

Correlation of 4D-CTA Imaging and Rupture Risk of Anterior Communicating Aneurysms
-
摘要:
目的 探讨利用4D—CTA成像对前交通动脉瘤破裂的风险因素的相关性分析。 方法 选取2020年6月至2023年3月昆明市延安医院放射科前交通动脉瘤患者100例为研究对象,依据患者(是否出现破裂)分为破裂组、未破裂组(每组各50例)并对未破裂组(50例)1~12月保守治疗下并随访观察,测量100例动脉瘤的瘤颈宽(Wn)、瘤高(H)、载瘤动脉平均直径(DA)、瘤长(L)、瘤颈比(AR)、动脉瘤的瘤高与载瘤动脉直径之比(SR)、动脉瘤体积/动脉瘤底面积(VOR)等相关数值以及动脉瘤搏动点的寻找,分析数值与动脉瘤破裂的相关性。 结果 破裂组 1 的Wn、AR、L 和 SR 均大于非破裂组 1(P < 0.05);破裂组 2 的Wn、AR、L 和 SR 均大于非破裂组 2(P < 0.05);4D-CTA中颈内动脉和大脑中动脉的的CT值以及脑实质CT值和噪声均高于3D-CTA(P < 0.05)。 结论 应用4D-CTA成像量化分析前交通动脉瘤,不仅可以对前交通动脉瘤预测破裂风险,还可以得到较3D成像更好的图像质量同时降低辐射剂量,4D-CTA成像对临床动脉瘤的诊疗有积极意义。 Abstract:Objective To explore the correlation between 4D-CTA imaging and the risk factors for the rupture of anterior communicating aneurysms. Methods A total of 100 patients with anterior communicating aneurysms in the Department of Radiology of Yan’ an Hospital of Kunming City from June 2020 to March 2023 were selected as the study objects. The patients were divided into ruptured group and unruptured group based on whether the aneurysm had ruptured(with 50 cases in each group). The unruptured group(50 cases) received conservative treatment and follow-up observation for 1-12 months. The measurements included the aneurysm neck width(Wn), aneurysm height(H), average diameter of the carrying artery(DA), aneurysm length(L), aneurysm neck ratio(AR), the ratio of aneurysm height to carrying artery diameter(SR), aneurysm volume to aneurysm base area(VOR), and the search for the pulsation point of the aneurysm, analyzing the correlation between these measurements and aneurysm rupture. Results Wn, AR, L and SR in ruptured group 1 were higher than those in non-ruptured group 1(P < 0.05). Wn, AR, L and SR in fracture group 2 were higher than those in non-fracture group 2(P < 0.05). The CT values of internal carotid artery and middle cerebral artery, and the CT values and noise of brain parenchyma in 4D-CTA were higher than those in 3D-CTA(P < 0.05). Conclusion The use of 4D-CTA imaging for quantitative analysis of anterior communicating aneurysms can not only predict the risk of rupture, but also provide better image quality compared to 3D imaging while reducing radiation dosage. 4D-CTA imaging has a positive impact on the diagnosis and treatment of clinical aneurysms. -

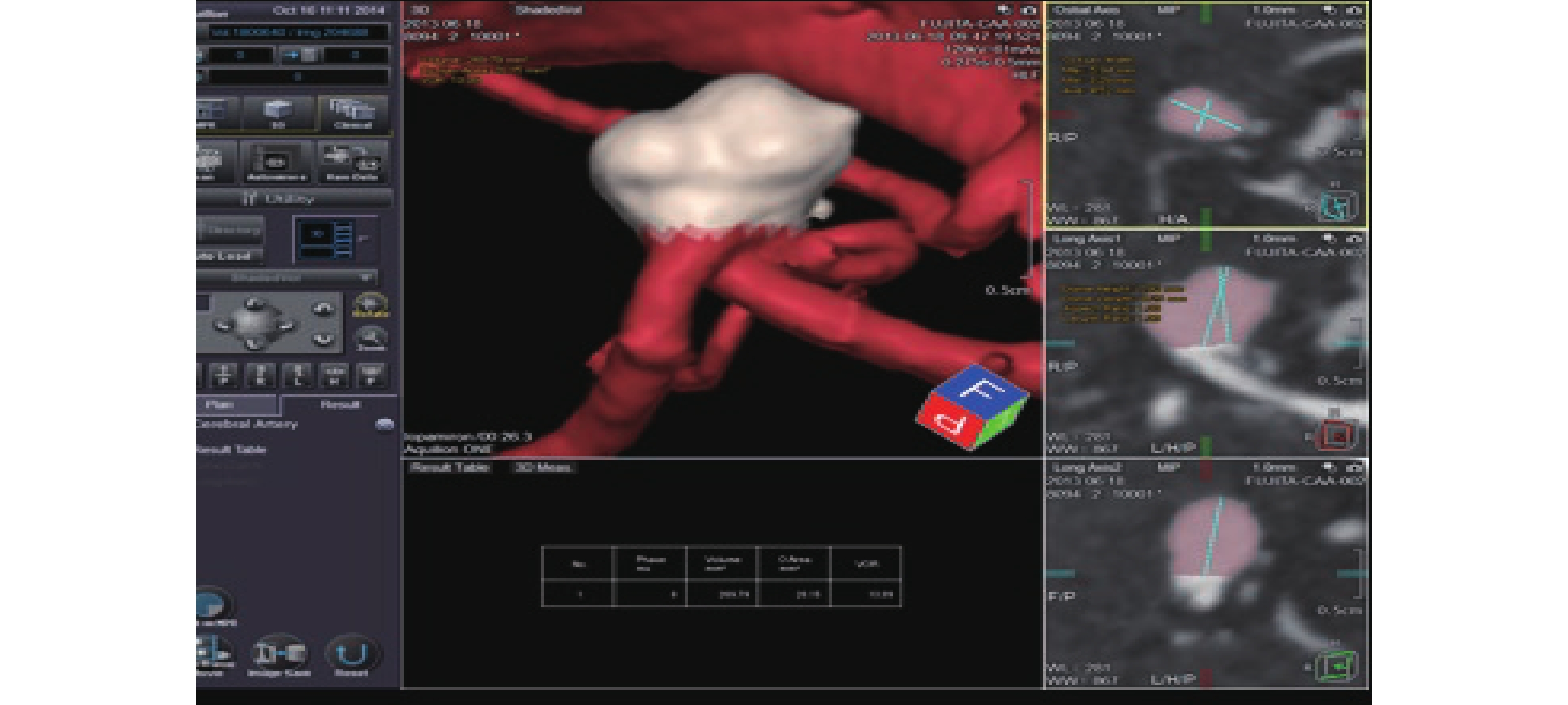
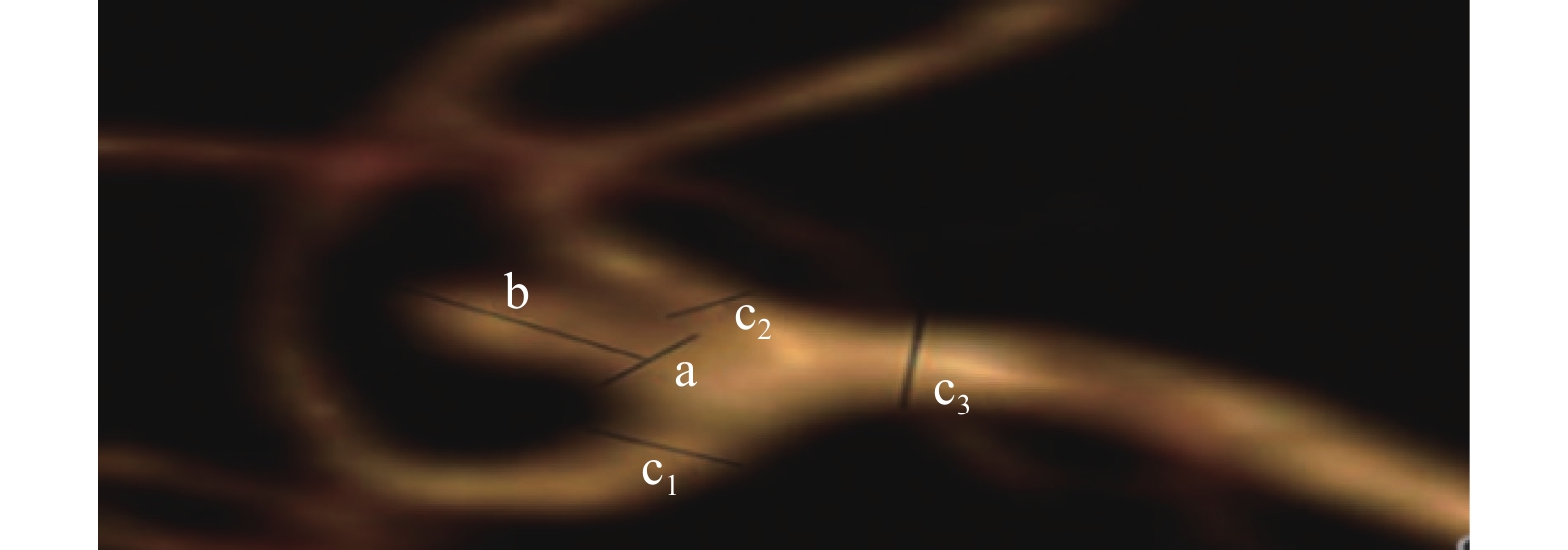
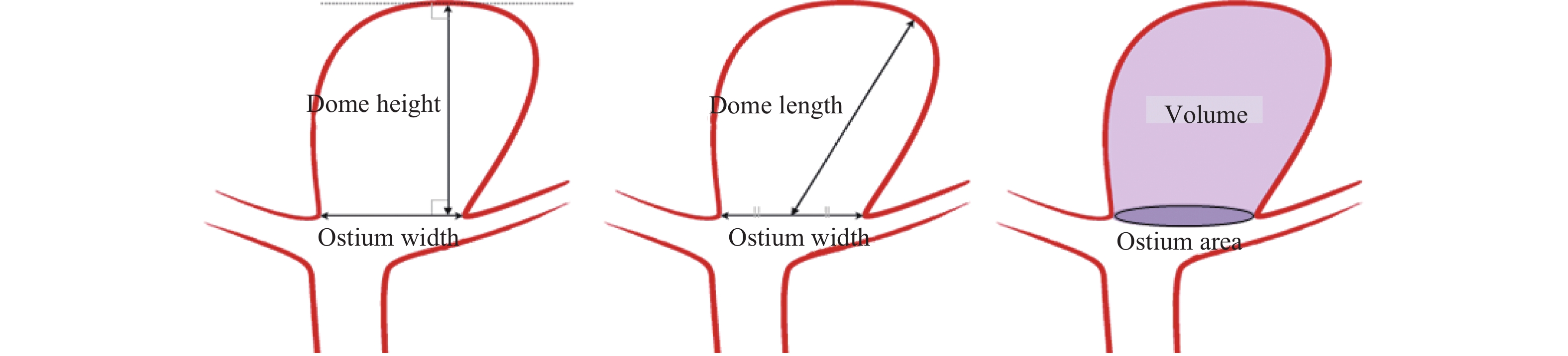
图 3 4D-CTA成像示意图
a:代表瘤颈;b :代表瘤高;c1、c2、c3:分别代表与动脉瘤相关的动脉瘤载瘤动脉直径,即距离近端瘤颈口附近6 mm以内最大的载瘤动脉管径的直径。
Figure 3. 4D-CTA imaging schematic diagram

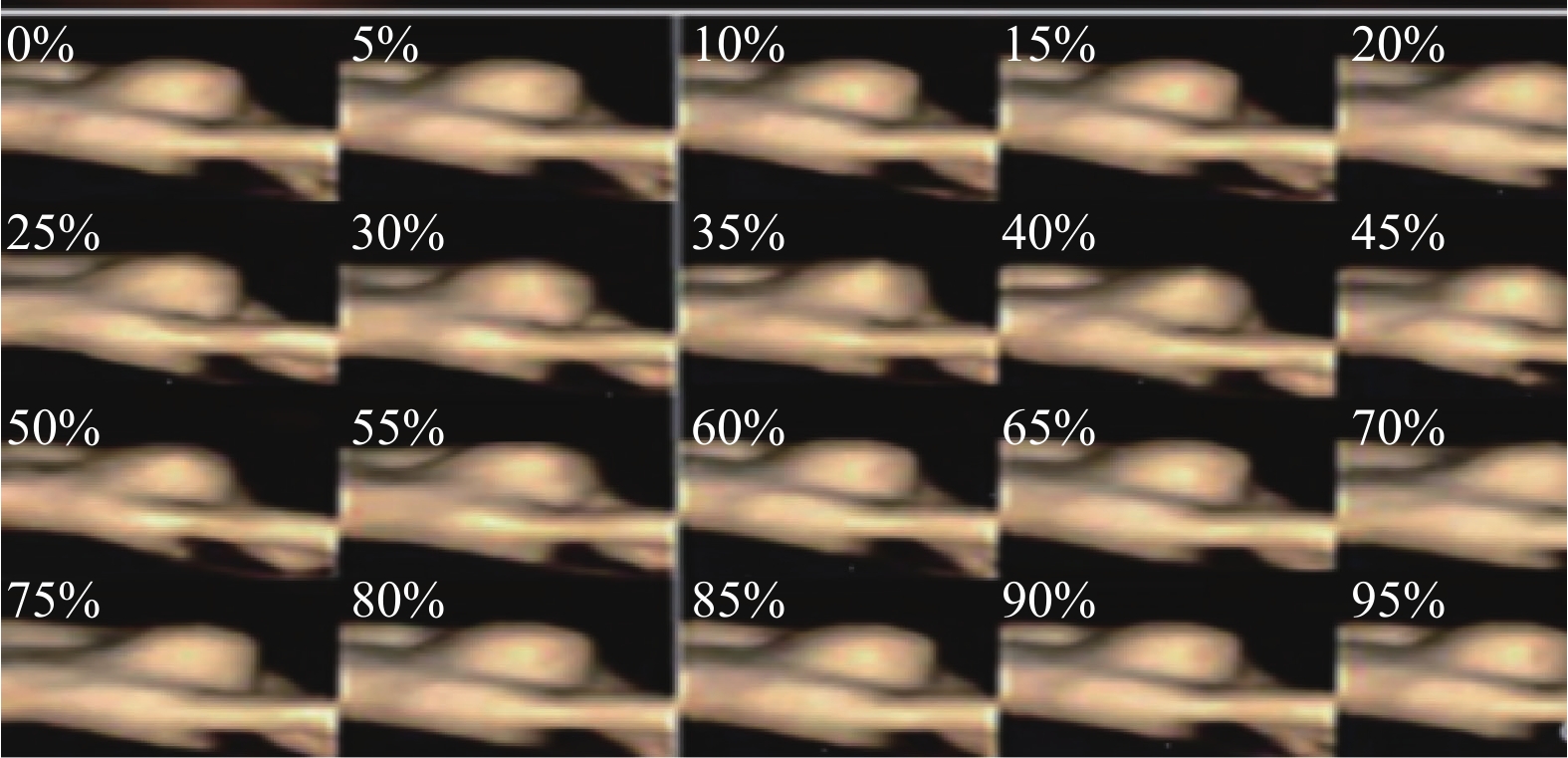
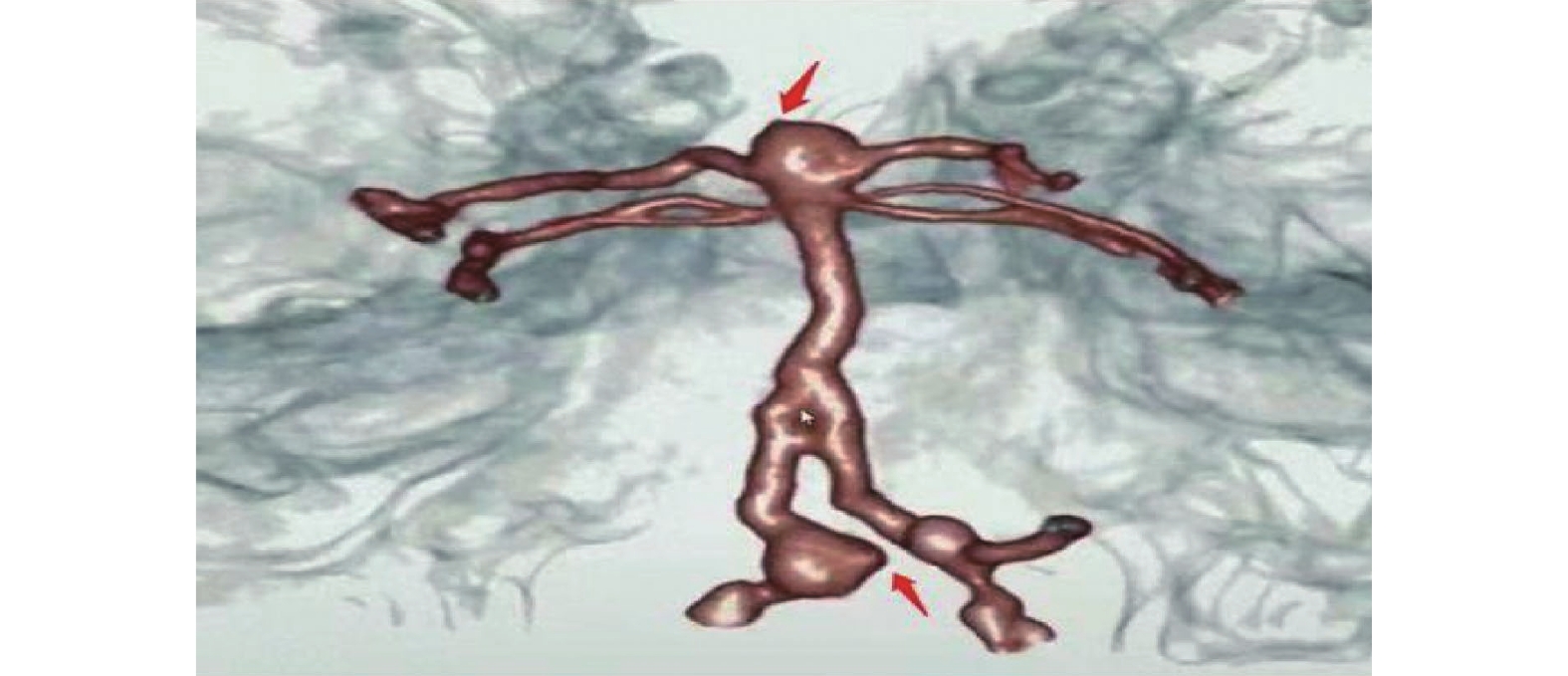
图 5 颅内动脉瘤异常搏动点显示
Figure 5. Display of abnormal pulsation points in intracranial aneurysms
表 1 前交通破裂组1和非破裂组1的4D-CTA成像特征($\bar x \pm s $)
Table 1. 4D-CTA imaging characteristics of ruptured group 1 and non-ruptured group 1 ($\bar x \pm s $)
分组 Wn(mm) H(mm) AR L(mm) DA(mm) SR VOR 破裂组 1 (n=50) 3.28±0.27 3.74±1.75 1.15±0.04 5.11±0.55 3.69±0.57 1.33±0.15 2.06±0.21 非破裂组1 (n=50) 2.88±0.31 3.12±1.34 1.06±0.07 4.36±0.49 3.57±0.61 1.19±0.13 1.87±0.19 t 6.880 1.828 7.894 7.200 1.093 4.987 3.677 P < 0.001* 0.071 < 0.001* < 0.001* 0.277 < 0.001* < 0.001* *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 未破裂组前交通动脉瘤1~12月随访破裂组2和非破裂组2的4D-CTA成像特征($\bar x \pm s $)
Table 2. 4D-CTA imaging characteristics of ruptured group 2 and non-ruptured group 2 during 1~12 months follow-up of anterior communicating aneurysms in the unruptured group ($\bar x \pm s $)
分组 Wn(mm) H(mm) AR L(mm) DA(mm) SR VOR 破裂组 2 (n=19) 2.88±0.27 3.22±1.45 1.10±0.08 4.41±0.55 3.62±0.35 1.22±0.15 1.98±0.15 非破裂组 2 (n=31) 2.26±0.34 3.01±1.25 1.03±0.06 4.03±0.36 3.49±0.51 1.07±0.10 1.88±0.08 t 6.743 0.543 2.517 2.958 0.977 4.248 2.906 P < 0.001* 0.590 0.015* 0.005* 0.333 < 0.001* < 0.001* *P < 0.05。
下载: 导出CSV
表 3 非破裂组 1 的 4D-CTA 和 3D-CTA 辐射剂量 ($\bar x \pm s $)
Table 3. Radiation doses of 4D-CTA and 3D-CTA in non-ruptured group 1 ($\bar x \pm s $)
分组 CTDIvoI(mGy) DLP(mGy·cm) ED(mSv) 4D-CTA (n=50) 53.36±5.02 830.48±77.03 1.85±0.15 3D-CTA (n=50) 66.23±5.03 1181.36±130.52 2.38±0.22 t 12.806 16.371 14.075 P < 0.001* < 0.001* < 0.001* *P < 0.05。
下载: 导出CSV
-
[1] Adeeb N,Griessenauer C J,Dmytriw A A,et al. Risk of branch occlusion and ischemic complications with the pipeline embolization device in the treatment of posterior circulation aneurysms[J]. AJNR Am J Neuro Radiol,2018,39(7):1303-1309. doi: 10.3174/ajnr.A5696 [2] 胡罗健,高凯波,杨明方,等. 16层螺旋CT血管造影对前交通动脉瘤破裂风险因素分析[J]. 实用放射学杂志,2011,27(2):169-172. [3] 黄钟情,周新卫,孟志华,等. 运用CTA分析颅内动脉瘤破裂的危险因素[J]. 临床放射学杂志,2017,36(1):15-19. doi: 10.13437/j.cnki.jcr.2017.01.005 [4] Beck J,Rohde S,el Beltagy M,et al. Difference in configuration of ruptured and unruptured intracranial aneurysms determined by biplanar digital subtraction angiography[J]. Acta Neurochir(Wien),2003,145(10):861-865. doi: 10.1007/s00701-003-0124-0 [5] 徐鹏,陈英,施小燕,等. 3D-CTA 对颅内后循环出血性动脉瘤早期诊断的价值[J]. 中华急诊医学杂志,2020,29(1):127-131. [6] Hallikainen J,Keränen S,Savolainen J,et al. Role of oral pathogens in the pathogenesis of intracranial aneurysm: Review of existing evidence and potential mechanisms[J]. Neurosurg Rev,2021,44(1):239-247. doi: 10.1007/s10143-020-01253-y [7] Sahnoun M,Soize S,Manceau P. Intracranial aneurysm treatment with WEB and adjunctive stent: Preliminary evaluationin a single-center series[J]. Neurointerv Surg,2022,14(2):164-168. doi: 10.1136/neurintsurg-2021-017379 [8] Isoda R,Kanaoka Y,Watanabe T. Total debranching plus antegrade thoracic endovascular aortic repair without side clamping in a patient with arch aneurysm and ascending aorta calcification[J]. Ann Vasc Dis,2021,14(2):181-184. [9] Hayakawa M, Katada K, Anno H, et al. CT angiography with electrocardiographically gated reconstruction for visualizing pulsation of intracranial aneurysms: Identification of aneurysmal protuberancepresumably associated with wallthinning[J] AJNR Am J Neuroradiol, 2005, 26(6): 1366−1369. [10] 马英剑. 3D-CTA 与 3D-DSA 对颅内动脉瘤破裂出血早期诊断价值分析[J]. 中国实用神经疾病杂志,2020,23(9):808-811. [11] 顾艳,胡春洪,徐伦,等. 心电监控四维CT血管成像检测颅内未破裂动脉瘤搏动点及其意义[J]. 中华放射学杂志,2017,51(6):401−406. [12] Saiga A,Koizumi J,Osumi K,et al. Celiac artery dissection and retroperitoneal hemorrhage in median arcuate ligament syndrome treated with a stent and transcatheter arterial embolization: Preprocedural 4-Dimensional computed tomography angiography assessment[J]. Vasc Endovascular Surg,2022,56(1):75-79. doi: 10.1177/15385744211028738 [13] Cui Y,Xing H,Zhou J,et al. Aneurysm morphological prediction of intracranial aneurysm rupture in elderly patients using four-dimensional CT angiography[J]. Clin Neurol Neurosurg,2021,208(2):106877. [14] Cancelliere N M,Najafi M,Brina O,et al. 4D-CT angiography versus 3D-rotational angiography as the imaging modality for computational fluid dynamics of cerebral aneurysms[J]. Neurointerv Surg,2020,12(6):26-30. [15] Zhang J,Li X,Zhao B,et al. Irregular pulsation of intracranial unruptured aneurysm detected by four-dimensional CT angiography is associated with increased estimated rupture risk and conventional risk factors[J]. Neurointerv Surg,2021,13(9):854-858. doi: 10.1136/neurintsurg-2020-016811 [16] Li X,Zhao B,Zhang J,et al. Irregular pulsation of aneurysmal wall is associated with symptomatic and ruptured intracranial aneurysms[J]. Neurointerv Surg,2023,15(1):91-96. doi: 10.1136/neurintsurg-2021-018381 [17] Dhar S,Tremmel M,Mocco J,et al. Morphology parameters for intracranial aneurysm rupture risk assessment[J]. Neurosurgery,2008,63(2):185-196. doi: 10.1227/01.NEU.0000316847.64140.81 [18] Meng H,Feng Y,Woodward S H,et al. Mathematical model of the rupture mechanism of intracranial saccular aneurysms through daughter aneurysm formation and growth[J]. Neurol Res,2005,27(5):459-465. doi: 10.1179/016164105X25171 [19] Cebral J R,Sheridan M,Putman C M. Hemodynamics and bleb formation in intracranial aneurysms[J]. AJNR Am J Neuroradiol,2010,31(2):304-310. doi: 10.3174/ajnr.A1819 [20] Investigators U,Morita A,Kirino T,et al. The natural course of unruptured cerebral aneurysms in a Japanese cohort[J]. New England Journal of Medicine,2012,366(26):2474-2482. doi: 10.1056/NEJMoa1113260 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1472
- HTML全文浏览量: 887
- PDF下载量: 10
- 被引次数: 0
