

Risk Factors of Recurrence in Patients with Ischemic Stroke Treated with Aspirin Single Drug Antiplatelet Therapy
-
摘要:
目的 探讨使用阿司匹林进行单抗二级预防的缺血性卒中患者复发的危险因素。 方法 对200例使用阿司匹林单抗治疗1 a后的轻型和中型缺血性卒中患者进行回顾性的分析,根据患者卒中是否复发分为未复发组和复发组,使用单因素分析和多因素Logistic回归模型分析探讨相关指标是否为复发的高危因素,并利用ROC曲线预测危险因素的临界值。 结果 单因素分析显示有统计学意义的危险因素为血小板计数、同型半胱氨酸水平和PEAR1基因rs12041331位点的A等位基因(P < 0.05)。多因素分析表明复发的独立危险因素为同型半胱氨酸水平[OR = 1.16(1.089~1.240),P < 0.001]。采用ROC预测的临界值为8.35 μmol/L(灵敏度0.847,特异度0.532)。 结论 PEAR1基因rs12041331位点的A等位基因、血小板计数和Hcy水平是导致阿司匹林单抗治疗的缺血性卒中患者复发的危险因素,Hcy水平是导致阿司匹林单抗治疗的缺血性卒中患者复发的独立危险因素,可利用Hcy水平预测阿司匹林单抗治疗的缺血性卒中患者复发的风险。 Abstract: Objective To investigate the risk factors of relapse in patients with ischemic stroke using aspirin for single drug antiplatelet therapy.Methods A retrospective analysis was conducted on 200 patients with mild and medium ischemic stroke after 12 months of single drug treatment with aspirin, and the patients were divided into non-recurrence group and recurrence group according to the recurrence of stroke. Univariate analysis and multivariate logistic regression model were used to explore whether the related indicators were risk factors for recurrence.The ROC curve was used to predict the critical value of risk factors. Results Univariate analysis showed that platelet count, Hcy level and the A allele at rs12041331 site of PEAR1 gene were statistically significant risk factors(P < 0.05). Multifactor analysis showed that the independent risk factor for recurrence was homocysteine level [OR = 1.16(1.089-1.240), P < 0.001)]. The critical value of ROC prediction was 8.35 μmol/L (sensitivity 0.847, specificity 0.532). Conclusions The Hcy level, platelet count and A allele at rs12041331 site of PEAR1 gene are risk factors for recurrence in patients with ischemic stroke treated with aspirin for Single drug antiplatelet therapy.Hcy level is independent risk factor and can be used to predict the risk of recurrence. -
Key words:
- Ischemic stroke /
- Recurrence /
- PEAR1 gene /
- Homocysteine /
- Risk factor
-
表 1 2组间一般资料比较[n(%)/M(P25,P75/($\bar x \pm s$)]
Table 1. Comparision of general data between the two groups [n(%)/M(P25,P75/($ \bar x \pm s $)]
临床指标 未复发组(n = 141) 复发组(n = 59) 检验值(F/Z/χ2) P 年龄(岁) 59.89 ± 12.05 57.8 ± 12.46 0.034 0.268 性别 男 104(73.75) 42(71.19) 0.1396 0.709 女 37(26.25) 17(28.81) 有无吸烟 吸烟 76(53.9) 26(44.07) 1.609 0.205 不吸烟 65(46.1) 33(55.93) 有无饮酒 饮酒 35(24.82) 20(33.90) 1.718 0.190 不饮酒 106(75.18) 39(66.10) 入院时NIHSS评分(分) 轻度(0~4) 109(77.30) 47(79.66) 0.1346 0.714 中度(5~15) 32(22.70) 12(20.34) 入院时ESSEN评分(分) 低危(0~2) 44(31.21) 19(32.20) 0.019 0.890 高危(3~6) 97(68.79) 40(67.80) 凝血功能(INR) 1.01(0.98,1.08) 1.02(0.99,1.07) −0.134 0.509 血小板计数 209.00(166.00~253.00) 220.00(180.00,285.00) −1.559 0.028* 总胆固醇(mmol/L) 3.75(3.00,4.43) 3.78(3.22,4.52) −1.010 0.397 高密度脂蛋(mmol/L) 1.01(0.85,1.23) 1.01(0.84,1.19) 0.820 0.295 低密度脂蛋(mmol/L) 2.18(1.69,2.91) 2.32(1.77,2.89) −1.015 0.315 甘油三脂(mmol/L) 1.49(1.12,2.00) 1.66(1.15,2.21) −1.286 0.332 同型半胱氨酸(μmol/L) 8.20(6.05,11.50) 12.00(9.00,17.00) −5.337 < 0.001* *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 2组间等位基因和基因型分布频率[n(%)]
Table 2. Distribution of allele and genotype frequencies between two groups [n(%)]
等位基因/基因型 未复发组(n = 141) 复发组(n = 59) GG 64(45.39) 17(28.82) GA 60(42.55) 27(45.76) AA 17(12.06) 15(25.42) G 188(66.66) 61(51.69) A 94(33.34) 57(48.31)
下载: 导出CSV
表 3 2组间PEAR1基因rs12041331位点等位基因和基因型分布频率比较(n)
Table 3. Comparison of allele and genotype frequencies between two groups (n)
等位基因/基因型 未复发组(n = 141) 复发组(n = 59) P OR(95%CI) Ga 188 61 0.007* 1.869(1.206~2.896) A 94 57 GGa 64 17 0.040* 2.053(1.068~3.949) GA+AA 77 42 GG+GAa 124 44 0.033* 2.487(1.146~5.398) AA 17 15 a:参照等位基因/基因型;*P < 0.05。
下载: 导出CSV
表 4 复发风险因素的多因素Logistic回归分析
Table 4. Logistic regression analysis for relevant indicators in risk factors for recurrence
指标 回归系数 标准误 统计量 OR 95%CI P 血小板计数 0.004 0.002 3.347 1.004 1.000~1.008 0.067 同型半胱氨酸 0.150 0.033 20.469 1.162 1.089~1.240 < 0.001* *P < 0.05。
下载: 导出CSV
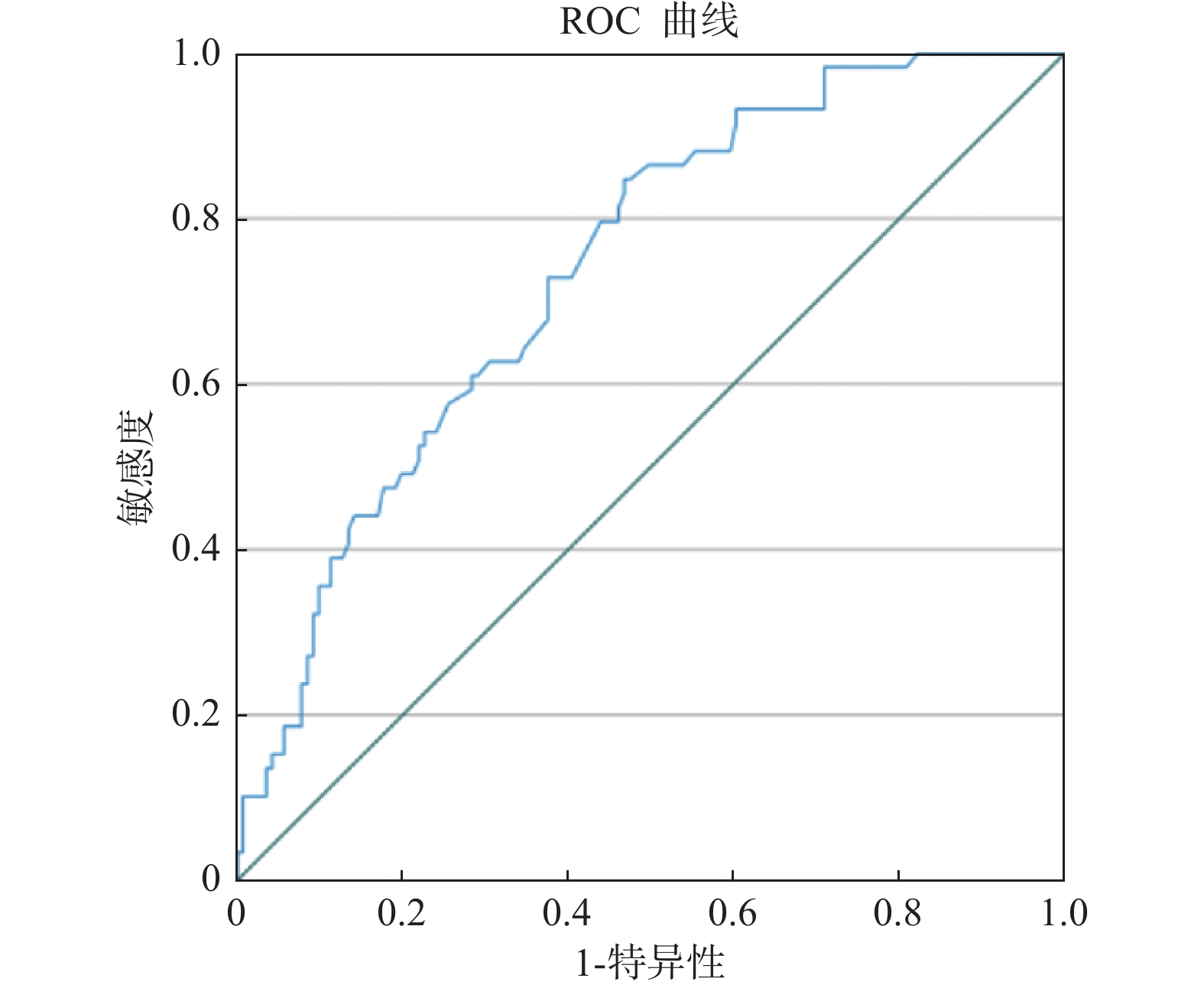
表 5 同型半胱氨酸对复发风险的预测价值
Table 5. The predictive value of homocysteine level on the risk of recurrence
危险因素 临界值 灵敏度 特异度 Youden指数 AUC(95%CI) P 同型半胱氨酸 8.35 0.847 0.532 0.379 0.711(0.668~0.810) < 0.001
下载: 导出CSV
-
[1] 中华医学会神经病学分会,中华医学会神经病学分会脑血管病学组. 中国缺血性卒中和短暂性脑缺血发作二级预防指南2022[J]. 中华神经科杂志,2022,55(10):1071. doi: 10.3760/cma.j.cn113694-20220714-00548 [2] 诸葛瑞琪,刘梅林. 阿司匹林用于心血管疾病一级预防的进展[J]. 中国心血管杂志,2022,27(3):211. [3] Alberts M J,Bergman D L,Molner E,et al. Antiplatelet effect of aspirin in patients with cerebrovascular disease[J]. Stroke,2004,35(1):175. doi: 10.1161/01.STR.0000106763.46123.F6 [4] Kasotakis G,Pipinos II,Lynch T G. Current evidence and clinical implications of aspirin resistance[J]. J Vasc Surg,2009,50(6):1500. doi: 10.1016/j.jvs.2009.06.023 [5] Haines J M,Lee P M,Hegedus R M,et al. Investigation into the causes of aspirin resistance in healthy dogs[J]. J Vet Pharmacol Ther,2019,42(2):160. doi: 10.1111/jvp.12725 [6] Meirhaeghe A,Cottel D,Cousin B,et al. Sex differences in stroke attack,incidence,and mortality rates in northern France[J]. J Stroke Cerebrovasc,2018,27(5):1368. doi: 10.1016/j.jstrokecerebrovasdis.2017.12.023 [7] 朱筱琦,陆学胜. 急性复发性脑梗死患者发生阿司匹林抵抗的相关性分析[J]. 中国药房,2016,27(9):1194. [8] 孟文超,高美景,王立羽. 阿托伐他汀治疗老年缺血性卒中合并高脂血症患者的疗效与安全性[J]. 中国循证心血管医学杂志,2017,9(6):700. [9] 赵楠楠,郑印,黄穹琼,等. 急性缺血性脑卒中早期预后不良的危险因素分析及预测模型构建[J]. 中国临床研究,2022,35(4):456. [10] Lewis J P,Riaz M,Xie S,et al. Genetic variation in PEAR1,cardiovascular outcomes and effects of Aspirin in a healthy elderly population[J]. Clin Pharmacol Ther,2020,108(6):1289. doi: 10.1002/cpt.1959 [11] Faraday N,Yanek L R,Yang X P,et al. Identification of a specific intronic PEAR1 gene variant associated with greater platelet aggregability and protein expression[J]. Blood,2011,118(12):3367. doi: 10.1182/blood-2010-11-320788 [12] 李建设,孟轲,赵剑婷,等. PEAR1基因多态性对长期服用阿司匹林脑梗死患者复发的影响[J]. 中国实用神经疾病杂志,2017,20(20):26. [13] Lewis J P,Ryan K,O'Connell J R,et al. Genetic variation in PEAR1 is associated with platelet aggregation and cardiovascular outcomes[J]. Circ Cardiovasc Genet,2013,6(2):184. doi: 10.1161/CIRCGENETICS.111.964627 [14] 张鸥,刘洋,蒙航娟,等. 血浆同型半胱氨酸水平与脑卒中关系研究进展[J]. 中国公共卫生,2021,37(12):1840. [15] Shi Z,Liu S,Guan Y,et al. Changes in total homocysteine levels after acute stroke and recurrence of stroke[J]. Sci Rep-UK,2018,8(1):6993. doi: 10.1038/s41598-018-25398-5 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1473
- HTML全文浏览量: 1009
- PDF下载量: 18
- 被引次数: 0
