

The Effect of the Bone Window Dimension on the Outcomes of Maxillary Sinus Floor Elevation:Meta-Analysis
-
摘要:
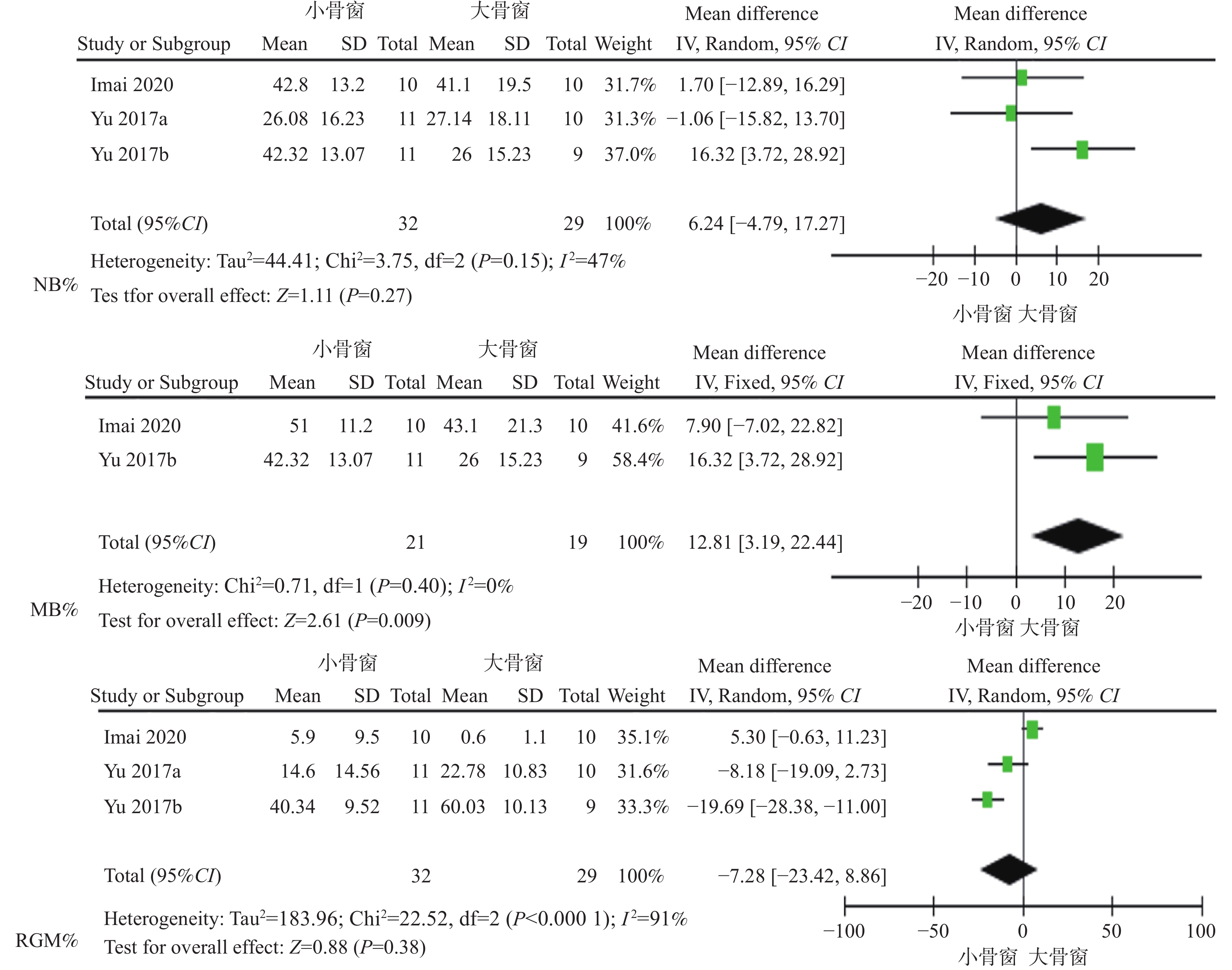
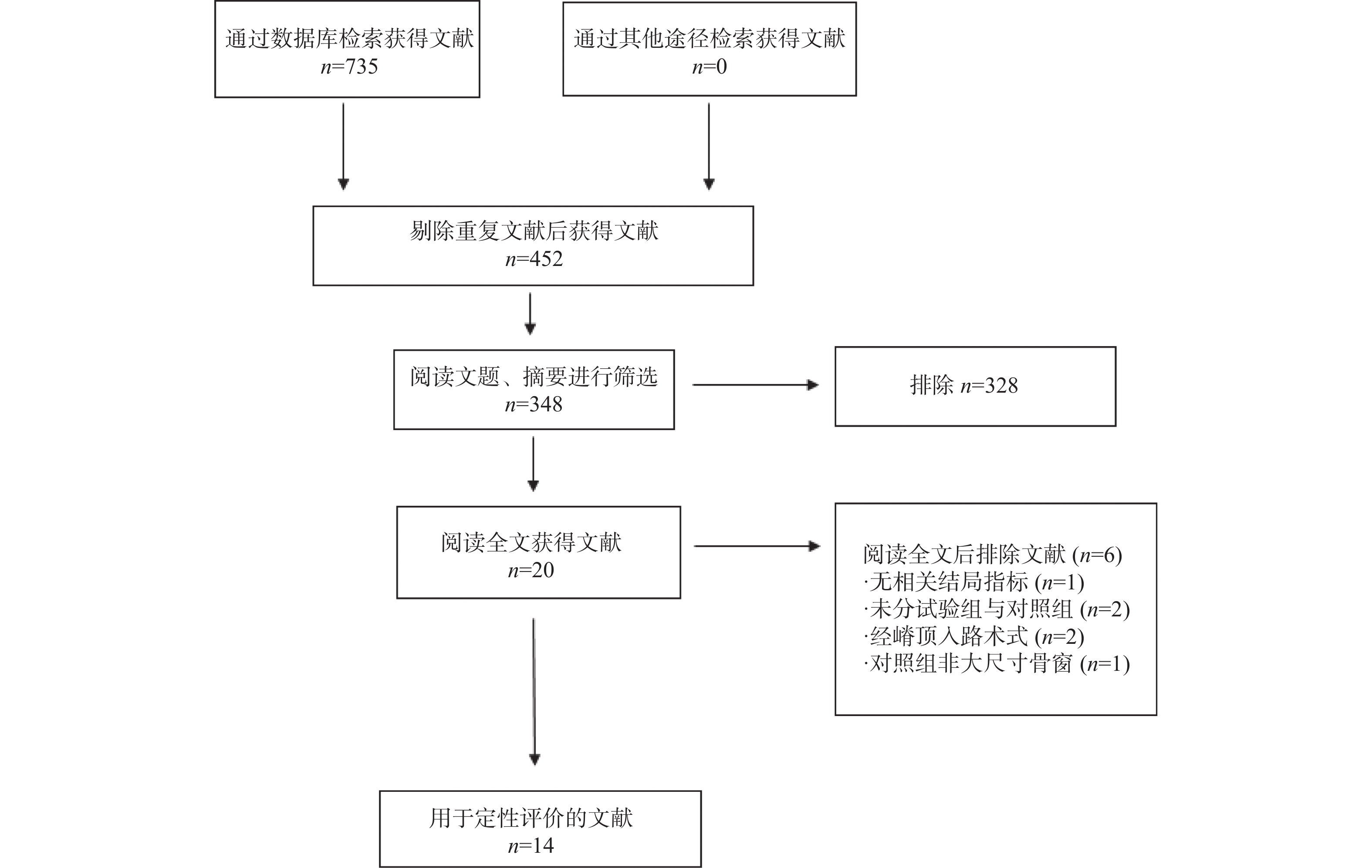
目的 上颌窦底提升术是增加上颌后牙垂直骨量的有效治疗方式,其成功与窦内新骨的形成密切相关。运用系统评价和Meta分析评估骨窗尺寸与上颌窦底提升术后治疗结果的相关性。 方法 电子检索Medline、Pubmed、Embase、Cochrane图书馆数据库、中国生物医学文献数据库(CBMdisc)和中国知识基础设施工程(CNKI),手动检索国家医学图书馆(NLM)。检索日期截止至2022年11月。检索要求包括经侧壁开窗式上颌窦底提升术分析骨窗尺寸与术后治疗结果的临床研究和动物研究,临床研究要求至少10例患者和6个月以上的随访期。3名研究者根据严格的纳入和排除标准独立纳入相关文献并提取数据进行偏倚风险评估,采用Revman 5.3软件进行Meta分析。 结果 经全文阅读后共纳入14篇文章进行系统评价。其中9篇为临床对照研究,6篇评估为低偏倚风险,2篇评估为中等偏倚风险,1篇为高偏倚风险。2种骨窗尺寸均能获得术后理想的上颌窦内骨再生和相似的生物学治疗结果。Meta分析结果显示,新骨矿化率与骨窗尺寸呈负相关性(P < 0.01)。新骨形成率和剩余骨移植材料率在小骨窗和大骨窗组差异无统计学意义(P > 0.05)。 结论 上颌窦内新骨矿化率与骨窗尺寸呈负相关,因此,经侧壁开窗式上颌窦底提升术中应尽量保存上颌窦侧壁,减小骨窗的制备,才能更大程度地获得窦内新骨的成熟和矿化。 Abstract:Objective Maxillary sinus floor elevation is an effective way to increase the vertical bone mass of maxillary posterior region, and its success is closely related to the formation of new bone. In this study, a systematic review and meta-analysis was used to evaluate the correlation between bone window dimension and postoperative outcomes after maxillary sinus floor elevation. Methods An electronic search strategy was performed on Medline, Pubmed, Embase, Cochrane Library database, Chinese Biology Medicine disc (CBMdisc), China National Knowledge Infrastructure (CNKI), and National Library of Medicine (NLM) up to November 2022. Clinical and animal studies that analyzed the effect of bone window dimension and postoperative outcomes using lateral window elevation were included. Clinical studies with at least ten patients, and a minimum follow-up period of 6 months were included. According to the inclusion and exclusion criteria, three evaluators independently screened related studies, extracted data, and evaluated risk bias. Meta-analysis was performed by Revman 5.3 software. Results A total of 14 studies were included for the systematic review after the full text reading. 6 studies with low risk of bias, 2 studies with moderate risk of bias and 1 study with high risk of bias were controlled clinical studies. Both of the two bone window dimensions achieved ideal maxillary sinus bone regeneration and similar biological outcomes. The Meta-analysis results showed that mineralized bone% was negatively correlated with the bone window dimension (P < 0.01). There was no significant difference in the new bone%, residual graft material% between the small bone window and the large bone window groups. Conclusion Negative correlation has been observed between the mineralized bone%and the dimension of bone window. Therefore, the lateral wall should be preserved as much as possible during the maxillary sinus floor elevation. Reducing the bone window has a positive effect on the maturity and mineralization of new bone. -

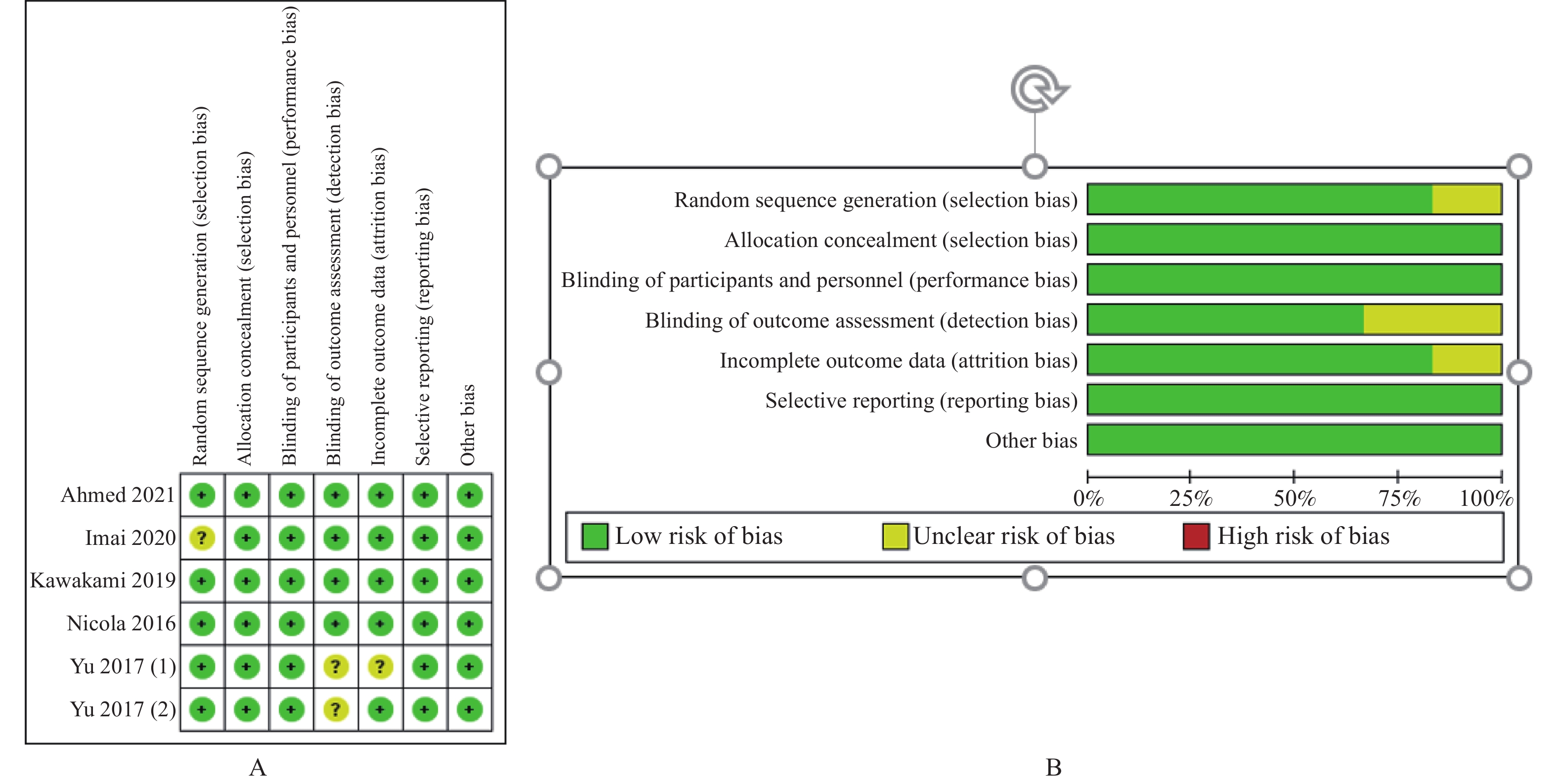
图 2 纳入研究中随机对照试验的偏倚风险评估
A:质量评价结果汇总点图;B:每项研究分析的偏倚风险。
Figure 2. Risk assessment of bias in randomized controlled trials
表 1 纳入文献特征表
Table 1. The characteristics of the articles
作者
发表年限研究
设计患者
(n)上颌窦
(n*)小骨窗(n*) 大骨窗(n*) 骨窗尺寸
(mm2)骨移植材料和
生物膜的类型种植体
植入时机愈合
时间结果测量方法 种植体存活率 生物学并发症 Yu
2017a随机对照试验 20 21 11 10 小骨窗:80.68 ± 6.17
大骨窗:114.31 ± 14.08Bio-Oss®: 100%
可吸收生物膜(大骨窗)
无生物膜覆盖(小骨窗)6个月后 6个月 组织形态学 NR 小骨窗:窦膜穿孔9.1%、
软组织塌陷18.2%
大骨窗:窦膜穿孔11.1%、
软组织塌陷44.4%Yu
2017b随机对照试验 19 20 11 9 小骨窗:81.65 ± 4.59
大骨窗:118.04 ± 19.53Bio-Oss®:90%
自体骨:10%
可吸收生物膜6个月后 6个月 组织形态学 小骨窗:100%
大骨窗:100%小骨窗:窦膜穿孔10%、
软组织塌陷18.2%
大骨窗:窦膜穿孔0%
软组织塌陷44.4%Imai
2020随机对照试验 20 20 10 10 小骨窗:49
大骨窗:98Osteobiol Gen-Os
可吸收生物膜6个月后 9个月 组织形态学 NR 窦膜穿孔:3例 Lu
2018队列研究 49 51 26 25 小骨窗:35.25 ± 9.19
大骨窗:47.49 ± 8.27Bio-Oss®: 100%
可吸收生物膜同期植入 6个月 CBCT 小骨窗:100%
大骨窗:94.28%小骨窗:窦膜穿孔7.69%
大骨窗:窦膜穿孔4%Nicola
2016随机对照试验 16 32 16 16 小骨窗:30.9 ± 4.4
大骨窗:73.7 ± 10.1Bio-Oss®: 100%
可吸收生物膜6个月后 6个月 CBCT NR 小骨窗:窦膜穿孔18.75%、
术中出血2例
大骨窗:窦膜穿孔25%Ahmed 2021 随机对照试验 20 30 15 15 小骨窗:20.88 ± 1.67
大骨窗:78.33 ± 3.67未植骨
可吸收生物膜同期植入 6个月 CBCT 小骨窗:100%
大骨窗:100%小骨窗:窦膜穿孔6.67%
大骨窗:窦膜穿孔6.67%Kawakami
2019随机对照试验 20 20 10 10 小骨窗:48.7 ± 14.7
大骨窗:98.3 ± 27.1Osteobiol Gen-Os
可吸收生物膜6个月后 9个月 CBCT NR 小骨窗:窦膜穿孔20%
大骨窗:窦膜穿孔20%牟永斌
2016队列研究 29 29 15 14 小骨窗:29.66 ± 5.2
大骨窗:141.2 ± 6.9Bio-Oss®: 100%
可吸收生物膜同期植入 6个月 CBCT 小骨窗:100%
大骨窗:100%小骨窗:窦膜穿孔0%
大骨窗:窦膜穿孔0%李文超
2020队列研究 30 30 15 15 小骨窗:31.69 ± 4.12
大骨窗:105.8 ± 9.34Bio-Oss®: 100%
可吸收生物膜同期植入 6个月 CBCT NR 小骨窗:窦膜穿孔6.67%
大骨窗:窦膜穿孔0%注:n指患者人数,n*代表行上颌窦提升术的窦腔数量。NR指未报道。  下载: 导出CSV
下载: 导出CSV
表 2 纳入研究中队列研究的偏倚风险评估
Table 2. Bias risk assessment of cohort studies
研究 研究对象
的代表性研究对象
的选择暴露因素的
测量方法研究开始前没有
研究对象发生
结局事件基于设计或分析
所得的队列的
可比性结局事件
的评估为观察到结局
发生,随访
是否充分随访的
完整性合计 Lu (2018) * * * * * * − 6 牟永斌(2016) * * * * − 4 李文超(2020) * * * * * − 5 *代表每个评估方面得1分,−代表每个评估方面无得分,总分为8分。
下载: 导出CSV
-
[1] Tatum H Jr. Maxillary and sinus implant reconstructions[J]. Dent Clin North Am,1986,30(2):207-229. doi: 10.1016/S0011-8532(22)02107-3 [2] Boyne P J,James R A. Grafting of the maxillary sinus floor with autogenous marrow and bone[J]. J Oral Surg,1980,38(8):613-616. [3] Zitzmann N U,Schärer P. Sinus elevation procedures in the resorbed posterior maxilla. Comparison of the crestal and lateral approaches[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod,1998,85(1):8-17. doi: 10.1016/S1079-2104(98)90391-2 [4] Van den Bergh J P,Ten Bruggenkate C M,Krekeler G,et al. Maxillary sinus floor elevation and grafting with human demineralized freeze dried bone[J]. Clin Oral Implants Res,2000,11(5):487-493. doi: 10.1034/j.1600-0501.2000.011005487.x [5] Schlegel K A,Zimmermann R,Thorwarth M,et al. Sinus floor elevation using autogenous bone or bone substitute combined with platelet-rich plasma[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod,2007,104(3):e15-e25. doi: 10.1016/j.tripleo.2007.04.021 [6] Testori T . Maxillary sinus surgery and alternatives in treatment[M]. Chicago: Quintessence Publishing USA, 2009: 194. [7] Vercellotti T,De Paoli S,Nevins M. The piezoelectric bony window osteotomy and sinus membrane elevation: Introduction of a new technique for simplification of the sinus augmentation procedure[J]. Int J Periodontics Restorative Dent,2001,21(6):561-567. [8] Cheon K J,Yang B E,Cho S W,et al. Lateral window design for maxillary sinus graft based on the implant position[J]. Int J Environ Res Public Health,2020,17(17):6335. doi: 10.3390/ijerph17176335 [9] Pariente L,Dada K,Daas M. Mini-lateral windows for minimally invasive maxillary sinus augmentation: Case series of a new technique[J]. Implant Dentistry,2014,23(4):371-377. [10] Imai H,Iezzi G,Piattelli A,et al. Influence of the dmensions of the antrostomy on osseointegration of mini-implants placed in the grafted region after sinus floor elevation: A randomized clinical trial[J]. Int J Oral Maxillofac Implants,2020,35(3):591-598. doi: 10.11607/jomi.8005 [11] Lu W,Xu J,Wang H M,et al. Influence of lateral windows with decreased vertical height following maxillary sinus floor augmentation: A 1-year clinical and radiographic study[J]. Int J Oral Maxillofac Implants,2018,33(3):661-670. doi: 10.11607/jomi.6213 [12] Barone A,Santini S,Marconcini S,et al. Osteotomy and membrane elevation during the maxillary sinus augmentation procedure. A comparative study: Piezoelectric device vs. conventional rotative instruments[J]. Clin Oral Implants Res,2008,19(5):511-515. doi: 10.1111/j.1600-0501.2007.01498.x [13] Avila-Ortiz G,Wang H L,Galindo-Moreno P,et al. Influence of lateral window dimensions on vital bone formation following maxillary sinus augmentation[J]. Int J Oral Maxillofac Implants,2012,27(5):1230-1238. [14] Aldahouk A , Elbeialy R R , Gibaly A , et al. The assessment of the effect of the size of lateral‐antrostomy in graftless balloon elevation of the maxillary sinus membrane with simultaneous implant placement (a randomized controlled clinical trial)[J]. Clinical Implant Dentistry and Related Research, 2021, 23(1): 31-42. [15] Baldini N,D'Elia C,Bianco A,et al. Lateral approach for sinus floor elevation: Large versus small bone window - a split-mouth randomized clinical trial[J]. Clin Oral Implants Res,2017,28(8):974-981. doi: 10.1111/clr.12908 [16] Yu H,He D,Qiu L. A prospective randomized controlled trial of the two-window technique without membrane versus the solo-window technique with membrane over the osteotomy window for maxillary sinus augmentation[J]. Clin Implant Dent Relat Res,2017,19(6):1099-1105. doi: 10.1111/cid.12547 [17] Page M J,Mckenzie J E,Bossuyt P M,et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews[J]. PLoS Medicine,2021,18(3):e1003583. doi: 10.1371/journal.pmed.1003583 [18] Higgins J P T,Altman D G,Gtzsche P C,et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials[J]. BMJ,2011,10(18):343. doi: 10.1136/bmj.d5928 [19] Wells G,Shea B,O'Connell D,et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of case-control studies in meta-analyses[J]. European Journal of Epidemiology,2011,1(25):603-605. [20] Yu H,Qiu L. A prospective randomized controlled trial of two-window versus solo-window technique by lateral sinus floor elevation in atrophic posterior maxilla: Results from a 1-year observational phase[J]. Clin Implant Dent Relat Res,2017,19(5):783-792. doi: 10.1111/cid.12505 [21] Kawakami S,Lang N P,Ferri M,et al. Influence of the height of the antrostomy in sinus floor elevation assessed by cone beam computed tomography - a randomized clinical trial[J]. Int J Oral Maxillofac Implants,2019,34(1):223-232. doi: 10.11607/jomi.7112 [22] 牟永斌,程然,吕昊昕,等. 改良小骨窗在上颌窦外提升术中的应用[J]. 江苏大学学报(医学版),2016,26(6):510-514. [23] 李文超,阮宁,李昊轩,等. 改良小开窗在低位上颌窦底外提升术中的应用[J]. 中国当代医药,2020,27(26):27. [24] Liqin Z,Jiakang Y,Jiaxing G,et al. Optimized beagle model for maxillary sinus floor augmentation via a mini-lateral window with simultaneous implant placement[J]. The Journal of international medical research,2018,46(11):4684-4692. [25] Zhu L,Yang J,Gong J,et al. Early bone formation in mini-lateral window sinus floor elevation with simultaneous implant placement: An in vivo experimental study[J]. Clin Oral Implants Res,2021,32(4):448-459. doi: 10.1111/clr.13714 [26] Scala A,Viña-Almunia J,Carda C,et al. Sequential healing of the elevated sinus floor with different size of antrostomy: A histomorphometric study in rabbits[J]. Oral Maxillofac Surg,2020,24(4):403-410. doi: 10.1007/s10006-020-00859-2 [27] Bornstein M M,Chappuis V,von Arx T,et al. Performance of dental implants after staged sinus floor elevation procedures: 5-year results of a prospective study in partially edentulous patients[J]. Clin Oral Implants Res,2008,19(10):1034-1043. doi: 10.1111/j.1600-0501.2008.01573.x [28] Lundgren S,Cricchio G,Hallman M,et al. Sinus floor elevation procedures to enable implant placement and integration: Techniques,biological aspects and clinical outcomes[J]. Periodontol,2016,73(1):103-120. [29] Danesh-Sani S A,Loomer P M,Wallace S S. A comprehensive clinical review of maxillary sinus floor elevation: Anatomy,techniques,biomaterials and complications[J]. Br J Oral Maxillofac Surg,2016,54(7):724-730. doi: 10.1016/j.bjoms.2016.05.008 [30] Galindo-Moreno P,Hernández-Cortés P,Mesa F,et al. Slow resorption of anorganic bovine bone by osteoclasts in maxillary sinus augmentation[J]. Clin Implant Dent Relat Res,2013,15(6):858-866. doi: 10.1111/j.1708-8208.2012.00445.x [31] Haas R,Baron M,Donath K,et al. Porous hydroxyapatite for grafting the maxillary sinus: A comparative histomorphometric study in sheep[J]. Int J Oral Maxillofac Implants,2002,17(3):337-346. [32] Scala A,Botticelli D,Rangel IG Jr,et al. Early healing after elevation of the maxillary sinus floor applying a lateral access: A histological study in monkeys[J]. Clin Oral Implants Res,2010,21(12):1320-1326. doi: 10.1111/j.1600-0501.2010.01964.x [33] Miyamoto S,Shinmyouzu K,Miyamoto I,et al. Histomorphometric and immunohistochemical analysis of human maxillary sinus-floor augmentation using porous β-tricalcium phosphate for dental implant treatment[J]. Clin Oral Implants Res,2013,24(Suppl A100):134-138. [34] Scala A,Botticelli D,Faeda R S,et al. Lack of influence of the Schneiderian membrane in forming new bone apical to implants simultaneously installed with sinus floor elevation: An experimental study in monkeys[J]. Clin Oral Implants Res,2012,23(2):175-181. doi: 10.1111/j.1600-0501.2011.02227.x [35] Zaffe D,D'Avenia F. A novel bone scraper for intraoral harvesting: A device for filling small bone defects[J]. Clin Oral Implants Res,2007,18(4):525-533. doi: 10.1111/j.1600-0501.2007.01368.x [36] Stacchi C,Spinato S,Lombardi T,et al. Minimally invasive management of implant-supported rehabilitation in the posterior maxilla,part I. sinus floor elevation: Biologic principles and materials[J]. Int J Periodontics Restorative Dent,2020,40(3):e85-e93. doi: 10.11607/prd.4497 [37] Wang H L,Boyapati L. "PASS" principles for predictable bone regeneration[J]. Implant Dent,2006,15(1):8-17. doi: 10.1097/01.id.0000204762.39826.0f [38] Simonpieri A,Choukroun J,Del Corso M,et al. Simultaneous sinus-lift and implantation using microthreaded implants and leukocyte- and platelet-rich fibrin as sole grafting material: A six-year experience[J]. Implant Dent,2011,20(1):2-12. doi: 10.1097/ID.0b013e3181faa8af [39] Scarano A,de Oliveira P S,Traini T,et al. Sinus membrane elevation with heterologous cortical lamina: A randomized study of a new surgical technique for maxillary sinus floor augmentation without bone graft[J]. Materials (Basel),2018,11(8):1457. doi: 10.3390/ma11081457 [40] Menassa G,Kassir A R,Landi L,et al. Implant placement with graftless sinus floor elevation via the lateral approach: A case series with 4 years post-loading radiographical outcomes and implant survival rate[J]. J Craniofac Surg,2022,33(5):e461-e465. doi: 10.1097/SCS.0000000000008356 [41] Menassa G,Kassir A R,Landi L,et al. Implant placement with sinus floor elevation via the lateral approach using only absorbable collagen sponge: 12-month post-loading radiographical outcomes and implant survival rate[J]. Oral Maxillofac Surg,2021,25(2):231-236. doi: 10.1007/s10006-020-00908-w [42] Schmitz J P,Hollinger J O. The critical size defect as an experimental model for craniomandibulofacial nonunions[J]. Clin Orthop Relat Res,1986,4(205):299-308. -

 点击查看大图
点击查看大图
图(3) / 表(2)
计量
- 文章访问数: 1951
- HTML全文浏览量: 814
- PDF下载量: 23
- 被引次数: 0
