

Clinical Investigation on Foure-dimensional Left Atrial Automatic Quantitative Technology in Evaluating Left Atrial Volume and Function
-
摘要:
目的 探讨四维左心房自动定量(4D Auto LAQ)技术对非选择性连续患者左心房的容积及功能的应用价值。 方法 187例入选患者中成功分析143例患者。应用4D Auto LAQ 技术及Simpson’s双平面技术分别获取左房整体射血分数(LAEF)、左房最大容积指数(LAVImax)、左心房舒张末期容积(LAVmax)、左心房收缩末期容积(LAVmin),同时记录分析时间,比较2种技术所测参数的准确性及可重复性。 结果 4D Auto LAQ 技术及Simpson’s双平面技术所测值相关性高(r值:LAVmax 0.91,LAVmin 0.89,LAVI0.90,LAEF 0.54;P < 0.01)、一致性较好[平均测量差异:LAVmax1 0.1 mL,LAVmin 3.1 mL,LAVI 6.4 mL,LAEF 10.0%;一致性区间:LAVmax(-30.7-50.9) mL,LAVmin(-32.2-38.4) mL,LAVI(-21.2-34.1) mL,LAEF(-19.8-39.8)%]。4D Auto LAQ 技术对不同心动周期各测量值相关性好(r值:LAVmax 0.99,LAVmin 0.98,LAVImax 0.99,LAEF 0.92;P < 0.01),一致性区间为[LAVmax(-8.9-7.9) mL,LAVmin(-7.9-10.8) mL,LAVI(-7.9-10.8) mL/m2,LAEF(-14.8-9.1)%]。4D Auto LAQ 技术各测量值在观察者内部、观察者间的重复性均较好(组内相关系数均 > 0.8,变异系数均 < 10%),且优于Simpson’s双平面法。4D Auto LAQ 技术技术用时较Simpson’s双平面法明显减少,分别为(30.87±5.05) s、(60.20±5.05) s,(P < 0.05)。 结论 4D Auto LAQ 技术评价左心房容积及功能用时更短,重复性好,具有临床推广价值。 -
关键词:
- 四维左心房自动定量分析 /
- Simpson’s法 /
- 左心房功能 /
- 左心房容积
Abstract:Objective To explore the role of four-dimensional left atrial automatic quantitative technology in evaluating the volume and function of the left atrium in non-selective continuous patients, and to preliminarily explore its accuracy and repeatability. Methods Foure-dimensional left atrial full-volume dynamic images of 187 consecutive patients were collected, 44 patients who failed the analysis were excluded, and 143 were successfully analyzed. Using Simpson’s biplane method as the reference standard, the 4D Auto LAQ technology was used to evaluate the left atrial end-diastolic volume (LAVmax), left atrial end-systolic volume (LAVmin), left atrial maximum volume index (LAVImax), and left atrial global ejection fraction. (LAEF) accuracy and repeatability. Results In all patients who were successfully analyzed, the inter-technique comparisons showed good correlations (R-values: LAVmax 0.91, LAVmin 0.89, LAVI 0.90, LAEF 0.54; all P < 0.01), small biases ( LAVmax 10.1 mL, LAVmin 3.1 mL, LAVI 6.4 mL, LAEF 10.0%; Concordance interval: LAVmax (-30.7-50.9) mL, LAVmin (-32.2-38.4) mL, LAVI (-21.2-34.1) mL, LAEF (-19.8-39.8)%] for all measurements in all patients. 4D Auto LAQ technology showed good correlation between the parameters of different cardiac cycles (r value: LAVmax 0.99, LAVmin 0.98, LAVImax 0.99, LAEF 0.92; all P < 0.01), and the average measurement difference did not exceed two measurement units (1 mL/volume, 1%/LAEF), the consistency interval is also narrow [LAVmax (-8.9-7.9) mL, LAVmin (-7.9-10.8) mL, LAVI (-7.9-10.8) mL/m2, LAEF (-14.8-9.1)%. The intra- and inter-observer repeatability of each parameter of 4D Auto LAQ technology was good (within-group correlation coefficients were all > 0.8, 0.81-0.99, and coefficients of variation were all < 10%), and it was better than Simpson’s biplane method. Compared with Simpson’s biplane method, the time of 4D Auto LAQ quantitative technology was significantly reduced, which were (30.87±5.05)s and (60.20±5.05)s respectively (P < 0.05). Conclusions Since4D Auto LAQ technology can be widely used in clinical practice as a feasible and objective ultrasound technique. -

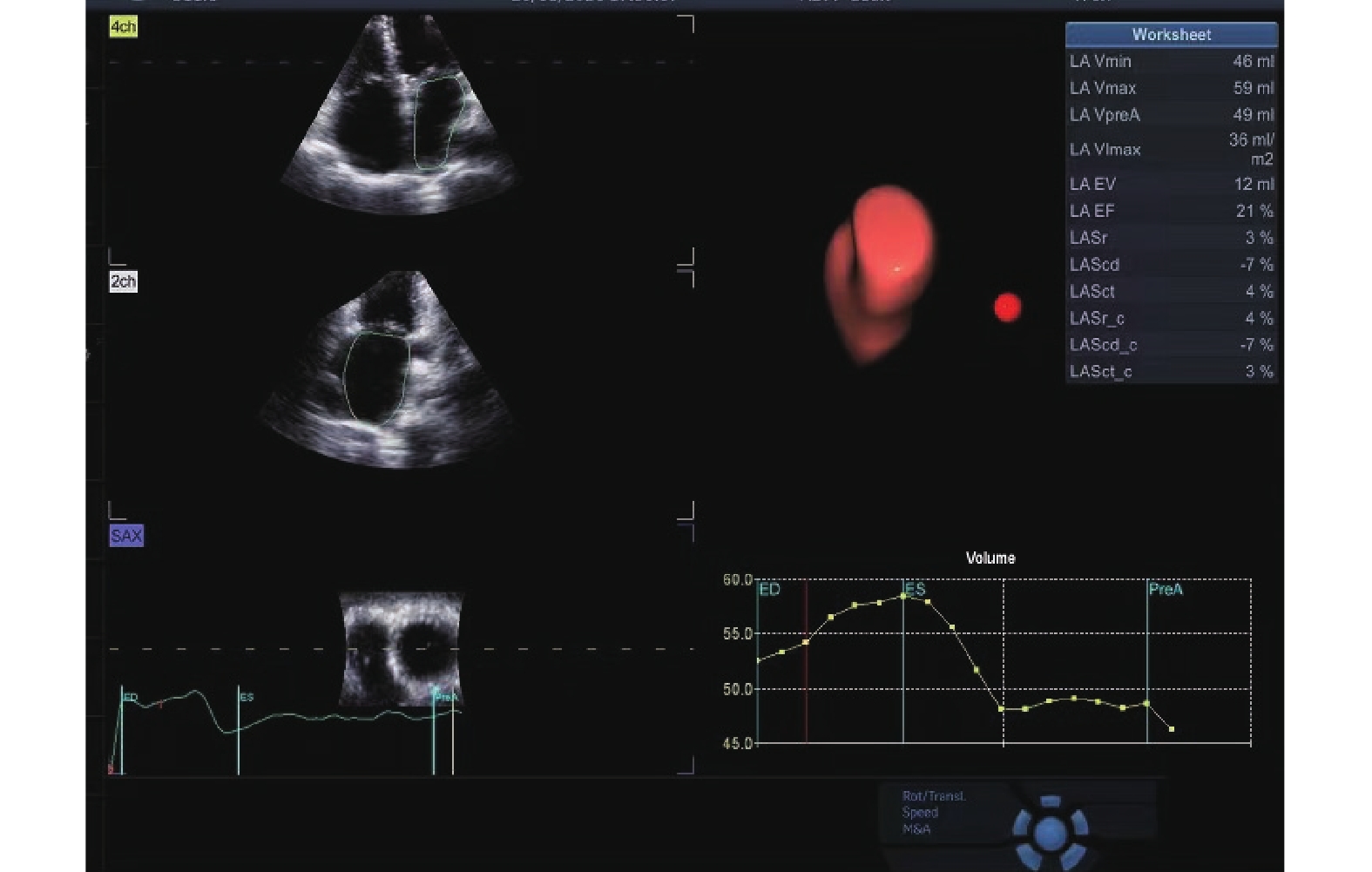
图 1 四维左心房自动定量分析(4D Auto LAQ)技术所获得的左心房容积及功能结果及左心房三维模型图
Figure 1. Left atrial volume and function results obtained by 4D Auto LAQ technology,as well as three-dimensional model of the left atrium

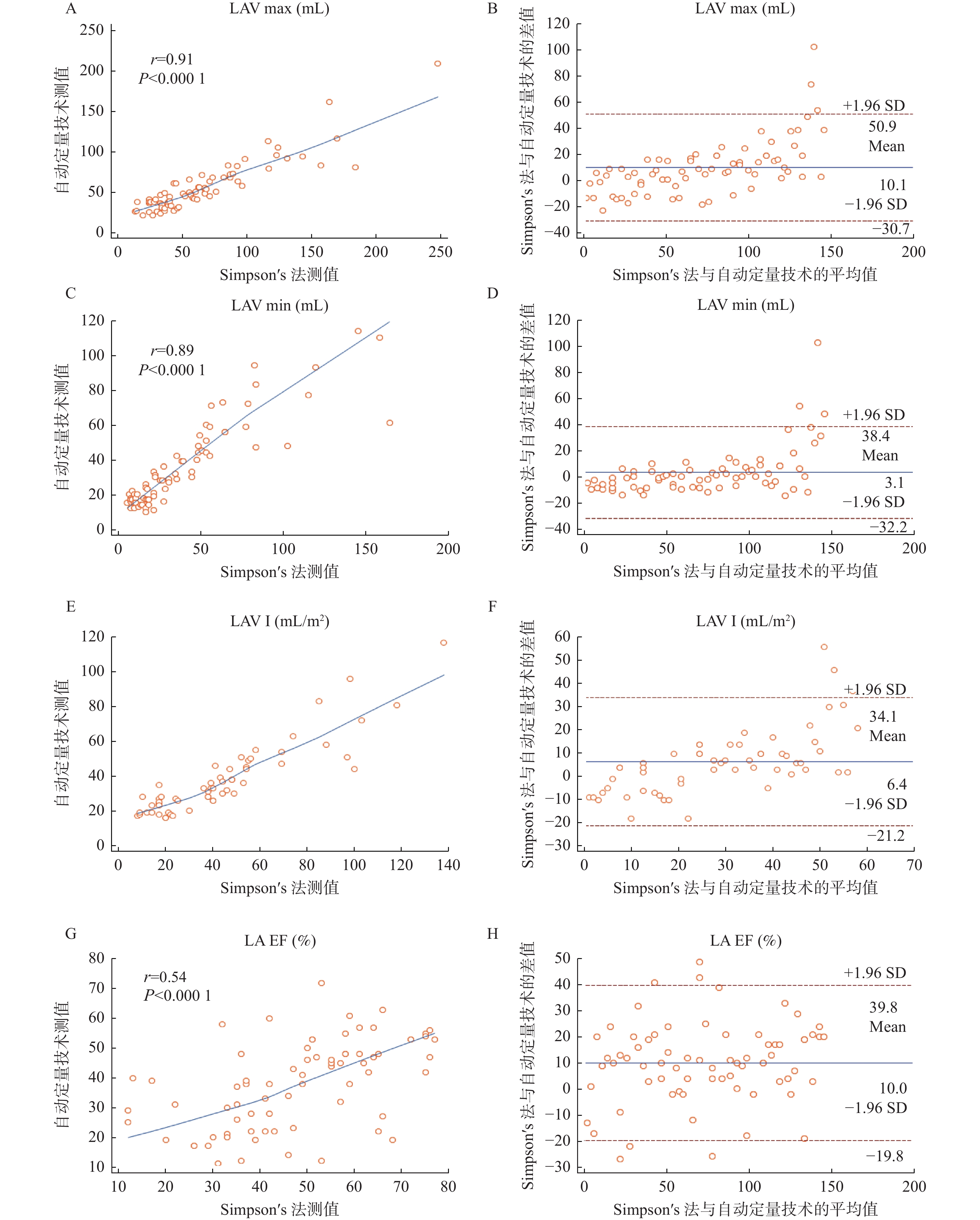
图 2 所有患者与Simpson’s双平面法法测值的相关性及Bland-Altman一致性检验
A、B:LAVmax;C、D:LAVmin ;E、F:LAVI;G、H:LAEF。
Figure 2. Correlation and Bland Altman consistency test between all patients and Simpson’s biplane method measurements
表 1 4D Auto LAQ技术与Simpson’s双平面法各参数的相关性和一致性分析(
$\bar x \pm s $ )Table 1. Comparison,correlation and consistency analysis of parameters between 4D Auto LAQ technology and Simpson’s biplane method (
$\bar x \pm s $ )变量 n 4D Auto LAQ技术 Simpson’s法 r P 平均测量差异 一致性区间 LAVmax(mL) 全部 150 56.86 ± 31.4 66.99 ± 44.4 0.91 < 0.0001* 10.1 −30.7-50.9 左房正常组 56 30.91 ± 7.0 32.43 ± 7.2 0.58 < 0.0001* 4.3 −11.7-20.4 左房扩大组 94 76.45 ± 33.73 99.11 ± 43.47 0.87 < 0.0001* 22.7 −19.6-64.9 LAVmin(mL) 全部 150 36.49 ± 24.27 39.63 ± 35.86 0.89 < 0.0001* 3.1 −32.2-38.4 左房正常组 56 15.07 ± 4.9 13.26 ± 4.2 0.51 < 0.0001* −1.8 −11.0-7.4 左房扩大组 94 53.51 ± 23.82 64.65 ± 37.17 0.81 < 0.0001* 11.1 −33.2-55.5 LAVImax(mL/m2) 全部 150 37.69 ± 20.57 44.14 ± 29.59 0.90 < 0.0001* 6.4 −21.2-34.1 左房正常组 56 21.86 ± 5.09 20.90 ± 4.18 0.72 < 0.0001* −1.0 −7.9-6.0 左房扩大组 96 46.86 ± 20.50 60.03 ± 26.12 0.88 < 0.0001* 13.2 −12.0-38.4 LAEF(%) 全部 150 37.99 ± 14.7 48.00 ± 16.72 0.54 < 0.0001* 10.0 −19.8-39.8 左房正常组 56 43.56 ± 14.69 62.61 ± 11.05 0.51 < 0.0001* 17.1 −6.7-40.9 左房扩大组 94 30.75 ± 11.67 37.61 ± 13.77 0.52 < 0.0001* 6.9 −18.4-32.2 LAVmax:左房最大容积;LAVmin:左最小容积;LAVImax:左房最大容积指数;LVEF:左房整体射血分数。*P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 4D Auto LAQ 技术技术不同心动周期各参数相关性及一致性分析(
$\bar x \pm s $ )Table 2. Correlation and consistency analysis of various parameters of 4D Auto LAQ technology in different Cardiac cycle (
$\bar x \pm s $ )变量 心动周期1 心动周期2 r P 平均测量差异 一致性区间 LAVmax(mL) 56.25 ± 30.4 56.77 ± 28.7 0.99 < 0.0001* −0.5 −8.9-7.9 LAVmin(mL) 35.56 ± 23.7 34.09 ± 21.6 0.98 < 0.0001* 1.5 −7.9-10.8 LAVIma(mL/m2) 37.89 ± 20.4 37.15 ± 19.7 0.99 < 0.0001* 0.7 −4.7-5.6 LAEF(%) 39.9 ± 14.8 42.8 ± 14.9 0.92 < 0.0001* −0.29 −14.8-9.1 *P < 0.05。
下载: 导出CSV
表 3 自动定量技术与Simpson’s双平面法重复性检验(
$\bar x \pm s $ )Table 3. Automatic quantitative technology and Simpson’s biplane method for repeatability testing (
$\bar x \pm s $ )变量 观察者内 观察者间 变异(%) 组内相关系数 变异(%) 组内相关系数 4D Auto LAQ技术 LAVmax 3.99 ± 5.2 0.99 8.81 ± 6.7 0.93 LAVmin 6.63 ± 5.7 0.96 11.2 ± 5.6 0.93 LAVImax 4.32 ± 5.1 0.98 9.26 ± 7.2 0.94 LAEF 6.50 ± 4.2 0.84 8.5 ± 9.2 0.81 Simpson’s法 EDV 9.1 ± 3.9 0.94 11.5 ± 8.9 0.86 ESV 13.66 ± 7.9 0.85 14.36 ± 9.5 0.83 LAVImax 8.3 ± 5.8 0.90 10.2 ± 5.7 0.86 EF 10.5 ± 7.4 0.71 13.6 ± 7.8 0.58
下载: 导出CSV
-
[1] Lang R M,Badano L P,Mor-Avi V,et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American society of echocardiography and the european association of cardiovascular imaging[J]. Eur Heart J Cardiovasc Imaging,2015,16(1):233-270. [2] Yao G H, Deng Y, Liu Y, et al, Echocardiographic measurements in Normal Chinese adults focusing on cardiac chambers and great arteries: A prospective, nationwide, and multicenter study[J]. Journal of the American Society of Echocardiography, 2015, 28(5): 570-579. [3] Sun L,Feng H,Ni L,et al. Realization of fully automated quantification of left ventricular volumes and systolic function using transthoracic 3D echocardiography[J]. Cardiovasc Ultrasound,2018,16(1):2. doi: 10.1186/s12947-017-0121-8 [4] Medvedofsky D,Mor-Avi V,Amzulescu M,et al. Three-dimensional echocardiographic quantification of the left-heart chambers using an automated adaptive analytics algorithm: Multicentre validation study[J]. Eur Heart J Cardiovasc Imaging,2018,19(1):47-58. doi: 10.1093/ehjci/jew328 [5] Chen L,Zhang C,Wang J,et al. Left atrial strain measured by 4D Auto LAQ echocardiography is significantly correlated with high risk of thromboembolism in patients with non-valvular atrial fibrillation.[J]. Quantitative Imaging in Medicine and Surgery,2021,11(9):3920-3931. doi: 10.21037/qims-20-1381 [6] 汤跃跃,张容亮,杨寒凝,等. 经食管实时三维及二维超声心动图在左心耳封堵围术期的应用[J]. 中国医学影像学杂志,2021,29(4):339-342. doi: 10.3969/j.issn.1005-5185.2021.04.012 [7] Thavendiranathan P ,Liu S. Full-volume 3D transthoracic echocardiography to measure LV volumes and systolic functiona fully automated endocardial contouring algorithm in sinus[J]. Journal of theAmerican College of Cardiology,2012,5(3):239-251. [8] 林广,张志强. 人工智能医学影像在骨关节系统中的应用进展[J]. 中国医学影像学杂志,2022,30(2):184-187. doi: 10.3969/j.issn.1005-5185.2022.02.017 [9] 胡彦斌,李亚南,崔存英,等. 四维自动左心房定量分析技术评估心力衰竭患者左心房功能的研究[J]. 中华超声影像学杂志,2022,31(3):7. [10] Luo X X,Fang F,So H K,et al. Automated left heart chamber volumetric assessment using three-dimensional echocardiography in Chinese adolescents[J]. Echo Res Pract,2017,4(4):53-61. doi: 10.1530/ERP-17-0028 [11] Feng C,Chen L,Li J,et al. Three-dimensional echocardiographic measurements using automated quantification software for big data processing[J]. J Xray Sci Technol,2017,25(2):313-321. [12] Spitzer E,Ren B,Soliman O I,et al. Accuracy of an automated transthoracic echocardiographic tool for 3D assessment of left heart cha mber volumes[J]. Echocardiography,2017,34(2):199-209. doi: 10.1111/echo.13436 [13] Laser K T,Karabiyik A,Krperich H,et al. Validation and reference values for three-dimensional echocardiographic right ventricular volumetry in children:A multicenter study[J]. Journal of the American Society of Echocardiography:Official Publication of the American Society of Echocardiography,2018,31(9):1050-1063. [14] Tsang W,Salgo I S,Medvedofsky D,et al. Transthoracic 3D echocardiographic left heart chamber quantification using an automated adaptive analytics algorithm[J]. JACC Cardiovasc Imaging,2016,9(7):769-782. [15] Levy F,Dan S E,Iacuzio L,et al. Performance of new automated transthoracic three-dimensional echocardiographic software for left ventricular volumes and function assessment in routine clinical practice: Comparison with 3 Tesla cardiac magnetic resonance[J]. Arch Cardiovasc Dis,2017,110(11):580-589. [16] Barletta V,Hinojar R,Carbonell A,et al. Three-dimensional full automated software in the evaluation of the left ventricle function:From theory to clinical practice[J]. Int J Cardiovasc Imaging,2018,34(8):1205-1213. [17] Cai Q,Wang J,Li H,Li C,Wu X,Lu X. Measurement of left ventricular volumes and ejection fraction in patients with regional wall motion abnormalities using an automated 3D quantification algorithm[J]. Ultrasound Med Biol,2018,44(11):2274-2282. [18] Sabour,Siamak. Automated measurement of left ventricular ejection fraction and volume using the Philips EPIQ system: Methodological issues on validity and reproducibility[J]. Echocardiography,2018,35(1):135. doi: 10.1111/echo.13781 [19] Menon D,Kadiu G,Sanil Y,et al. Anthracycline treatment and left atrial function in children:A real-time 3-dimensional echocardiographic study[J]. Pediatric Cardiology,2022,43(3):645-654. [20] Muraru A D,Ac A,Cucchini A U,et al. Intervendor consistency and accuracy of left ventricular volume measurements using three-dimensional echocardiography[J]. Journal of the American Society of Echocardiography,2018,31(2):158-168. doi: 10.1016/j.echo.2017.10.010 [21] Levy F,Iacuzio L,Schouver E D,et al. Performance of a new fully automated transthoracic three-dimensional echocardiographic software for quantification of left cardiac chamber size and function:Comparison with 3 Tesla cardiac magnetic resonance[J]. Journal of Clinical Ultrasound,2019,47(9):546-554. [22] Motoc A,Scheirlynck E,Roosens B,et al. Additional value of left atrium remodeling assessed by three-dimensional echocardiography for the prediction of atrial fibrillation recurrence after cryoballoon ablation[J]. The International Journal of Cardiovascular Imaging,2022,38(5):1103-1111. [23] Toader D M,Mirea O,Craciun-Mirescu A,et al. The link between left atrial longitudinal reservoir strain and mitral apparatus geometry in patients with dilated cardiomyopathy[J]. European Heart Journal,2022,43(2):26-29. [24] 滕花,任建丽,冉海涛,等. 三维超声心动图自动定量技术在评价左心腔容积及功能中的应用价值[J]. 中华超声影像学杂志,2019,28(3):192-199. doi: 10.3760/cma.j.issn.1004-4477.2019.03.002 -







 点击查看大图
点击查看大图
计量
- 文章访问数: 3073
- HTML全文浏览量: 2432
- PDF下载量: 37
- 被引次数: 0
