

Analysis of Correlations of Age,Diseases and Blood Pressure Based on a Population of 82782 Individuals
-
摘要:
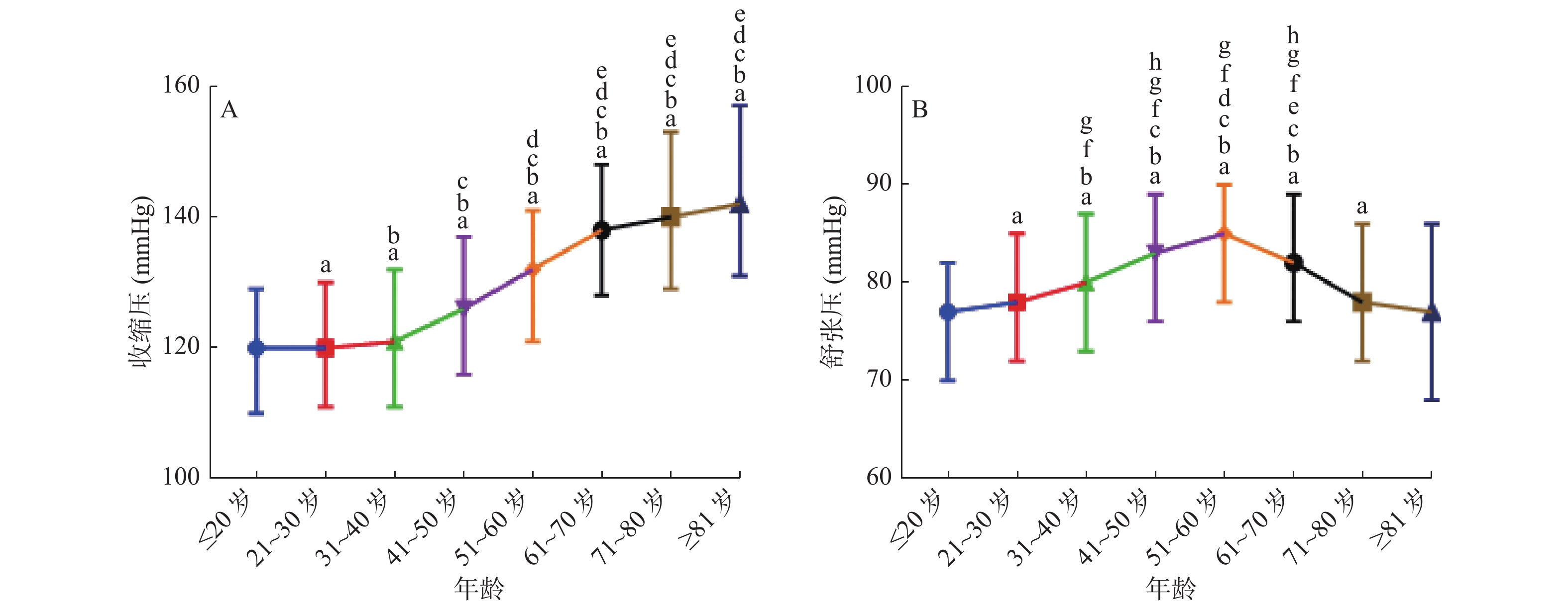
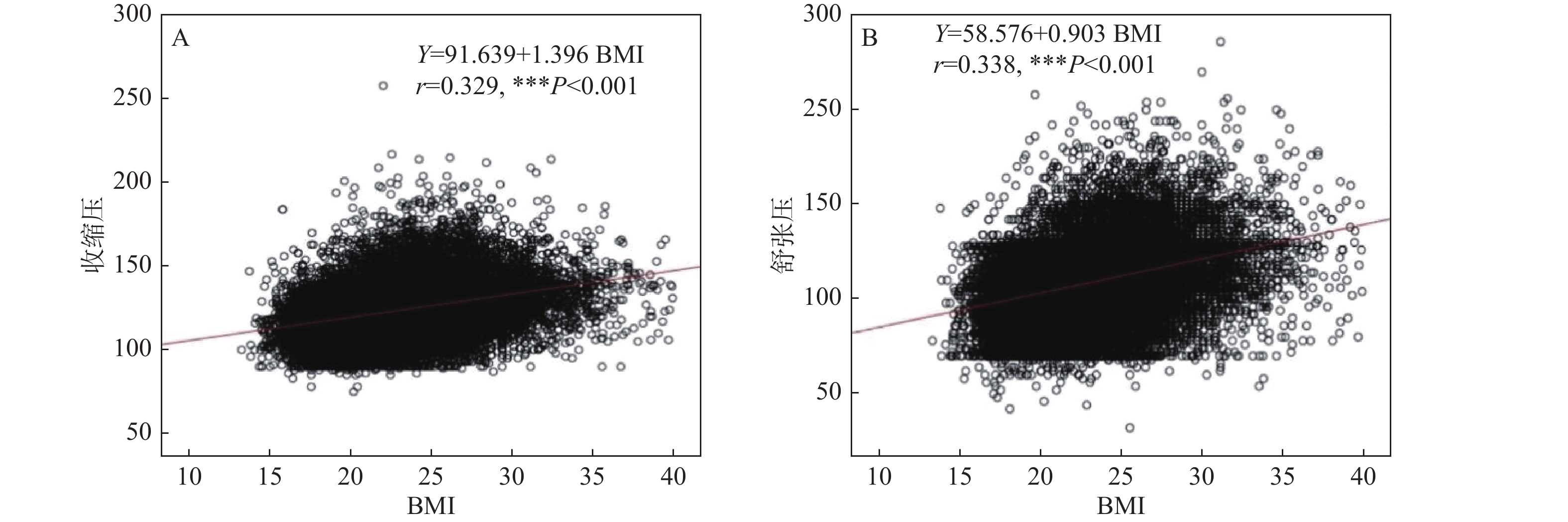
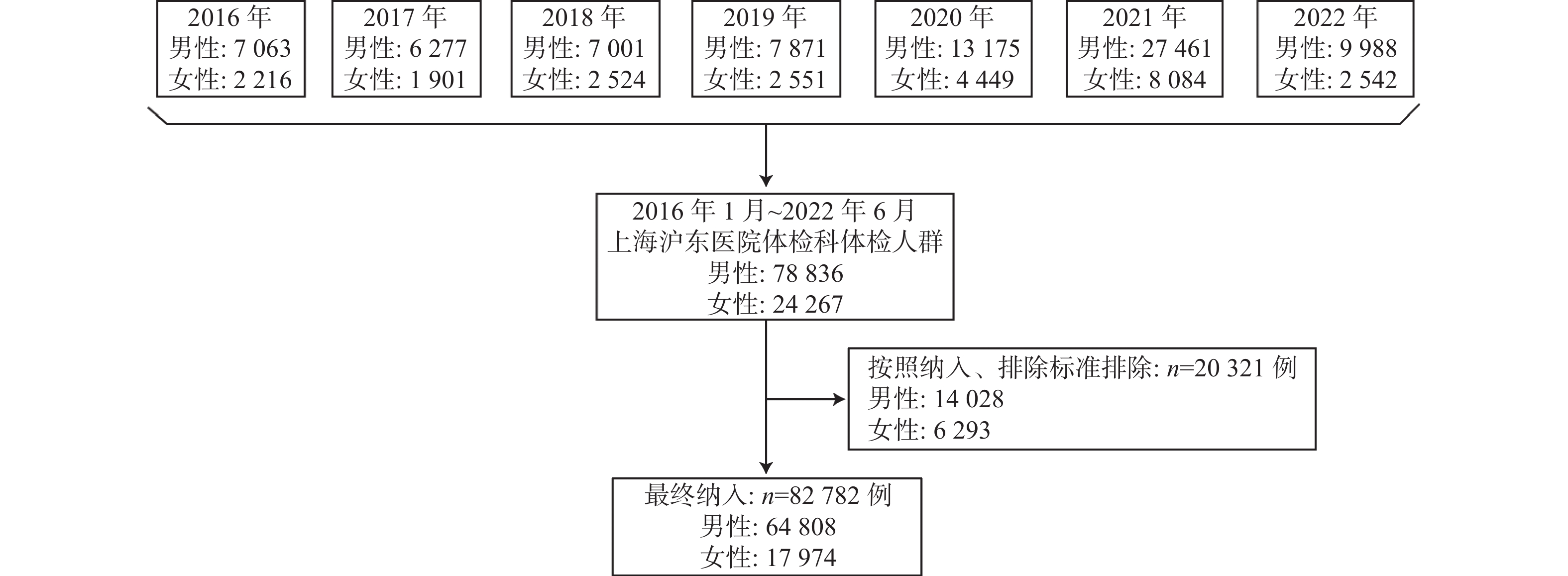
目的 探究年龄和疾病与血压的相关性。 方法 采用回顾性研究,将2016年1月到2022年6月在上海沪东医院体检科体检并符合相关标准的82 782例人群纳入研究。按照10岁为1个年龄阶段分组,分为≤20岁组,21~30岁组,31~40岁组,41~50岁组,51~60岁组,61~70岁组,71~80岁组和≥81岁组,比较各组的收缩压和舒张压水平;采用Pearson双变量相关方法,分析BMI与收缩压和舒张压的相关性;再次筛选数据,根据体检结果归类,体检人群分为对照组和疾病组,应用Logistic分析高血压发生与疾病因素的相关性。 结果 收缩压随着衰老发生具有不断增高的趋势,到61~70岁组之前,后1个年龄段组人群的收缩压水平一直高于之前年龄段组(P < 0.01)。舒张压随着年龄增加也具有增加的趋势,51~60岁之间舒张压最高,之后则显著降低。Logistic分析结果显示校正年龄和BMI因素后,代谢综合征对单纯收缩压的影响,差异有统计学意义( OR = 1.068,P = 0.042);代谢综合征对收缩压和舒张压均升高的高血压影响,差异具有统计学意义(OR = 1.032,P = 0.038)。 结论 血压变化具有年龄特异性,收缩压随着衰老发生具有不断增高的趋势,舒张压则在51~60岁之间达到最高值,之后不断降低;代谢综合征与高血压的发生具有关联。 Abstract:Objective To investigate the correlations of age, diseases and blood pression (BP). Methods A retrospective study was conducted to include 82 782 patients who underwent physical examination in the physical examination department of Hudong Hospital in Shanghai from January 2016 to June 2022 and met relevant criteria. Grouping according to age stages, with each stage representing 10 years, the groups are divided into ≤20 years, 21-30 years, 31-40 years, 41-50 years, 51-60 years, 61-70 years, 71-80 years, and ≥81 years. Pearson bivariate correlation method was used to analyze the correlation between BMI and systolic and diastolic blood pressure. The data were screened again and classified according to the physical examination results. The physical examination population was divided into control group and disease group, and the correlation between hypertension and disease factors was analyzed by Logistic analysis. Results Systolic blood pressure tended to increase with age, and the level of systolic blood pressure in the group aged 61-70 was consistently higher than in the younger age groups (P < 0.01). Diastolic blood pressure also showed an increasing trend with age, with the highest levels observed between the ages of 51 and 60, followed by a significant decrease. Logistic analysis results indicated that after adjusting for age and BMI factors, metabolic syndrome had a statistically significant impact on isolated systolic blood pressure (OR = 1.068, P = 0.042). Furthermore, metabolic syndrome had a statistically significant effect on both systolic and diastolic blood pressure elevation in hypertension (OR = 1.032, P = 0.038). Conclusion Blood pressure changes have age specificity, with systolic blood pressure showing a continuous increase with aging. Diastolic blood pressure reaches its highest value between the ages of 51 and 60, and then gradually decreases. Metabolic syndrome is associated with the occurrence of hypertension. -
Key words:
- Age /
- Blood pressure /
- Diseases
-

图 2 各年龄段组血压水平比较 [Median (IQR)]
A:收缩压;B:舒张压;与≤20岁年龄组比较,a P < 0.01;与21~30岁年龄组比较,b P < 0.01;与31~40岁年龄组比较,c P < 0.01;与41~50岁年龄组比较,d P < 0.01;与51~60岁年龄组比较,e P < 0.01;与≥81岁年龄组比较,f P < 0.01;与71~80岁年龄组比较,g P < 0.01;与51~60岁年龄组比较,h P < 0.01。
Figure 2. The blood pressure levels comparison among the groups

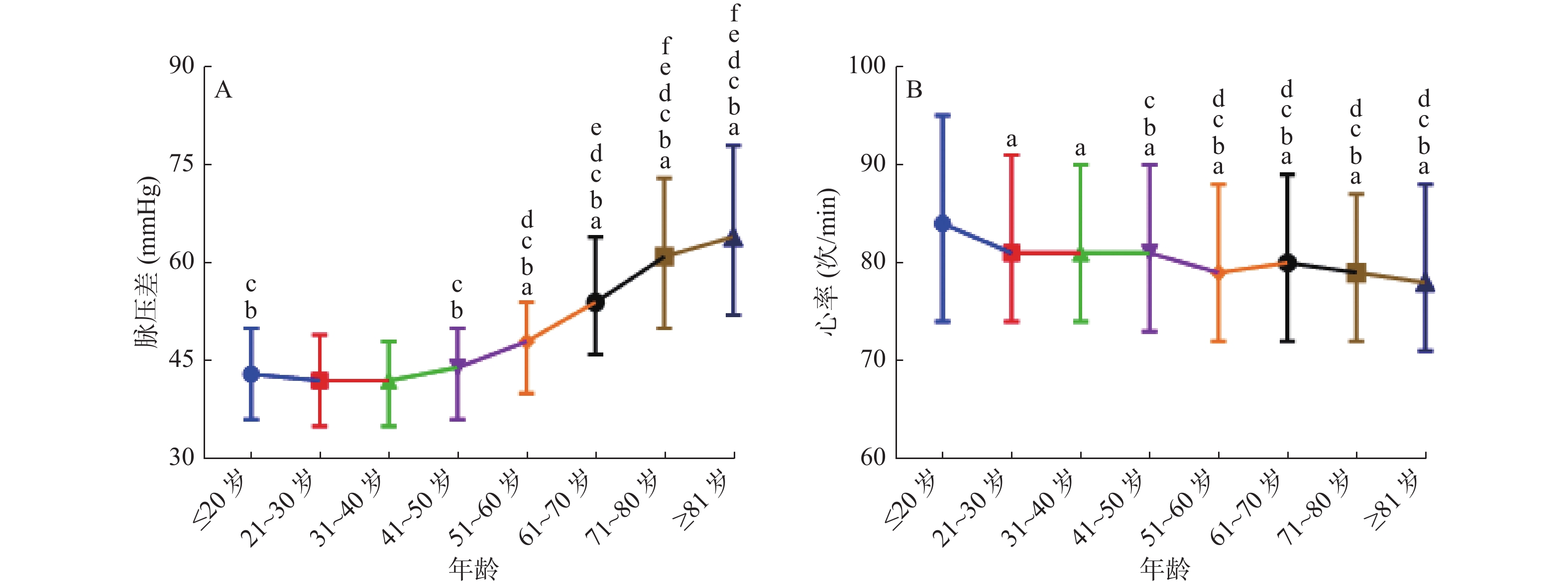
图 3 各年龄段组脉压差和心率水平比较 [Median (IQR)]
A:脉压差;B:心率;与≤20岁年龄组比较aP < 0.01;与21~30岁年龄组比较,bP < 0.01;与31~40岁年龄组比较,cP < 0.01;与41~50岁年龄组比较,d P < 0.01;与51~60岁年龄组比较,eP < 0.01;与61~70岁年龄组比较,fP < 0.01。
Figure 3. The Pulse pressure difference and Heart rate levels comparison among the groups [Median (IQR)]

图 4 BMI与血压的相关性分析
A:收缩压;B:舒张压。
Figure 4. The correlation analysis between BMI and blood pressure
表 1 纳入人群的一般特点 [(%)/( $\bar x \pm s $)]
Table 1. The common characteristics of the included subjects [(%)/( $\bar x \pm s $)]
项目 n /值 总人数 82782 性别 男 64808 (78.29) 女 17974 (21.71) 年龄 (岁) 36.20 ± 12.82 BMI (kg/m2) a 23.27 ± 3.85 年龄段b(岁) ≤20 7121 (8.60) 21~30 22983 (27.76) 31~40 24807 (30.00) 41~50 16932 (20.45) 51~60 7361 (8.89) 61~70 1998 (2.41) 71~80 849 (1.03) ≥81 448 (0.54) 血压 (mmHg) c 收缩压 123.85 ± 15.51 舒张压 80.30 ± 10.15 心率 (次/min) d 82.54 ± 15.72 a:样本量64880人;b:样本量82499人;c:样本量82782人;d: 样本量82780人。  下载: 导出CSV
下载: 导出CSV
表 2 Logistic分析人群发生单纯高收缩压与疾病因素的相关性
Table 2. Logistic analysis for the correlations between the occurrence of simple high systolic blood pressure and disease factors in the people
高血压
(单纯收缩压高)单因素Logistic分析A 多因素Logistic分析B 多因素Logistic分析C 多因素Logistic分析D OR P OR OR OR P OR P 心脏异常a 0.402 < 0.001 ** 0.203 < 0.001 ** 0.004 < 0.001 ** - - 代谢综合征b 1.144 0.001** 1.123 < 0.001 ** 1.079 < 0.001 ** 1.068 0.042* 血清炎症水平增高c 0.710 0.008** 0.231 0.040* - - - - 肝胆类病变d 0.213 < 0.001 ** 0.257 < 0.001 ** - - - - 肺部疾病e 0.443 < 0.001 ** 0.392 < 0.001 ** - - - - 红细胞升高f 0.493 0.007** - - - - - - 贫血g 0.364 0.005** 0.487 0.046* - - - - A:与对照组体检人群比较,并以未患该类疾病为参照;B: 与对照组体检人群比较,并矫正了年龄的因素,并以未患该类疾病为参照; C:与对照组体检人群比较,并矫正了BMI的因素;D:与对照组体检人群比较,并矫正了年龄、BMI的因素,并以未患该类疾病为参照;-:无统计学意义或未纳入方程;*P < 0.05, **P < 0.001。
下载: 导出CSV
表 3 Logistic分析人群发生高血压与疾病因素的相关性
Table 3. Logistic analysis for the correlations between the occurrence of high blood pressure and disease factors in the people
高血压
(收缩/舒张压均高)单因素Logistic分析A 多因素Logistic分析B 多因素Logistic分析C 多因素Logistic分析D OR P OR P OR P OR P 心脏异常a 0.600 < 0.001 ** 0.371 0.001** - - - - 代谢综合征b 1.065 < 0.001 ** 1.055 < 0.001 ** 1.044 < 0.001 ** 1.032 0.038* 血清炎症水平增高c 0.051 < 0.001 ** 0.069 < 0.001 ** - - - - 肝胆类病变d 0.143 < 0.001 ** 0.156 < 0.001 ** - - - - 肺部疾病e 0.641 < 0.001 ** - - - - - - 红细胞升高f 0.641 0.001** - - - - - - 贫血g 0.275 < 0.001 ** 0.328 < 0.001 ** - - - - A:与对照组体检人群比较,并以未患该类疾病为参照;B:与对照组体检人群比较,并矫正了年龄的因素,并以未患该类疾病为参照; C:与对照组体检人群比较,并矫正了BMI的因素,并以未患该类疾病为参照;D:与对照组体检人群比较,并矫正了年龄、BMI的因素,并以未患该类疾病为参照。*P < 0.05, **P < 0.001。
下载: 导出CSV
-
[1] Mills K T,Bundy J D,Kelly T N,et al. Global disparities of hypertension prevalence and control: A systematic analysis of population-based studies from 90 countries[J]. Circulation,2016,134(6):441-450. doi: 10.1161/CIRCULATIONAHA.115.018912 [2] Xiong P,Liu Z,Xiong M,et al. Prevalence of high blood pressure under 2017 ACC/AHA guidelines: A systematic review and meta-analysis[J]. J Hum Hypertens,2021,35(3):193-206. doi: 10.1038/s41371-020-00454-8 [3] GBD 2015 Risk Factors Collaborators. Global,regional,and national comparative risk assessment of 79 behavioural,environmental and occupational,and metabolic risks or clusters of risks,1990-2015: A systematic analysis for the Global Burden of Disease Study 2015[J]. Lancet,2016,388(10053):1659-1724. doi: 10.1016/S0140-6736(16)31679-8 [4] 蔡军,孙英贤,李玉明,等. 中国高血压临床实践指南[J]. 中华心血管病杂志,2022,50(11):1050. [5] 夏文豪,董兵,刘晓玲,等. 衰老成血管T细胞与高血压患者血管内皮功能障碍及炎症状态的相关性[J]. 中华高血压杂志,2021,29(10):972-980. [6] Fuchs F D,Whelton P K. High blood pressure and cardiovascular disease[J]. Hypertension,2020,75(2):285-292. doi: 10.1161/HYPERTENSIONAHA.119.14240 [7] 陈琦玲. 特殊类型高血压临床诊治要点专家建议[J]. 中国全科医学,2020,23(10):1202-1228. [8] Flack J M,Adekola B. Blood pressure and the new ACC/AHA hypertension guidelines[J]. Trends Cardiovasc Med,2020,30(3):160-164. doi: 10.1016/j.tcm.2019.05.003 [9] 高血压联盟(中国),中华医学会心血管病学分会,中国医师协会高血压专业委员会,等. 中国高血压防治指南2018年修订版[J]. 心脑血管病防治,2019,19(1):1-44. [10] Turin T C,Okamura T,Afzal A R,et al. Hypertension and lifetime risk of stroke[J]. Journal of Hypertension,2016,34(1):116-122. doi: 10.1097/HJH.0000000000000753 [11] Fabian J,Gondwe M,Mayindi N,et al. Chronic kidney disease (CKD) and associated risk in rural South Africa: A population-based cohort study[J]. Wellcome Open Research,2022,7(3):236. [12] van Dalen J W,Brayne C,Crane P K,et al. Association of systolic blood pressure with dementia risk and the role of age,U-shaped associations,and mortality[J]. JAMA Internal Medicine,2022,182(2):142-152. doi: 10.1001/jamainternmed.2021.7009 [13] 刘建勋,付朝红,李建彬,等. 郑州市年龄≥18岁居民正常高值血压流行状况与相关危险因素[J]. 中华高血压杂志,2023,31(1):61-66. [14] 郭子怡,徐传胜,陈虹,等. 炎症因子C5a和肿瘤坏死因子α刺激对小鼠主动脉内皮细胞衰老与代谢的差异化网络调控作用[J]. 中国分子心脏病学杂志,2021,21(6):4335-4343. [15] 陈凯,唐汉韡,侯剑峰,等. 体外膜肺氧合在心脏外科领域的应用[J]. 中国循环杂志,2019,34(12):1244-1248. doi: 10.3969/j.issn.1000-3614.2019.12.020 [16] Voss A,Schroeder R,Heitmann A,et al. Short-term heart rate variability-influence of gender and age in healthy subjects[J]. PLoS One,2015,10(3):e0118308. doi: 10.1371/journal.pone.0118308 [17] Young J B,Macdonald I A. Sympathoadrenal activity in human obesity: Heterogeneity of findings since 1980[J]. Int J Obes Relat Meatb Disord,1992,16(8):959-967. [18] Seravalle G,Grassi G. Obesity and hypertension[J]. Pharmacol Res,2017,122(7):1-7. [19] Yin R X,Wu D F,Aung L H H,et al. Several lipid-related gene polymorphisms interact with overweight/obesity to modulate blood pressure levels[J]. Int J Mol Sci,2012,13(9):12062-12081. [20] Ratajczak M,Skrypnik D. Effects of endurance and endurance-strength training on endothelial function in women with obesity: A randomized trial[J]. Int J Environ Res Public Health,2019,16(21):4291. doi: 10.3390/ijerph16214291 [21] Wilkinson M J,Manoogian E N C,Zadourian A,et al. Ten-hour time-restricted eating reduces weight,blood pressure,and atherogenic lipids in patients with metabolic syndrome[J]. Cell Metab,2020,31(1):92-104. doi: 10.1016/j.cmet.2019.11.004 [22] Ritter A M,de Faria A P,Barbaro N,et al. Crosstalk between obesity and MMP-9 in cardiac remodelling -a cross-sectional study in apparent treatment-resistant hypertension[J]. Blood Press,2017,26(2):122-129. doi: 10.1080/08037051.2016.1249336 [23] Eckel R H,Grundy S M,Zimmet P Z. The metabolic syndrome[J]. Lancet,2005,365(9468):1415-1428. doi: 10.1016/S0140-6736(05)66378-7 [24] Katsimardou A,Imprialos K,Stavropoulos K,et al. Hypertension in metabolic syndrome: Novel insights[J]. Curr Hypertens Rev,2020,16(1):12-18. doi: 10.2174/1573402115666190415161813 [25] Carli M,Kolachalam S,Longoni B,et al. Atypical antipsychotics and metabolic syndrome: From molecular mechanisms to clinical differences[J]. Pharmaceuticals,2021,14(3):707-715. [26] Roddy G W. Metabolic syndrome and the aging retina[J]. Curr Opin Ophthalmol,2021,32(3):280-287. doi: 10.1097/ICU.0000000000000747 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2771
- HTML全文浏览量: 1768
- PDF下载量: 44
- 被引次数: 0
