

Network Meta-Analysis of Three Different Interventional Methods for the Treatment of Tracheobronchial Tuberculosis
-
摘要:
目的 系统评价不同支气管镜下介入方法联合常规抗结核方案治疗气管支气管结核(TBTB)的疗效与安全性,为临床提供循证参考。 方法 计算机检索PubMed、Web of Science、EMBase、中国知网(CNKI)、万方数据库(Wanfang)、维普数据库(VIP),收集不同支气管镜下介入方法(局部给药、冷冻治疗和雾化治疗)联合常规抗结核治疗的随机对照试验(RCT),提取数据资料并进行质量评价后,利用软件Stata 16.0进行网状Meta分析。 结果 共纳入38项RCT,共计3114名患者,涉及常规+局药、常规+冷冻、常规+局药+雾化等3种干预措施。与常规治疗比较,常规+冷冻、常规+局药、常规+局药+雾化均可显著缓解临床症状,提高有效率(P < 0.05),网状Meta排序结果为:常规+局药+雾化 > 常规+局药 > 常规+冷冻 > 常规;纤维支气管镜下,与常规治疗比较,常规+冷冻、常规+局药、常规+局药+雾化均可显著提高治疗有效率(P < 0.05),网状Meta排序结果为:常规+局药 > 常规+局药+雾化 > 常规+冷冻>常规;与常规治疗比较,常规+局药、常规+局药+雾化均可显著提高患者治疗后8周末痰菌转阴率(P < 0.05);与常规+冷冻相比,常规+局药可显著提高患者治疗后8周末痰菌转阴率(P < 0.05)。网状Meta排序结果为:常规+局药 > 常规+局药+雾化 > 常规+冷冻>常规;与常规治疗比较,常规+局药可显著提高患者治疗后24周末痰菌转阴率(P < 0.05),网状Meta排序结果为常规+局药 > 常规+局药+雾化 > 常规+冷冻>常规;在不良反应发生率方面,各组组间比较,差异均无统计学意义(P > 0.05)。 结论 常规+局药+雾化方案提高疗效最为显著,而常规+局药方案在纤维支气管镜下治疗有效率方面效果最佳;TBTB患者早期应用常规+局药+雾化方案可加速痰菌转阴,但在长期治疗中应用常规+局药方案痰菌转阴效果更佳;在常规抗结核基础上联用支气管镜下介入治疗不会增加不良反应,安全性良好。但研究有待纳入更多高质量、双盲RCT进一步验证。 Abstract:Objective To systematically evaluate the efficacy and safety of different bronchoscopic intervention methods combined with the conventional anti-tuberculosis regimen in the treatment of tracheobronchial tuberculosis (TBTB), and to provide the evidence-based reference for clinical practice. Methods Computer search PubMed, Web of Science, EMBase, CNKI, Wanfang Database, VIP database, randomized controlled trials (RCTS) of different bronchoscopic interventions (local administration, cryotherapy, and atomization) combined with conventional anti-tuberculosis therapy were collected. After the data extraction and quality evaluation, network meta-analysis was performed using Stata 16.0 software. Results A total of 38 RCTS were included, involving a total of 3114 patients and three interventions (conventional + local administration, conventional+ cryotherapy, conventional + local administration + atomization). Compared with the conventional treatment, conventional+ cryotherapy, conventional + local administration, conventional + local administration + atomization could significantly improve the total clinical response rate (P < 0.05). The results of mesh Meta ranking were conventional + local administration + atomization > conventional + local administration > conventional + cryotherapy > conventional. Compared with the conventional treatment, conventional + cryotherapy, conventional + local administration, conventional + local administration + atomization could significantly improve the effective rate of fiberoptic bronchoscopy (P < 0.05). The results of mesh Meta ranking were conventional + local administration > conventional + local administration + atomization > conventional + cryotherapy > conventional. Compared with the conventional treatment, conventional + local administration, conventional + local administration + atomization could significantly improve the sputum negative conversion rate at the end of 8 weeks after the treatment (P < 0.05). Compared with conventional + cryotherapy, conventional + local administration could significantly improve the sputum negative conversion rate at the end of 8 weeks after treatment (P < 0.05). The results of mesh Meta ranking were conventional + local administration > conventional + local administration + atomization > conventional + cryotherapy > conventional. Compared with the conventional treatment, conventional + local administration could significantly improve the sputum negative conversion rate at the end of 24 weeks after treatment (P < 0.05). The results of mesh Meta ranking were conventional + local administration > conventional + local administration + atomization > conventional + cryotherapy > conventional. There was no statistically significant difference in the incidence of adverse reactions among all groups (P > 0.05). Conclusion The conventional + local administration + atomization scheme has the most significant improvement effect, while the conventional + local administration scheme has the best effect in improving the effective rate under bronchoscopy. In TBTB patients, the conventional + local administration + atomization regimen can accelerate the sputum to negative in the early stage, but the conventional + local administration regimen can accelerate the conversion of sputum to negative in the long-term treatment. Bronchoscopic intervention on the basis of conventional anti-tuberculosis therapy does not increase adverse reactions and has the good safety. However, this study needs to be further verified by including more high-quality, double-blind RCTS. -

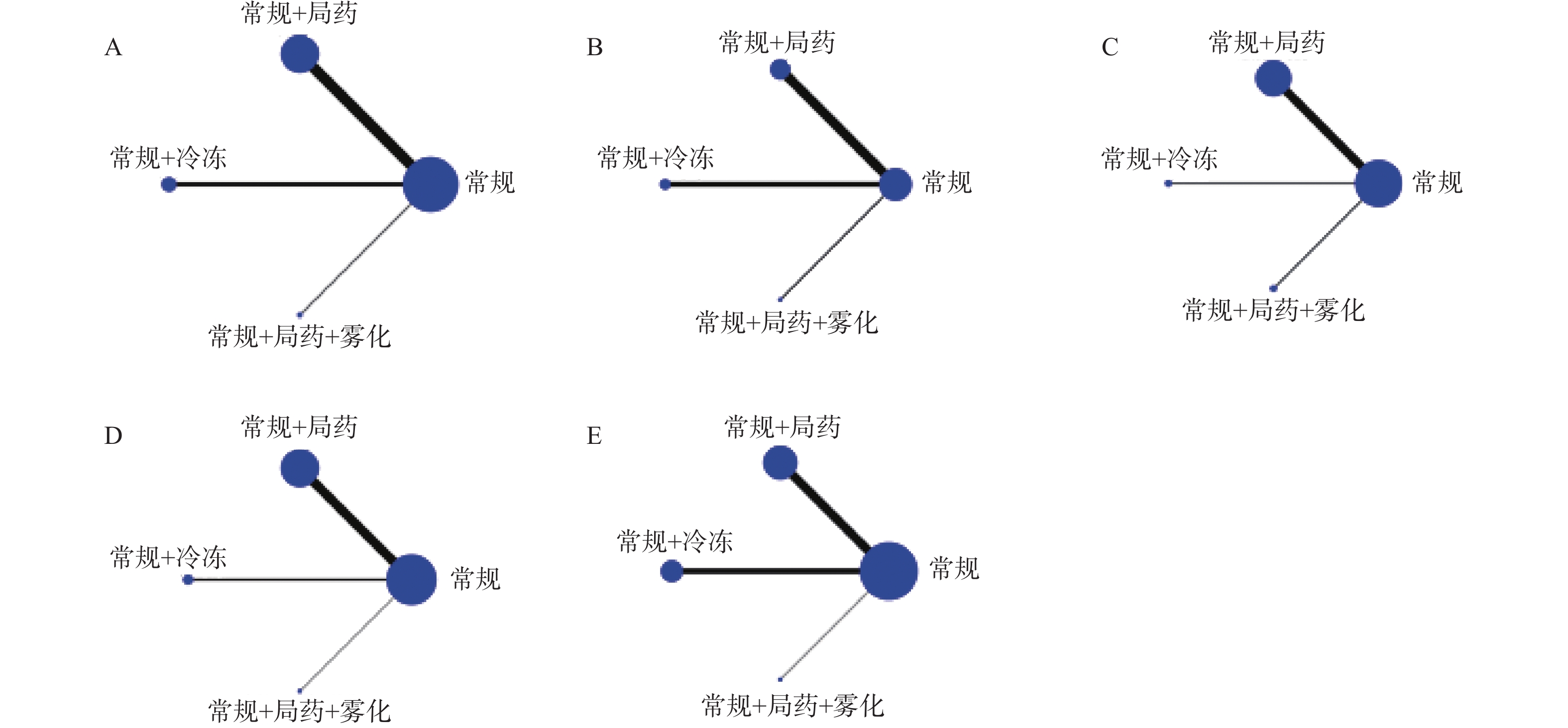
图 3 证据关系图
A:临床症状有效率纳入研究证据关系;B:纤维支气管镜下有效率纳入研究证据关系;C:治疗后8周末痰菌转阴率纳入研究证据关系;D:治疗后24周末痰菌转阴率纳入研究证据关系;E:治疗后不良反应发生率纳入研究证据关系。
Figure 3. Evidence diagram
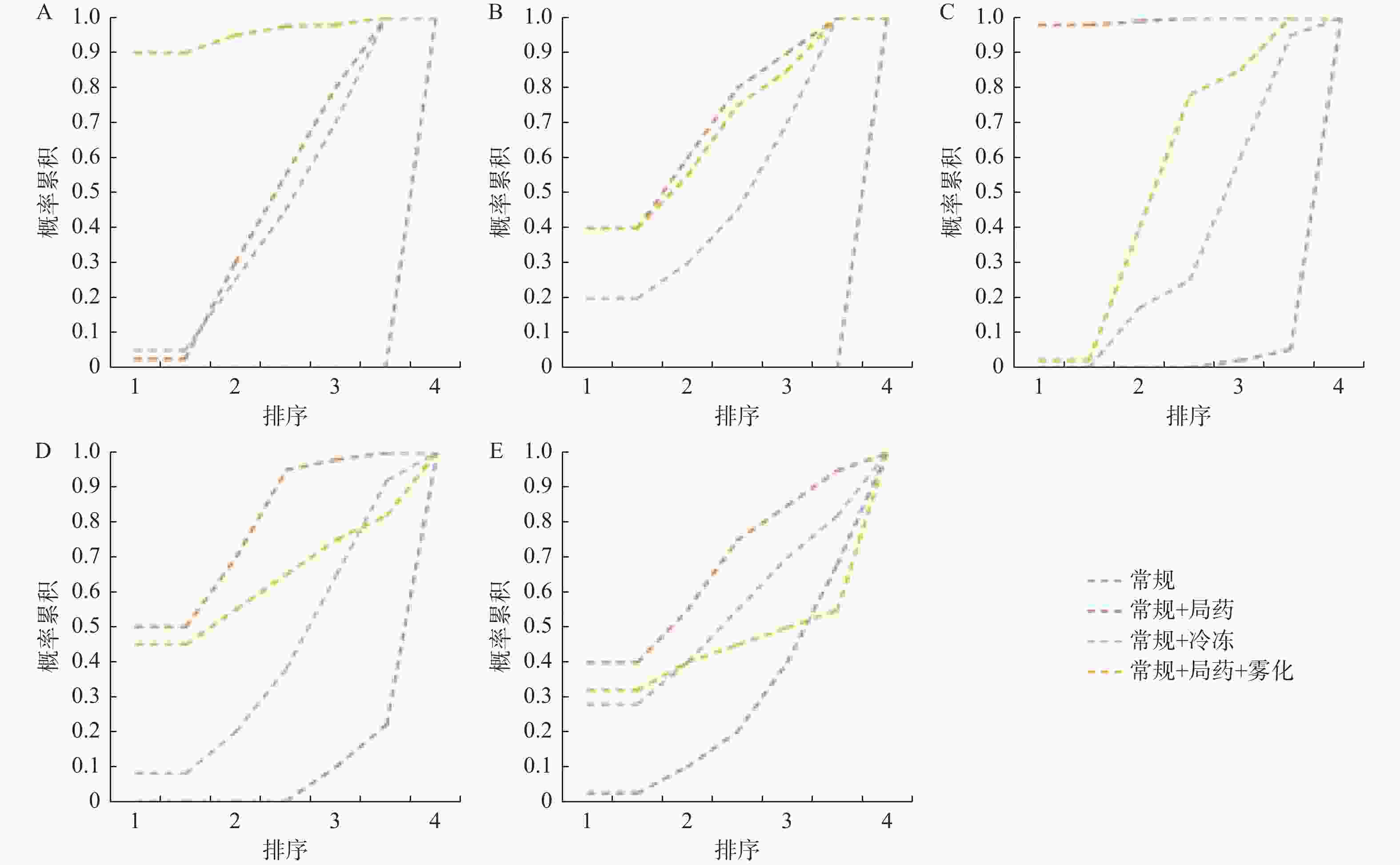
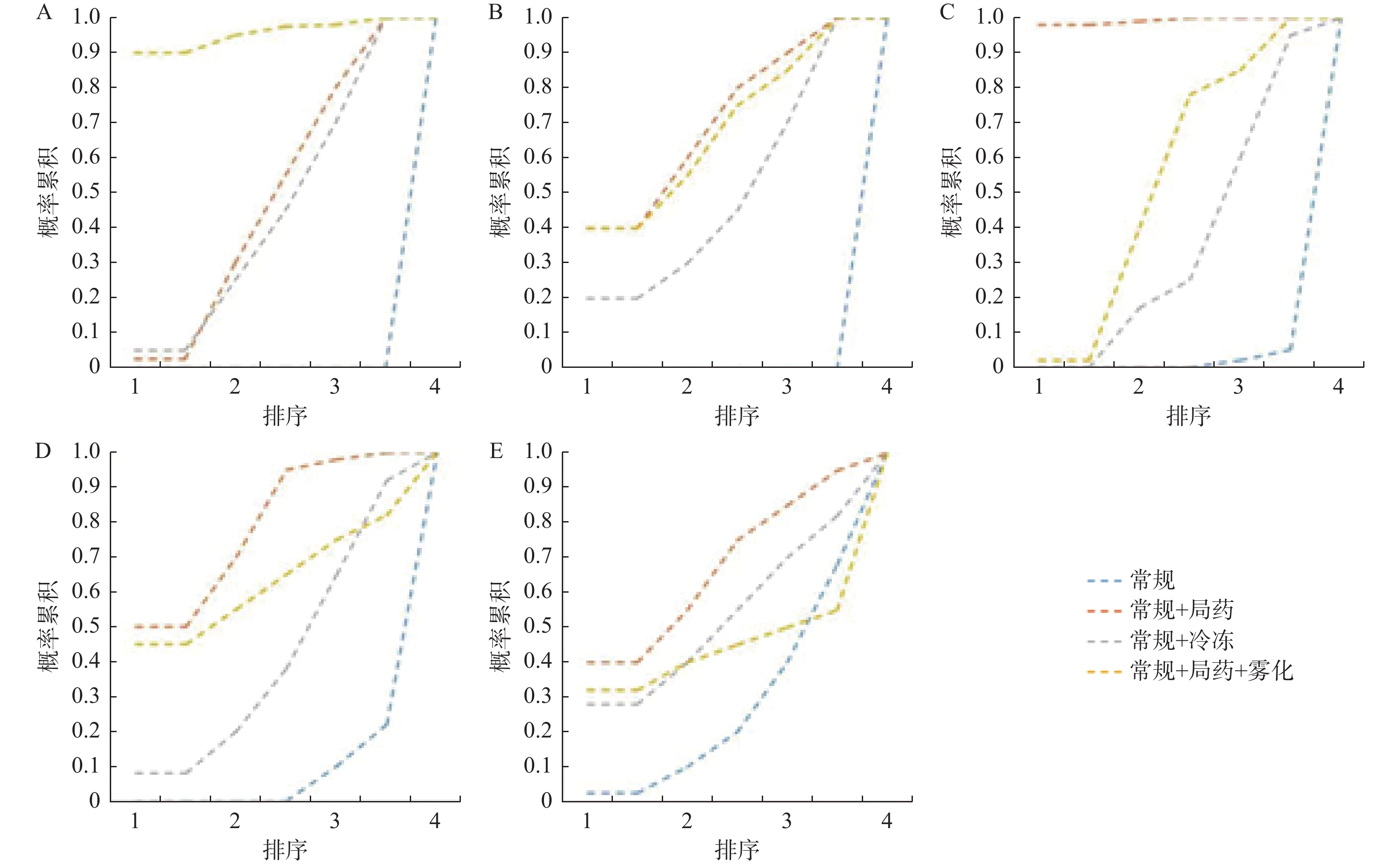
图 4 累积概率排序图
A:临床症状有效率的累积概率排序图;B:纤维支气管镜下有效率的累积概率排序图;C:治疗后8周末痰菌转阴率的累积概率排序图;D:治疗后24周末痰菌转阴率的累积概率排序图;E:不良反应发生率的累积概率排序图。
Figure 4. Cumulative probability ranking chart

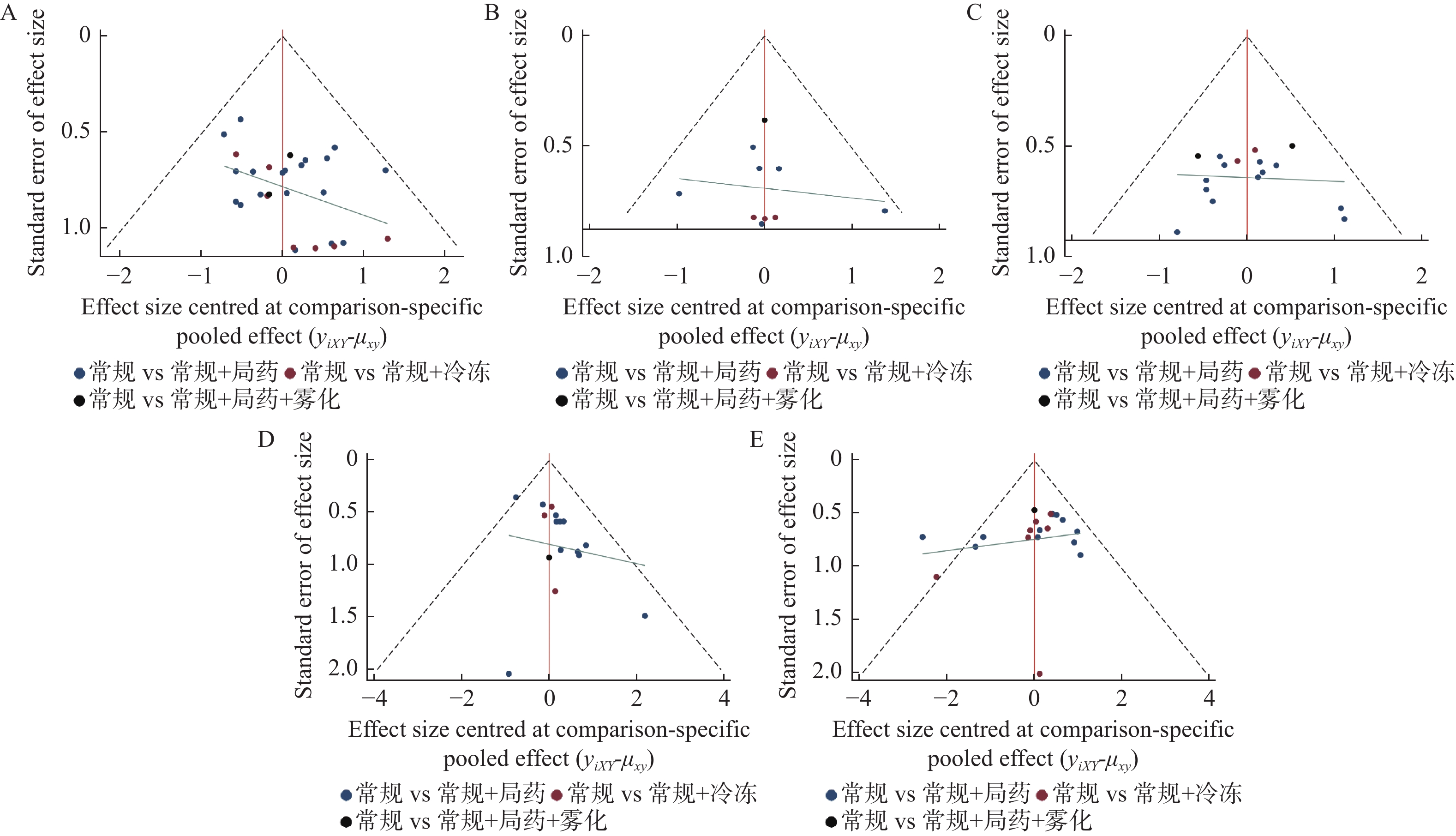
图 5 发表偏倚分析图
A:临床治疗总有效率的倒漏斗图;B:纤维支气管镜下治疗有效率的倒漏斗图;C:治疗后8周末痰菌转阴率的倒漏斗图;D:治疗后24周末痰菌转阴率的倒漏斗图;E:治疗后不良反应发生率的倒漏斗图。
Figure 5. Published bias analysis chart
表 1 纳入研究基本信息[(
$\bar x \pm s $ )/n(%)]Table 1. Includes basic research information [(
$\bar x \pm s $ )/n(%)]文献来源 例数 年龄/岁 干预措施 结局指标 试验组/对照组 试验组/对照组 试验组/对照组 田江华2014[4] 31/31 35.6 ± 13.1/36.0 ± 13.0 常规+局药/常规2HRZE/10HR ①④ 高鸿2021[5] 45/45 46.63 ± 3.82/46.52 ± 3.74 常规+局药/常规2HRZE/10HRE ①③ 张新宝2015[6] 36/36 17~71 常规+局药/常规3HRZE/9HRE ①③④⑤ 张德利2019[7] 34/34 - 常规+局药/常规3HRZE/9HR ①④ 崔金霞2021[8] 40/40 36.75 ± 5.28/37.43 ± 5.56 常规+局药/常规2HRZE/10HR ①⑤ 符少平2009[9] 85/35 29 ± 1.12/31 ± 1.26 常规+局药/常规2HRZE/4HR ②④ 肖斌2020[10] 39/39 43.15 ± 1.35/43.62 ± 1.32 常规+局药/常规HRZE ①⑤ 潘丽2013[11] 34/33 37.85 ± 7.12/38.63 ± 7.34 常规+局药/常规2HRZE(S)/10HR ③⑤ 郑飞2013[12] 23/23 50 ± 11/49 ± 11 常规+局药/常规2HRZE(S)/6HRE ①② 刘宗道2002[13] 26/26 36.8 ± 11.2/37.1 ± 10.9 常规+局药/常规2HRZE/4HR ④⑤ 韩彩丽2013[14] 62/58 33.5 ± 6.7/32.8 ± 6.2 常规+局药/常规3HRZE(S)/9HRE ①② 叶涛生2018[15] 32/32 52.38 ± 13.71/52.35 ± 13.68 常规+局药/常规HRZELfx ①③④ 孙明华2017[16] 48/47 47.6 ± 3.8/48.2 ± 3.4 常规+局药/常规2HRZE/10HRE ①③ 陈廷宪2021[17] 41/41 28.75 ± 3.62/28.65 ± 3.59 常规+局药/常规2HRZE/10HRE ①③④ 胡翠兰2015[18] 38/37 37.4 ± 8.2/38.2 ± 8.7 常规+局药/常规2HRZS/4HR ①② 陈艳2009[19] 52/41 20~76 常规+局药/常规2HRZE(S)/10HR ④⑤ 王枝梅2012[20] 36/36 18~61 常规+局药/常规 ①③ 张胜堂2020[21] 48/46 35.81 ± 12.46/36.37 ± 13.15 常规+局药/常规2HRZS/10HRE ⑤ 朱红涛2020[22] 41/41 46.48 ± 12.34/47.03 ± 11.57 常规+局药/常规2HRZS/4HR ③ 杨新建2021[23] 30/30 43.30 ± 3.41/42.40 ± 2.11 常规+局药/常规2HRZE/4HR ①③⑤ 张含琼2016[24] 44/41 38.2 ± 10.1/42.9 ± 13.2 常规+局药/常规2HRZE/10HRE ③⑤ 张廷梅2008[25] 35/18 16~61/6~51 常规+局药/常规HRZE(S) ①④⑤ 刘斌远2012[26] 47/46 18~65/17~67 常规+局药/常规3HRZE/9HRE ①②④ 李史来2013[27] 34/34 18~61 常规+局药/常规2HRZE(S)/10HRE ①②④ 庄辉2019[28] 35/35 44.31 ± 8.69/43.63 ± 9.81 常规+局药/常规2HRZE/10HRE ⑤ 付娟2017[29] 73/73 - 常规+局药/常规4HRZE/8HR ①⑤ 程耀强2021[30] 30/30 48.96 ± 8.02/49.25 ± 9.42 常规+局药/常规HRZE ①③④ 如克亚木2020[31] 48/48 40.06 ± 3.66/39.65 ± 3.26 常规+冷冻/常规2HRZE/10HRE ①③ 刘荣奎2016[32] 51/50 46.58 ± 4.52/45.62 ± 4.48 常规+冷冻/常规2HRZE/10HR ①③ 蒋凛2019[33] 35/35 43.12 ± 4.03/42.36 ± 4.21 常规+冷冻/常规3HR ①③ 王志刚2019[34] 33/31 43.12 ± 16.82/44.03 ± 15.52 常规+冷冻/常规3HRZE/9HRE ①②③④⑤ 王莉2013[35] 39/31 30.52 ± 12.75 常规+冷冻/常规HRZE ②④ 姜心成2018[36] 30/30 47.5 ± 10.5/48.5 ± 11.5 常规+冷冻/常规HRE ①③⑤ 刘明2018[37] 34/34 31.29 ± 12.93/32.49 ± 12.87 常规+冷冻/常规 ② 于丹2016[38] 46/46 48.1 ± 4.3/47.5 ± 5.3 常规+冷冻/常规2HRZE/4HR ①③⑤ 黄自强2021[39] 30/30 45.20 ± 13.14/45.25 ± 12.56 常规+冷冻/常规2HRZE/10HRE ①③ 陆兰英2010[40] 116/112 18~71/16~70 常规+局药+雾化/常规2HRZE(S)/6HRE ①②③④ 谭红玉2014[41] 30/28 20~60/16~58 常规+局药+雾化/常规 ①④⑤ 注:H:异烟肼;R:利福平;Z:吡嗪酰胺;E:乙胺丁醇;S:链霉素;Lfx:左氧氟沙星,全文其他地方同。①:临床症状治疗有效率;②:纤维支气管镜下有效率;③:治疗后不良反应发生率;④:治疗后8周末痰菌转阴率;⑤:治疗后24周末痰菌转阴率。  下载: 导出CSV
下载: 导出CSV
表 2 2组患者临床症状有效率的网状Meta分析结果
Table 2. Results of reticular meta analysis of effective treatment of clinical symptoms in two groups of patients
组别 OR(95%CI) OR(95%CI) OR(95%CI) 常规+冷冻 1.05 (0.52,2.13) 0.17 (0.09,0.32) 2.43 (0.76,7.74) 0.95 (0.47,1.93) 常规+局药 0.16 (0.12,0.22) 2.31(0.83,6.41) 5.90 (3.13,11.10) 6.20 (4.53,8.49) 常规 14.32 (5.42,37.85) 0.41 (0.13,1.31) 0.43 (0.16,1.20) 0.07 (0.03,0.18) 常规+局药+雾化
下载: 导出CSV
表 3 2组患者纤维支气管镜下治疗有效率的网状Meta分析结果
Table 3. Results of reticular meta analysis of the efficacy of fiberoptic bronchoscopy in two groups of patients
组别 OR(95%CI) OR(95%CI) OR(95%CI) 常规+冷冻 1.32 (0.45,3.82) 0.13 (0.05,0.34) 1.31 (0.40,4.31) 0.76 (0.26,2.20) 常规+局药 0.10 (0.06,0.17) 0.99 (0.40,2.46) 7.55 (2.98,19.15) 9.94 (5.94,16.65) 常规 9.87 (4.68,20.83) 0.76 (0.23,2.52) 1.01 (0.41,2.50) 0.10 (0.05,0.21) 常规+局药+雾化
下载: 导出CSV
表 4 2组患者治疗后8周末痰菌转阴率的网状Meta分析结果
Table 4. Results of reticular meta analysis of negative probability of sputum culture in two groups at the end of 8 weeks of treatment
组别 OR(95%CI) OR(95%CI) OR(95%CI) 常规+冷冻 3.10 (1.34,7.14) 0.52 (0.25,1.11) 1.41 (0.50,3.98) 0.32 (0.14,0.74) 常规+局药 0.17 (0.12,0.24) 0.45 (0.20,1.02) 1.91 (0.90,4.04) 5.92 (4.09,8.59) 常规 2.70 (1.31,5.54) 0.71 (0.25,2.00) 2.20 (0.98,4.94) 0.37 (0.18,0.76) 常规+局药+雾化
下载: 导出CSV
表 5 2组患者治疗后24周末痰菌转阴率的网状Meta分析结果
Table 5. Results of reticular meta analysis of negative probability of sputum culture in two groups at the end of 24 weeks of treatment
组别 OR(95%CI) OR(95%CI) OR(95%CI) 常规+冷冻 1.69 (0.75,3.81) 0.59 (0.30,1.19) 1.49 (0.20,10.87) 0.59 (0.26,1.33) 常规+局药 0.35 (0.23,0.53) 0.88 (0.13,5.93) 1.68 (0.84,3.38) 2.85 (1.88,4.32) 常规 2.50 (0.39,16.13) 0.67 (0.09,4.92) 1.14 (0.17,7.70) 0.40 (0.06,2.58) 常规+局药+雾化
下载: 导出CSV
表 6 2组患者治疗后不良反应发生率的网状Meta分析结果
Table 6. Results of reticular meta analysis of the incidence of adverse reactions in two groups of patients after treatment
组别 OR(95%CI) OR(95%CI) OR(95%CI) 常规+冷冻 0.89 (0.35,2.27) 1.24 (0.59,2.61) 1.19 (0.21,6.86) 1.12 (0.44,2.83) 常规+局药 1.38 (0.79,2.42) 1.33 (0.25,7.14) 0.81 (0.38,1.71) 0.72 (0.41,1.26) 常规 0.96 (0.20,4.68) 0.84 (0.15,4.84) 0.75 (0.14,4.02) 1.04 (0.21,5.06) 常规+局药+雾化
下载: 导出CSV
-
[1] 中华医学会结核病学分会,《中华结核和呼吸杂志》编辑委员会. 气管支气管结核诊断和治疗指南(试行)[J]. 中华结核和呼吸杂志,2012,35(8):581-587. [2] 李莹,曹益瑞,陶红竹,等. 气管支气管结核的局部药物治疗进展[J]. 中国防痨杂志,2021,43(10):1096-1101. [3] Ding H,Hu G L,Zheng X Y,et al. The method quality of cross-over studies involved in cochrane systematic reviews[J]. PLoS One,2015,10(4):e0120519. doi: 10.1371/journal.pone.0120519 [4] 田江华,戴元荣,颜孙舜,等. 经支气管镜局部药物灌注治疗气管支气管结核的临床研究[J]. 中国防痨杂志,2014,36(6):494-497. [5] 高鸿,赵金辅. 支气管镜下局部用药法联合常规抗结核疗法治疗气管支气管结核的疗效[J]. 当代医药论丛,2021,19(11):80-81. [6] 张新宝,周瑛,张毕玲. 支气管镜注入治疗支气管结核72例临床疗效分析[J]. 临床肺科杂志,2015,20(11):1960-1962. [7] 张德利,张彦. 支气管镜下局部治疗支气管结核临床分析[J]. 临床医药文献电子杂志,2019,6(77):81. [8] 崔金霞. 纤维支气管镜给药治疗支气管结核的临床研究[J]. 大健康,2021,8(3):131-132. [9] 符少平,邱晨,孔焱. 非瘢痕狭窄型支气管内膜结核局部治疗的疗效观察[J]. 山东医药,2009,49(17):91-92. [10] 肖斌. 经电子支气管镜局部注药治疗支气管结核的近远期疗效对照分析[J]. 影像研究与医学应用,2020,4(17):165-166. [11] 潘丽. 经纤维支气管镜局部化疗治疗气管支气管结核的疗效[J]. 中外医学研究,2013,11(34):48-49. [12] 郑飞. 经纤维支气管镜局部注药治疗支气管结核的疗效观察[J]. 河北医药,2013,35(23):3556-3557. [13] 刘宗道,敬军. 经纤维支气管镜治疗痰菌阳性的支气管内膜结核的疗效分析[J]. 中国内镜杂志,2002,8(7):21-22. [14] 韩彩丽. 经纤维支气管镜注药治疗气管及支气管结核的临床疗效观察[J]. 内蒙古医学杂志,2013,45(7):799-800. [15] 叶涛生,张培泽,曾旋,等. 经支气管镜治疗淋巴结瘘型支气管结核的效果分析[J]. 新发传染病电子杂志,2018,3(4):202-205. [16] 孙明华. 局部给药治疗支气管结核的临床疗效[J]. 临床肺科杂志,2017,22(9):1716-1718,1721. [17] 陈廷宪,黄祖军,冯晓红. 抗结核联合电子支气管镜治疗支气管结核患者的效果及安全性分析[J]. 中国当代医药,2021,28(22):62-65. [18] 胡翠兰,刘纯钢,袁艳梅. 联合治疗支气管结核的疗效观察[J]. 临床肺科杂志,2015,20(2):363-364. [19] 陈艳,王波,蒲青,等. 纤维支气管镜局部治疗支气管内膜结核的疗效观察[J]. 西部医学,2009,21(9):1480-1481. [20] 王枝梅. 纤维支气管镜下局部给药治疗支气管结核疗效观察[J]. 中国实用医药,2012,7(35):89-90. [21] 张胜堂,唐炳俭,张晓伟,等. 纤维支气管镜下局部注射治疗支气管内膜结核的临床疗效观察[J]. 当代医学,2020,26(25):31-33. [22] 朱红涛. 纤支镜局部注射药物联合2HRSZ/4HR方案治疗支气管结核的短期随访研究[J]. 实用医药杂志,2020,37(6):510-512. doi: 10.14172/j.issn1671-4008.2020.06.009 [23] 杨新建. 纤支镜气管内注入异烟肼联合利福平治疗支气管结核的临床观察[J]. 世界最新医学信息文摘,2021,21(85):129-130. [24] 张含琼,李强. 异烟肼治疗气管支气管结核的临床疗效与安全性观察[J]. 检验医学与临床,2016,13(12):1656-1658. [25] 张廷梅,熊敏,吴鉴文,等. 支气管结核单纯化疗和介入综合治疗近期效果观察[J]. 中国防痨杂志,2008,30(3):206-209. [26] 刘斌远,史海霞,吕广波,等. 支气管结核经纤维支气管镜介入治疗与单纯全身化疗对比研究[J]. 河北医药,2012,34(6):852-853. [27] 李史来,黄智祥,林少云,等. 支气管镜辅助治疗支气管内膜结核的观察[J]. 中国热带医学,2013,13(12):1535-1537. [28] 庄辉,丁园国,藏千静,等. 支气管镜局部注射化疗在支气管结核患者治疗中的应用价值[J]. 中国社区医师,2019,35(13):105. [29] 付娟. 支气管镜下局部灌药联合全身化疗治疗支气管结核的疗效及应用[J]. 黑龙江医学,2017,41(7):649-651. [30] 程耀强,陀子能. 支气管镜下局部治疗联合全身抗结核治疗支气管结核疗效分析[J]. 中国实用医药,2021,16(26):28-31. [31] 如克亚木·阿不都沙拉木,古力米热·依明,麦不班姆·依不拉依木,等. 电子支气管镜下冷冻结合抗结核药物治疗支气管结核的效果[J]. 临床医学研究与实践,2020,5(3):51-52. [32] 刘荣奎. 电子支气管镜下冷冻治疗支气管结核的疗效及安全性分析[J]. 中国医疗器械信息,2016,22(6):63-64. [33] 蒋凛. 经支气管镜冷冻治疗支气管结核疗效分析[J]. 江西医药,2019,54(5):503-504,507. [34] 王志刚,刘媛媛. 经纤维支气管镜介入冷冻联合其他方法治疗气管支气管结核的疗效及不良反应分析[J]. 中国防痨杂志,2019,41(5):569-574. [35] 王莉,徐爱晖. 经纤支镜介入冷冻治疗支气管结核的疗效分析[J]. 临床肺科杂志,2013,18(8):1450-1452. [36] 姜心成. 经支气管镜介入冷冻治疗支气管结核的临床效果观察[J]. 中国实用医药,2018,13(2):32-33. [37] 刘明,马英莲,魏国月,等. 支气管结核患者经纤支镜介入冷冻治疗的疗效分析[J]. 河北医学,2018,24(12):2051-2054. [38] 于丹. 支气管镜介入冷冻治疗支气管结核临床研究[J]. 中国现代医生,2016,54(8):82-84. [39] 黄自强,吴俊杰,吴琼华. 纤维支气管镜下支气管结核冷冻疗法对肉芽增殖型支气管结核的疗效与安全性[J]. 安徽医学,2021,42(3):257-260. [40] 陆兰英,靖秋生,王卫华. 经纤维支气管镜注药联合雾化吸入治疗支气管结核的疗效观察[J]. 中国防痨杂志,2010,32(2):104-107. [41] 谭红玉. 经可弯曲纤维支气管镜局部注药联合雾化吸入结核药物方法治疗支气管内膜结核的疗效观察[J]. 中国伤残医学,2014,22(6):152-154. [42] Su Z,Cheng Y,Wu Z,et al. Incidence and predictors of tracheobronchial tuberculosis in pulmonary tuberculosis: A multicentre,large-scale and prospective study in Southern China[J]. Respiration,2019,97(2):153-159. doi: 10.1159/000492335 [43] 《中华结核和呼吸杂志》编辑委员会. 支气管结核的几点专家共识[J]. 中华结核和呼吸杂志,2009,32(8):568-571. [44] Momin M A M,Rangnekar B,Sinha S,et al. Inhalable dry powder of bedaquiline for pulmonary tuberculosis: In vitro physicochemical characterization,antimicrobial activity and safety studies[J]. Pharmaceutics,2019,11(10):502. doi: 10.3390/pharmaceutics11100502 [45] Rangnekar B,Momin M A M,Eedara B B,et al. Bedaquiline containing triple combination powder for inhalation to treat drug-resistant tuberculosis[J]. Int J Pharm,2019,570(10):118689. [46] Shao Z,Tai W,Qiu Y,et al. Spray-dried powder formulation of capreomycin designed for inhaled tuberculosis therapy[J]. Pharmaceutics,2021,13(12):2044. doi: 10.3390/pharmaceutics13122044 [47] Rai P Y,Sansare V A,Warrier D U,et al. Formulation,characterization and evaluation of inhalable effervescent dry powder of Rifampicin nanoparticles[J]. Indian J Tuberc,2023,70(1):49-58. doi: 10.1016/j.ijtb.2022.03.007 [48] Bax H I,de Steenwinkel J E,Ten Kate M T,et al. Colistin as a potentiator of anti-TB drug activity against Mycobacterium tuberculosis[J]. J Antimicrob Chemother,2015,70(10):2828-2837. doi: 10.1093/jac/dkv194 [49] Stewart I E,Lukka P B,Liu J,et al. Development and characterization of a dry Powder formulation for anti-tuberculosis drug spectinamide 1599[J]. Pharm Res,2019,36(9):136. doi: 10.1007/s11095-019-2666-8 [50] Gonzalez-Juarrero M,Lukka P B,Wagh S,et al. Preclinical evaluation of inhalational spectinamide-1599 therapy against tuberculosis[J]. ACS Infect Dis,2021,7(10):2850-2863. doi: 10.1021/acsinfecdis.1c00213 [51] 张慧珊,陈熙泼,叶乐平,等. 经支气管镜冷冻介入在儿童气管支气管结核诊疗中的临床应用[J]. 中华儿科杂志,2021,59(11):963-967. [52] Ni C,Yu H,Han X,et al. Clinical analysis of bronchoscopic cryotherapy in 156 pediatric patients[J]. Pediatr Int,2017,59(1):62-67. doi: 10.1111/ped.13088 -




 点击查看大图
点击查看大图
计量
- 文章访问数: 1973
- HTML全文浏览量: 892
- PDF下载量: 22
- 被引次数: 0
