

The Antinociception of Galanin on Nucleus Accumbens and Its Mechanism in Rats
-
摘要:
目的 研究伏核甘丙肽对正常大鼠、炎症痛大鼠和神经痛大鼠的镇痛作用,并初步探索其机制。 方法 炎症痛动物模型采用鹿角菜碱足底皮下注射的方法制备,神经痛动物模型采用左侧坐骨神经结扎的方法制备。测量大鼠的后爪缩爪潜伏期(hind-paw withdraw latency,HWL)和后爪缩爪阈值(hind-paw withdraw threshold,HWT)来反应痛阈;使用蛋白免疫印迹法检测大鼠伏核甘丙肽受体(galanin receptors,GalRs)的表达。 结果 (1)伏核注射甘丙肽引起正常大鼠(P左 < 0.05;P右 < 0.01)、炎症痛大鼠(P左 < 0.001;P右 < 0.001)和神经痛大鼠(P左 < 0.001;P右 < 0.001)的HWL延长,且正常大鼠(P左 < 0.001;P右 < 0.01)、炎症痛大鼠(P左 < 0.001;P右 < 0.001)和神经痛大鼠(P左 < 0.001;P右 < 0.001)的HWT增加;(2)比较甘丙肽对3种大鼠的镇痛作用,甘丙肽对炎症痛大鼠(HWL:P左 < 0.05,P右 < 0.05;HWT:P左 < 0.01,P右 < 0.05)和神经痛大鼠(HWL:P左 < 0.05,P右 < 0.05;HWT:P左 < 0.001,P右 < 0.001)的镇痛作用比对正常大鼠的镇痛作用强;但比较甘丙肽对炎症痛大鼠和神经痛大鼠的镇痛作用,差异无统计学意义(P > 0.05);(3)足底皮下注射鹿角菜碱后3 h(P < 0.001)和坐骨神经结扎后14 d(P < 0.001)引起大鼠伏核神经细胞GalR1的表达上调,且注射鹿角菜碱后3 h(P < 0.05)和坐骨神经结扎后14 d(P < 0.05)大鼠伏核神经细胞GalR2的表达也上调。 结论 伏核甘丙肽对正常大鼠、炎症痛大鼠和神经痛大鼠都具有镇痛作用,甘丙肽通过和其受体结合对大鼠具有镇痛作用。 Abstract:Objective To research the analgesic effect of galanin on native rats, inflammatory rats and neuropathic rats in nucleus accumbens (NAc), and to explore its mechanism. Methods A inflammatory pain model was prepared by subcutaneous injection of carrageine into rat’s plantar, while the model of neuralgia was prepared by ligation of the left sciatic nerve. The hind-paw withdraw latency (HWL) induced by thermal stimulation and the hind-paw withdraw threshold (HWT) induced by mechanical stimulation were measured to reflect the pain threshold. The expression of galanin receptors (GalRs) in the nucleus accumbens of inflammatory and neuropathic rats were detected by western blot (WB). Results 1. The HWL of normal (Pleft < 0.05; Pright < 0.01), inflammatory (Pleft < 0.001; Pright < 0.001) and neuropathic (Pleft < 0.001; Pright < 0.001) rats were increased by injection of galanin into nucleus accumbens, and the HWT of normal (Pleft < 0.001; Pright < 0.01), inflammatory (Pleft < 0.001; Pright < 0.001) and neuropathic (Pleft < 0.001; Pright < 0.001) rats also were increased. 2. The antinociception of galanin on the rats with inflammatory (HWL: Pleft < 0.05, Pright < 0.05; HWT: Pleft < 0.01, Pright < 0.05) or neuropathic pain (HWL: Pleft < 0.05, Pright < 0.05; HWT: Pleft < 0.001, Pright < 0.001) was stronger than that of the native rats. However, the antinociception of galanin on the rats with the inflammatory pain and neuropathic pain was not significantly different (P > 0.05). 3. The expressions of GalR1 were increased in rats after 3 hours of subcutaneous injection of carrageine (P < 0.001) and 14 days of sciatic nerve ligation (P < 0.001), and the expressions of GalR2 also were increased in rats after 3 hours of subcutaneous injection of carrageine (P < 0.05) and 14 days of sciatic nerve ligation (P < 0.05). Conclusion Intra-NAc injection of galanin has the antinociceptive effects on native, inflammatory and neuralgia rats and the antinociceptive effect of galanin in rats is induced by the activation of GalRs. -
Key words:
- Galanin /
- Neuralgia /
- Inflammatory pain /
- Antinociceptive effect /
- Nucleus accumbens
-

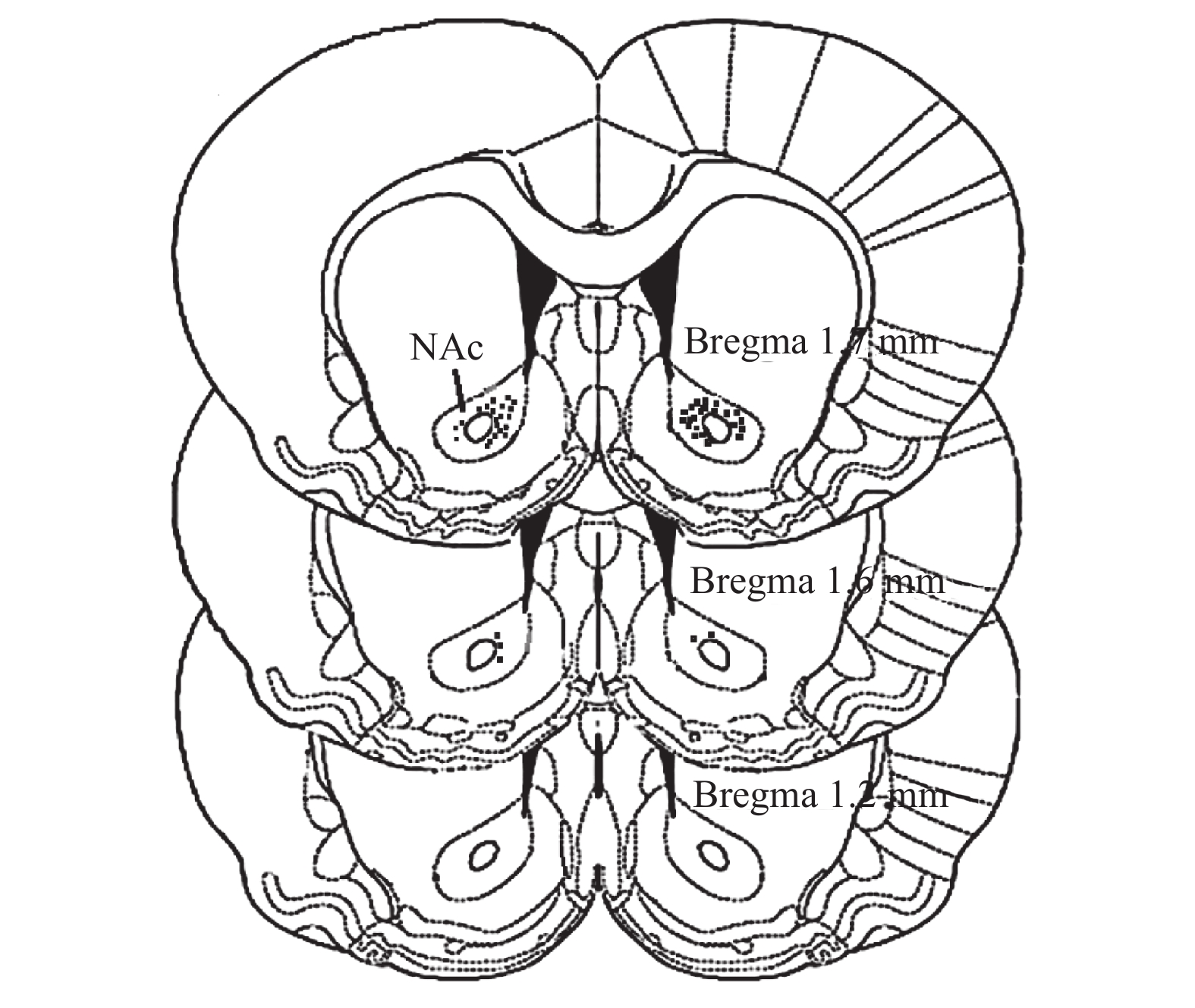
图 1 伏核注射位点鉴定图
NAc:伏核。
Figure 1. Illustration of the location of the injection needle tips

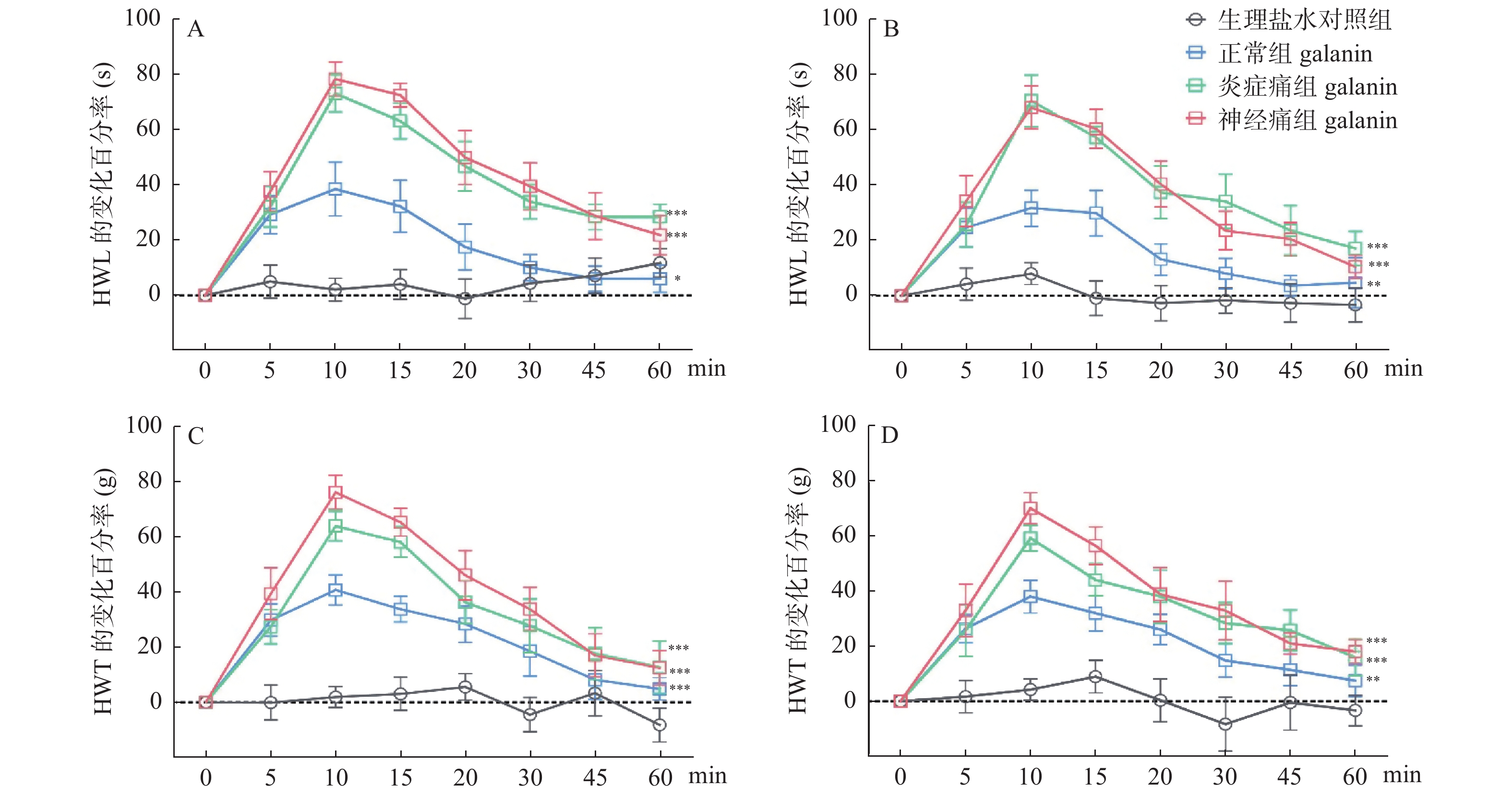
图 2 伏核注射甘丙肽对正常大鼠、炎症痛大鼠和神经痛大鼠 HWL 和 HWT 的影响
A:左 HWL、B:右 HWL、C:左 HWT、D:右 HWT。 与生理盐水对照组比较, *P < 0.05、 **P < 0.01、***P < 0.001。
Figure 2. Effects of intra-NAc injection of galanin on HWL and HWT in normal, inflammatory and CCI rats

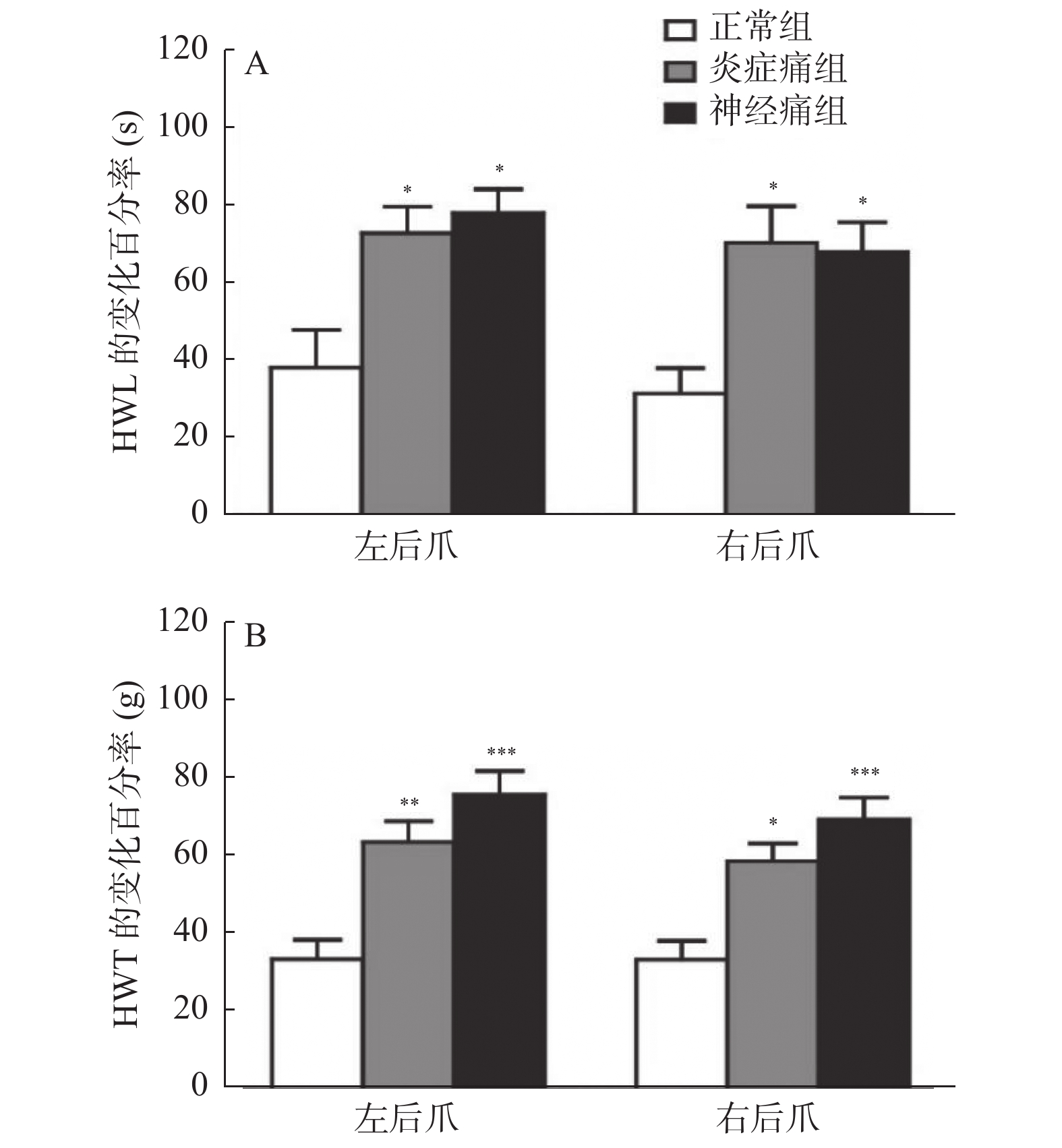
图 3 甘丙肽对正常大鼠、炎症痛大鼠和神经痛大鼠的镇痛作用比较
与正常组比较,*P < 0.05、**P < 0.01、***P < 0.001。
Figure 3. Comparison of analgesic effects of galanin on native, inflammatory and CCI rats
-
[1] Tatemoto K,Rökaeus A,Jörnvall H,et al. Galanin-a novel biologically active peptide from porcine intestine[J]. FEBS Lett,1983,164(1):124-128. doi: 10.1016/0014-5793(83)80033-7 [2] Taylor T S,Konda P,John S S,et al. Galanin suppresses visceral afferent responses to noxious mechanical and inflammatory stimuli[J]. Physiological Reports,2020,8(2):e14326. [3] Yu M,Fang P H,Wang H,et al. Beneficial effects of galanin system on diabetic peripheral neuropathic pain and its complications[J]. Peptides,2020,134(12):170404. [4] Liu F, Yajima T, Wang M, et al. Effects of trigeminal nerve injury on the expression of galanin and its receptors in the rat trigeminal ganglion [J]. Neuropeptides, 2020, 84(期号!): 102098.Liu F,Yajima T,Wang M,et al. Effects of trigeminal nerve injury on the expression of galanin and its receptors in the rat trigeminal ganglion[J]. Neuropeptides,2020,84:102098. [5] Amorim D,David-Pereira A,Marques P,et al. A role of supraspinal galanin in behavioural hyperalgesia in the rat[J]. Plos one,2014,9(11):e113077. doi: 10.1371/journal.pone.0113077 [6] Dias E V,Sartori C R,Mariao P R,et al. Nucleus accumbens dopaminergic neurotransmission switches its modulatory action in chronification of inflammatory hyperalgesia[J]. Eur J Neurosci,2015,42(7):2380-2389. doi: 10.1111/ejn.13015 [7] Duan H,Zhang Y,Zhang X M,et al. Antinociceptive roles of galanin receptor 1 in nucleus accumbens of rats in a model of neuropathic pain[J]. J Neurosci Res,2015,93(10):1542-1551. doi: 10.1002/jnr.23611 [8] Mitsukawa K,Lu X,Bartfai T. Galanin,galanin receptors and drug targets[J]. Cell Mol Life Sci,2008,65(12):1796-1805. doi: 10.1007/s00018-008-8153-8 [9] Gear R W,Aley K O,Levine J D. Pain—induced analgesia mediated by mesolimbic reward circuits[J]. J Neurosci,1999,19(16):7175-7181. doi: 10.1523/JNEUROSCI.19-16-07175.1999 [10] Watanabe M,Sugiura Y,Sugiyama E,et al. Extracellular N- acetylaspartylglutamate released in the nucleus accumbens modulates the pain sensation: Analysis using a microdialysis/mass spectrometry integrated system[J]. Mol Pain,2018,14:1744806918754934. [11] Zhang Y, Gao Y, Li CY, et al. Galanin plays a role in antinociception via binding to galanin receptors in the nucleus accumbens of rats with neuropathic pain [J]. Neurosci Lett, 2019, 706(期号?): 93-98.Zhang Y,Gao Y,Li C Y,et al. Galanin plays a role in antinociception via binding to galanin receptors in the nucleus accumbens of rats with neuropathic pain[J]. Neurosci Lett,2019,706:93-98. [12] Zhang, ML, Fu, FH, Yu, LC. Antinociception induced by galanin in anterior cingulate cortex in rats with acute inflammation [J]. Neurosci. Lett. 2017, 638(期号?): 156-161.Zhang M L,Fu F H,Yu L C. Antinociception induced by galanin in anterior cingulate cortex in rats with acute inflammation[J]. Neurosci Lett,2017,638:156-161. [13] Zhang M L,Wang H B,Fu F H,et al. Involvement of galanin and galanin receptor 2 in nociceptive modulation in anterior cingulate cortex of normal rats and rats with mononeuropathy[J]. Sci Rep,2017,7(1):45930. doi: 10.1038/srep45930 [14] Li S Y,Huo M L,Wu X Y,et al. Involvement of galanin and galanin receptor 1 in nociceptive modulation in the central nucleus of amygdala in normal and neuropathic rats[J]. Sci Rep,2017,7(1):15317. doi: 10.1038/s41598-017-13944-6 [15] Li L X, Wang X B, Yu L C. Involvement of opioid receptors in the CGRP-induced antinociception in the nucleus accumbens of rats[J]. Brain Res,2010,1353:53-59. [16] Hobson S A,Bacon A,Elliot-Hunt C R,et al. Galanin acts as a trophic factor to the central and peripheral nervous systems[J]. Cell Mol Life Sci,2008,65(12):1806-1812. [17] Barreda-Gómez G,Giralt M T,Rodríguez-Puertas R. G protein-coupled galanin receptor distribution in the rat central nervous system[J]. Neuropeptides,2005,39(3):153-156. [18] Lang R,Gundlach A L,Holmes F E,et al. Physiology,signaling,and pharmacology of galanin peptides and receptors: Three decades of emerging diversity[J]. Pharmacol Rev,2015,67(1):118-175. doi: 10.1124/pr.112.006536 [19] Chen S H,Lue J H,Hsiao Y J,et al. Elevated galanin receptor type 2 primarily contributes to mechanical hypersensitivity after median nerve injury[J]. PLoS ONE,2018,13(6):e0199512. [20] Xu X F,Yang X D,Zhang P,et al. Effects of exogenous galanin on neuropathic pain state and change of galanin and its receptors in DRG and SDH after sciatic nerve-pinch injury in rat[J]. Plos One,2012,7(5):e37621. doi: 10.1371/journal.pone.0037621 [21] Dong Yan,Li Chongyang,Zhang Xiaomin,et al. The activation of galanin receptor 2 plays an antinociceptive effect in nucleus accumbens of rats with neuropathic pain[J]. J Physiol Sci,2021,71(1):6. doi: 10.1186/s12576-021-00790-5 [22] Mengnan Li, Xiaomin Zhang, Chongyang Li, et al. Galanin receptor 2 is involved in galanin-induced analgesic effect by activating PKC and CaMKII in the nucleus accumbens of inflammatory pain rats [J]. Front Neurosci, 2021, 14(期号?): 593331.Li Mengnan,Zhang Xiaomin,Li Chongyang,et al. Galanin receptor 2 is involved in galanin-induced analgesic effect by activating PKC and CaMKII in the nucleus accumbens of inflammatory pain rats[J]. Front Neurosci,2021,14:593331. -

 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 1921
- HTML全文浏览量: 1211
- PDF下载量: 17
- 被引次数: 0
