0.3 200 mm×200 mm 2 288×256 矢状位T2WI 4101 90 3 0.3 200 mm×200 mm 2 288×256 垂直于直肠长轴T2WI 4101 90 3 0.3 200 mm×200 mm 2 264×240  下载: 导出CSV
下载: 导出CSV
表 2 临床流行病学特征[(
$\bar x \pm s $ )/n(%)]Table 2. Clinical epidemiological characteristics [(
$\bar x \pm s $ )/n(%)]训练集(n = 104) 测试集(n = 27) 特征 pCR(n = 20) 非pCR(n = 84) P t/χ2 pCR(n = 6) 非pCR(n = 21) P t/χ2 年龄(岁) 59 ± 10.3 57.45 ± 11.82 0.591 0.539 49.5 ± 7.94 58.33 ± 12.97 0.129 1.572 性别 0.108 2.589 0.127 2.328 男 10(50) 26(31) 3(50) 4(19) 女 10(50) 58(69) 3(50) 17(81) 分化程度 0.334 2.193 0.480 1.467 高分化 16(80) 58(69) 5(91) 18(86) 中分化 4(20) 18(21) 1(9) 1(4) 低分化 0 8(10) 0 2(10) MRI肿瘤T分期 0.132 4.046 0.793 0.464 T0/1/2 0 4(5) 0 1(5) T3a/b/c 15(75) 43(51) 4(67) 15(71) T4 5(15) 37(44) 2(33) 5(24) MRI肿瘤N分期 0.129 4.089 0.825 0.386 N0 3(15) 3(3) 1(16.5) 5(24) N1 4(20) 15(18) 1(16.5) 5(24) N2 13(65) 66(79) 4(67) 11(52)
下载: 导出CSV
表 3 Lasso回归筛选特征及其权重系数
Table 3. Lasso regression screening features and their weight coefficients
特征 权重系数 lbp-3D-k_glcm_MCC −0.691 log-sigma-3-0-mm-3D_glszm_SmallAreaEmphasis 0.113 log-sigma-5-0-mm-3D_gldm_DependenceNonUniformityNormalized −0.305 log-sigma-5-0-mm-3D_gldm_SmallDependenceHighGrayLevelEmphasis 0.193 log-sigma-5-0-mm-3D_glszm_SizeZoneNonUniformityNormalized 0.524 log-sigma-5-0-mm-3D_glszm_SmallAreaEmphasis −0.286 original_firstorder_Skewness 0.324 wavelet-HHL_firstorder_Skewness 0.628 wavelet-HHL_glcm_JointAverage −0.912 wavelet-HHL_glcm_SumAverage 0.009 wavelet-HHL_glszm_SmallAreaLowGrayLevelEmphasis 0.078 wavelet-LLH_firstorder_Skewness −0.375
下载: 导出CSV
表 4 预测临床结局最终模型的诊断指标
Table 4. Diagnostic indicators of the final model for predicting clinical outcomes
项目 训练集 验证集 测试集 模型 支持向量机(SVM) 随机森林(RF) 逻辑回归(LR) 支持向量机(SVM) 随机森林(RF) 逻辑回归(LR) 支持向量机(SVM) 随机森林(RF) 逻辑回归(LR) AUC 0.9979
(95% CI:
99.5~100)1.0000
(95% CI:
100~100)0.8868
(95% CI:
84.06~92.39)0.9115
(95% CI:
79.85~99.09)0.9789
(95% CI:
95.68~99.56)0.8493
(95% CI:
72.86~95.52)0.8810
(95% CI:
76~98.18)0.7579
(95% CI:
57.86~91.67)0.9206
(95% CI:
80.56~100)准确度 0.9702
(95% CI:
94.64~98.81)1.0000
(95% CI:
100~100)0.7857
(95% CI:
94.64~98.81)0.8813
(95% CI:
79.22~95.85)0.9228
(95% CI:
84.56~98.22)0.7554
(95% CI:
63.05~86.86)0.8148
(95% CI:
70.37~92.59)0.8148
(95% CI:
66.67~92.59)0.9259
(95% CI:
85.19~100)灵敏度 0.9643
(95% CI:
92.68~98.92)1.0000
(95% CI:
100~100)0.7738
(95% CI:
69.32~84.72)0.8114
(95% CI:
67.26~93.46)0.8879
(95% CI:
77.26~97.99)0.7485
(95% CI:
55.87~91.03)0.9048
(95% CI:
80~100)0.9524
(95% CI:
85.71~100)0.9524
(95% CI:
86.36~100)特异度 0.9762
(95% CI:
94.57~100)1.0000
(95% CI:
100~100)0.7976
(95% CI:
72.34~87.1)0.9332
(95% CI:
84.34~98.89)0.9889
(95% CI:
96~99.31)0.7674
(95% CI:
62.23~91.17)0.5000
(95% CI:
16.67~85.71)0.3333
(95% CI:
0~66.67)0.8333
(95% CI:
57.14~100)
下载: 导出CSV
-
[1] 郑荣寿,张思维,孙可欣,等. 2016年中国恶性肿瘤流行情况分析[J]. 中华肿瘤杂志,2023,45(3):212-220. [2] Siegel R L,Miller K D,Goding Sauer A,et al. Colorectal cancer statistics,2020[J]. CA:A Cancer Journal for Clinicians,2020,70(3):145-164. doi: 10.3322/caac.21601 [3] Arnaldo Stanzione,Francesco Verde,Valeria Romeo,et al. Radiomics and machine learning applications in rectal cancer:Current update and future perspectives[J]. World J Gastroenterol,2021,27(32):5306-5321. doi: 10.3748/wjg.v27.i32.5306 [4] Kanani A,Veen T,Søreide K. Neoadjuvant immunotherapy in primary and metastatic colorectal cancer[J]. The British Journal of Surgery,2021,108(12):1417-1425. doi: 10.1093/bjs/znab342 [5] Shimizu H,Nakayama K I. Artificial intelligence in oncology[J]. Cancer science,2020,111(5):1452-1460. doi: 10.1111/cas.14377 [6] Lambin P,Rios-Velazquez E,Leijenaar R,et al. Radiomics: Extracting more information from medical images using advanced feature analysis[J]. European Journal of Cancer (Oxford,England:1990),2012,48(4):441-446. [7] Aerts H J W L,Velazquez E R,Leijenaar R T H,et al. Erratum: Corrigendum: Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach[J]. Nature Communications,2014,5(1):1-8. [8] Gillies R J,Kinahan P E,Hricak H. Radiomics: Images are more than pictures,they are data[J]. Radiology,2016,278(2):563-577. doi: 10.1148/radiol.2015151169 [9] Horvat N,Veeraraghavan H,Khan M,et al. MR imaging of rectal cancer: Radiomics analysis to assess treatment response after neoadjuvant therapy[J]. Radiology,2018,287(3):833-843. doi: 10.1148/radiol.2018172300 [10] Avanzo M,Wei L,Stancanello J,et al. Machine and deep learning methods for radiomics[J]. Medical physics,2020,47(5):e185-e202. [11] Zhang X Y,Wang L,Zhu H T,et al. Predicting rectal cancer response to neoadjuvant chemoradiotherapy using deep learning of diffusion kurtosis MRI[J]. Radiology,2020,296(1):56-64. doi: 10.1148/radiol.2020190936 [12] Shin J,Seo N,Baek S E,et al. MRI radiomics model predicts pathologic complete response of rectal cancer following chemoradiotherapy[J]. Radiology,2022,303(2):351-358. doi: 10.1148/radiol.211986 [13] Liu Z,Zhang X Y,Shi Y J,et al. Radiomics analysis for evaluation of pathological complete response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer[J]. Clinical Cancer Research:An Official Journal of the American Association for Cancer Research,2017,23(23):7253-7262. doi: 10.1158/1078-0432.CCR-17-1038 [14] Yi X,Pei Q,Zhang Y,et al. MRI-based radiomics predicts tumor response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer[J]. Frontiers in Oncology,2019,9(9):552. [15] Horvat N,Bates D D B,Petkovska I. Novel imaging techniques of rectal cancer: What do radiomics and radiogenomics have to offer? A literature review[J]. Abdominal Radiology (New York),2019,44(11):3764-3774. doi: 10.1007/s00261-019-02042-y [16] Hiram Shaish,Andrew Aukerman,Rami Vanguri,et al. Radiomics of MRI for pretreatment prediction of pathologic complete response,tumor regression grade,and neoadjuvant rectal score in patients with locally advanced rectal cancer undergoing neoadjuvant chemoradiation: An international multicenter study[J]. Eur Radiol,2020,30(11):6263-6273. doi: 10.1007/s00330-020-06968-6 [17] Antunes J T,Ofshteyn A,Bera K,et al. Radiomic features of primary rectal cancers on baseline T2 -weighted MRI are associated with pathologic complete response to neoadjuvant chemoradiation: A multisite study[J]. Journal of Magnetic Resonance Imaging:JMRI,2020,52(5):1531-1541. doi: 10.1002/jmri.27140 -




 点击查看大图
点击查看大图

计量
- 文章访问数: 3659
- HTML全文浏览量: 2310
- PDF下载量: 6
- 被引次数: 0
