

Identification of Atrial Fibrillation-related Inflammatory Genes and Their Association with Immune Cell Infiltration Based on Comprehensive Bioinformatic Analysis
-
摘要:
目的 鉴定心房颤动 ( atrial fibrillation,AF)患者的炎症相关基因,并探讨这些基因与浸润免疫细胞在AF的发生发展过程中可能的作用和机制。 方法 通过一系列的生物信息学分析结合机器学习算法识别AF的生物标志物,使用受试者操作特性曲线(receiver operating characteristic,ROC)验证关键基因的预测及诊断价值,采用Spearman 相关分析明确关键基因与浸润免疫细胞的相关性。 结果 筛选出593个差异基因[|log2 (fold change,FC)|>1,P<0.05],7种免疫细胞亚型(P<0.05),获得190个免疫相关差异基因,识别出 3 个生物标志物(IGF1、PTGS2和PPARG),相关性分析结果显示3个标志物与浸润免疫细胞显著相关(P<0.05)。 结论 IGF1、PTGS2和PPARG是AF的炎症相关基因,推测其与免疫细胞浸润过程和途径密切相关。 Abstract:Objective To identify inflammation-related genes in atrial fibrillation (AF) and explore the possible role and mechanism of these genes and infiltrating immune cells in the development of AF. Methods A series of bioinformatics analysis combined with machine learning algorithms to identify biomarkers of AF, the receiver operating characteristic (ROC) curves were used to verify the prediction and diagnostic value of key genes, and Spearman correlation analysis was used to clarify the correlation between key genes and infiltrating immune cells. Results 593 differential genes (| log2 (fold change, FC) |> 1, P <0.05), 7 immune cell subtypes (P <0.05) were selected, 190 immune-related differential genes were obtained, 3 biomarkers (IGF1, PTGS 2 and PPARG), and the correlation analysis showed that 3 markers were significantly associated with infiltrating immune cells (P < 0.05). Conclusion IGF1, PTGS2 and PPARG are inflammation-related genes of AF, which are speculated to be closely related to the process and pathway of immune cell infiltration. -
Key words:
- Atrial fibrillation /
- Bioinformatics analysis /
- Immune infiltration /
- Inflammatory response /
- Biomarkers
-
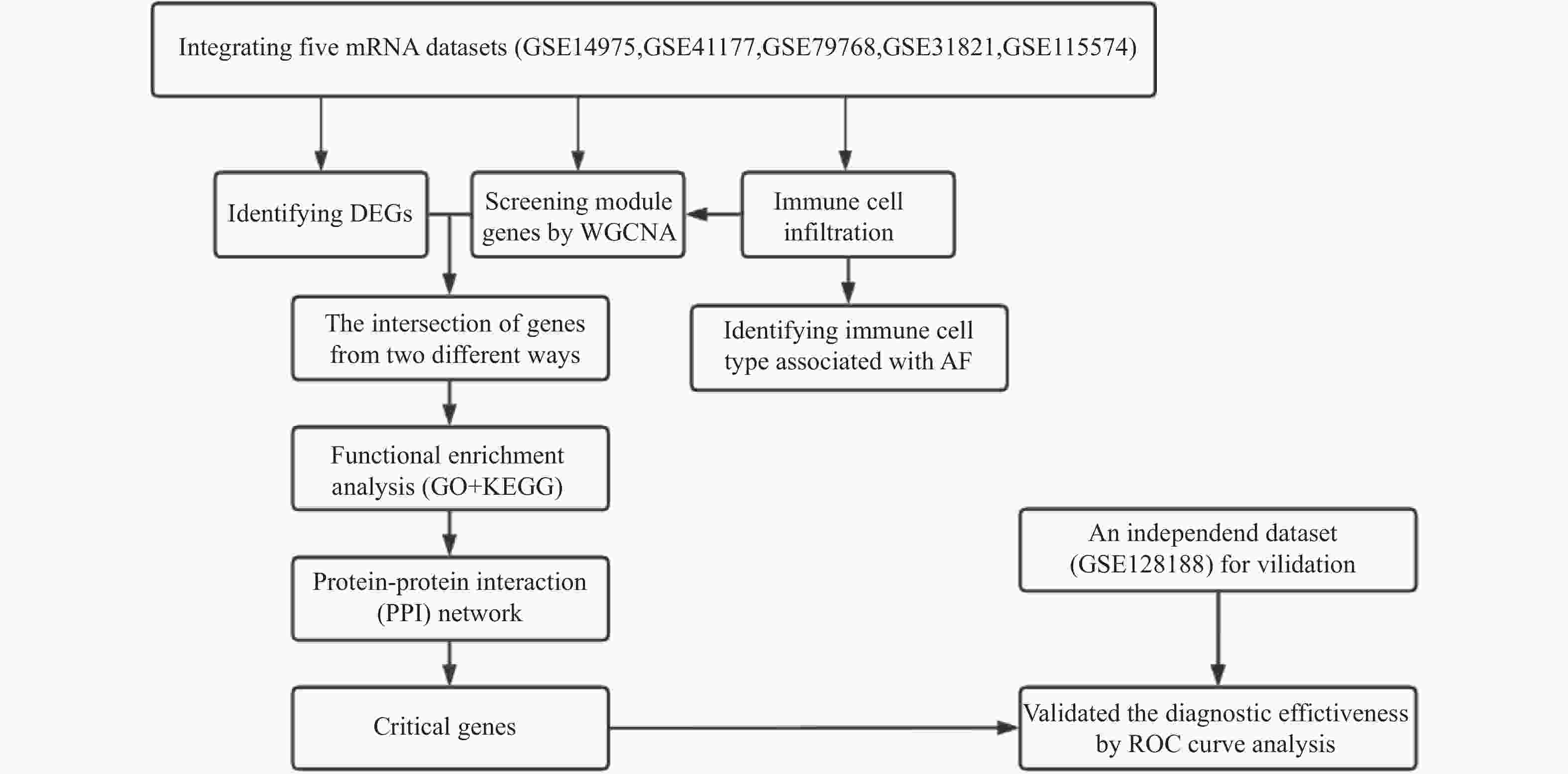
图 1 生物信息学分析的流程图
DEGs:差异表达基因;WGCNA:加权基因共表达网络分析; GO:基因本体论;KEGG:京都基因和基因组百科全书;PPI:蛋白质-蛋白质相互作用;ROC:受试者操作特性曲线。
Figure 1. Flow diagram of the bioinformatics analysis
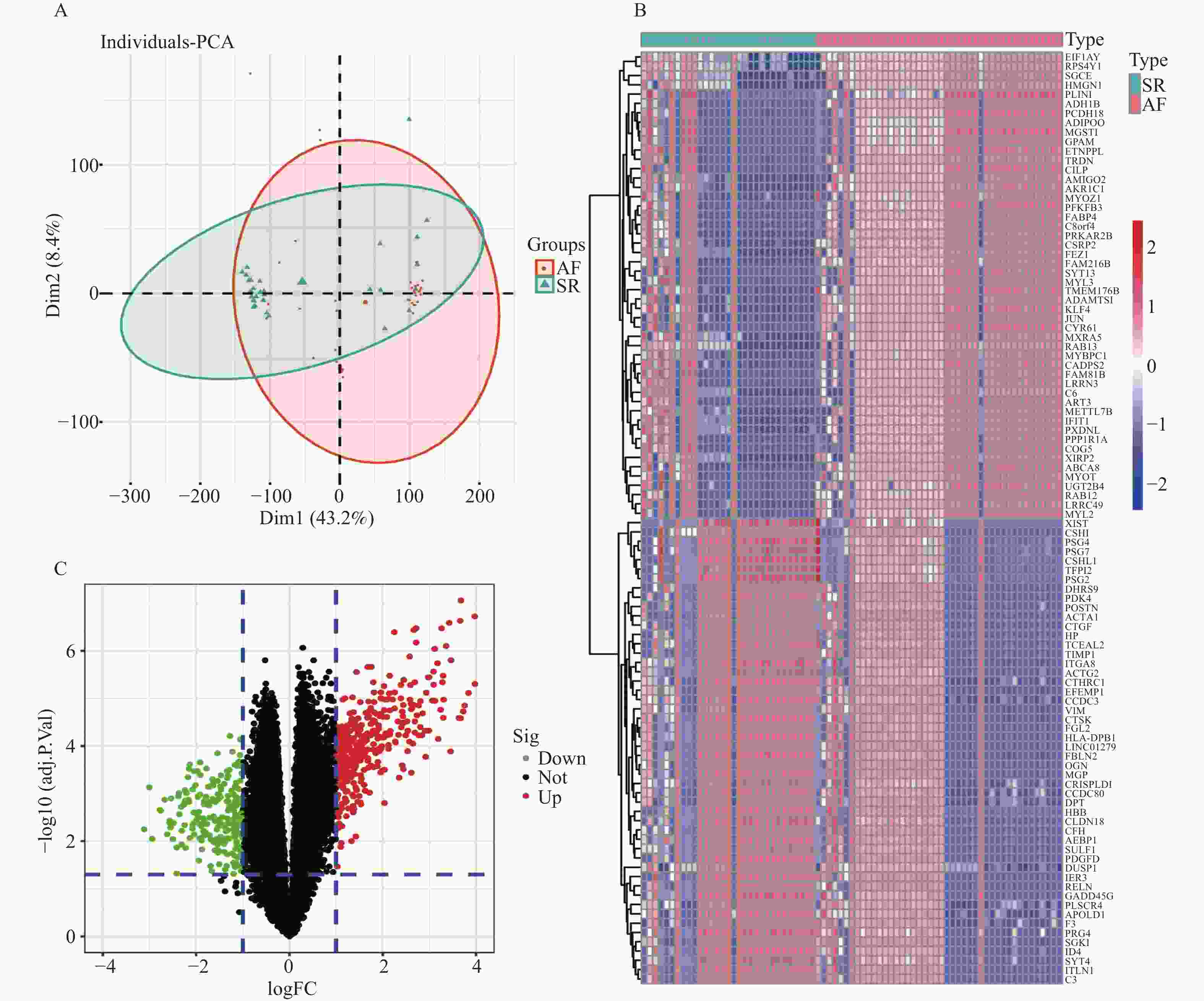
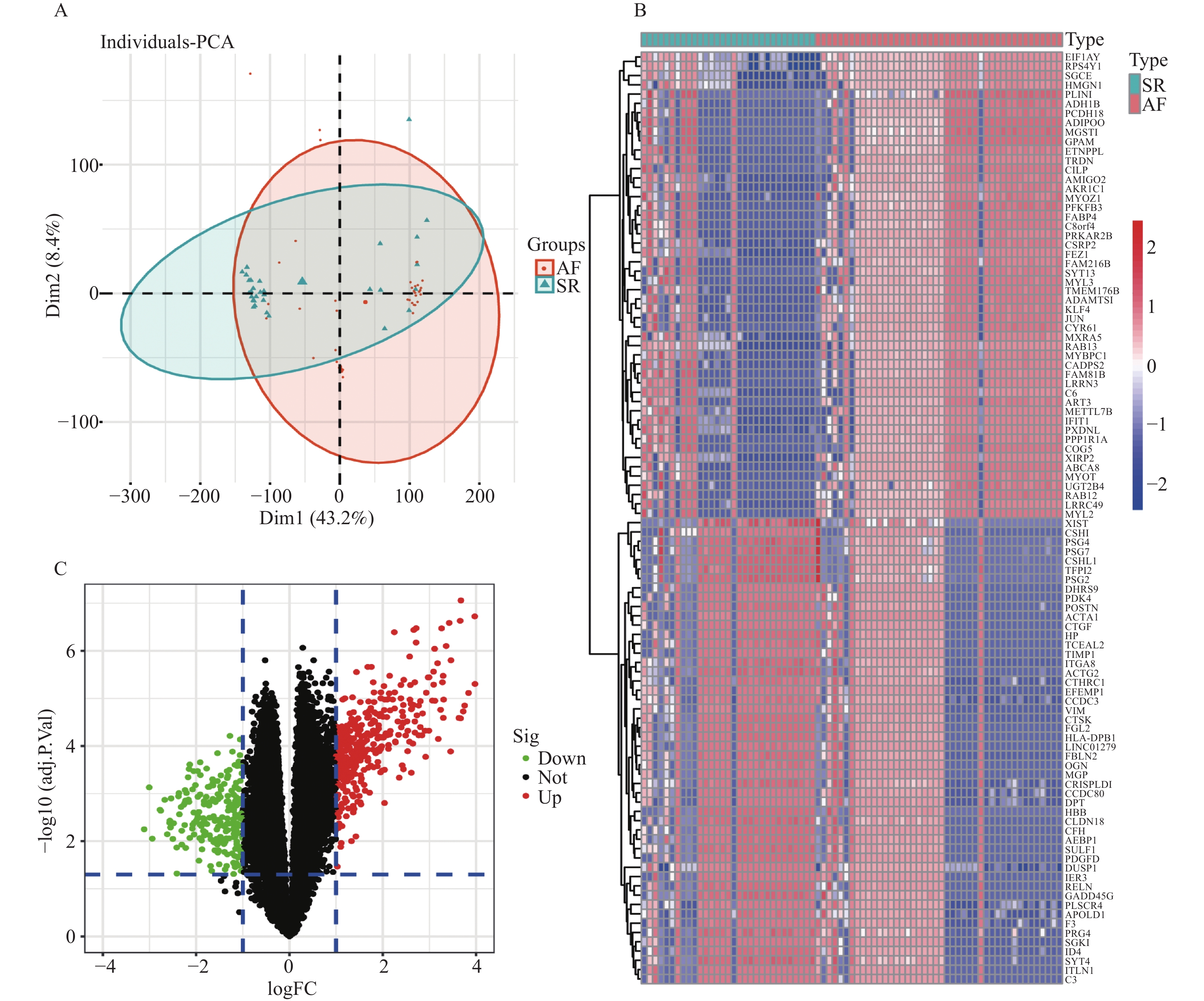
图 2 AF和SR样本组间的DEGs鉴定
A:去除批次效应后AF和SR组间的PCA图;B:前50个DEGs的热图;C:DEGs的火山图。
Figure 2. Identification of DEGs between AF and SR samples

图 3 免疫细胞浸润的分布和相关性
A:22种免疫细胞亚型的分布相对百分比;B:SR和AF组间22种免疫细胞亚型的浸润分数;C:22种免疫细胞亚型组成的相关矩阵。
Figure 3. Distribution and correlation of immune cell infiltration
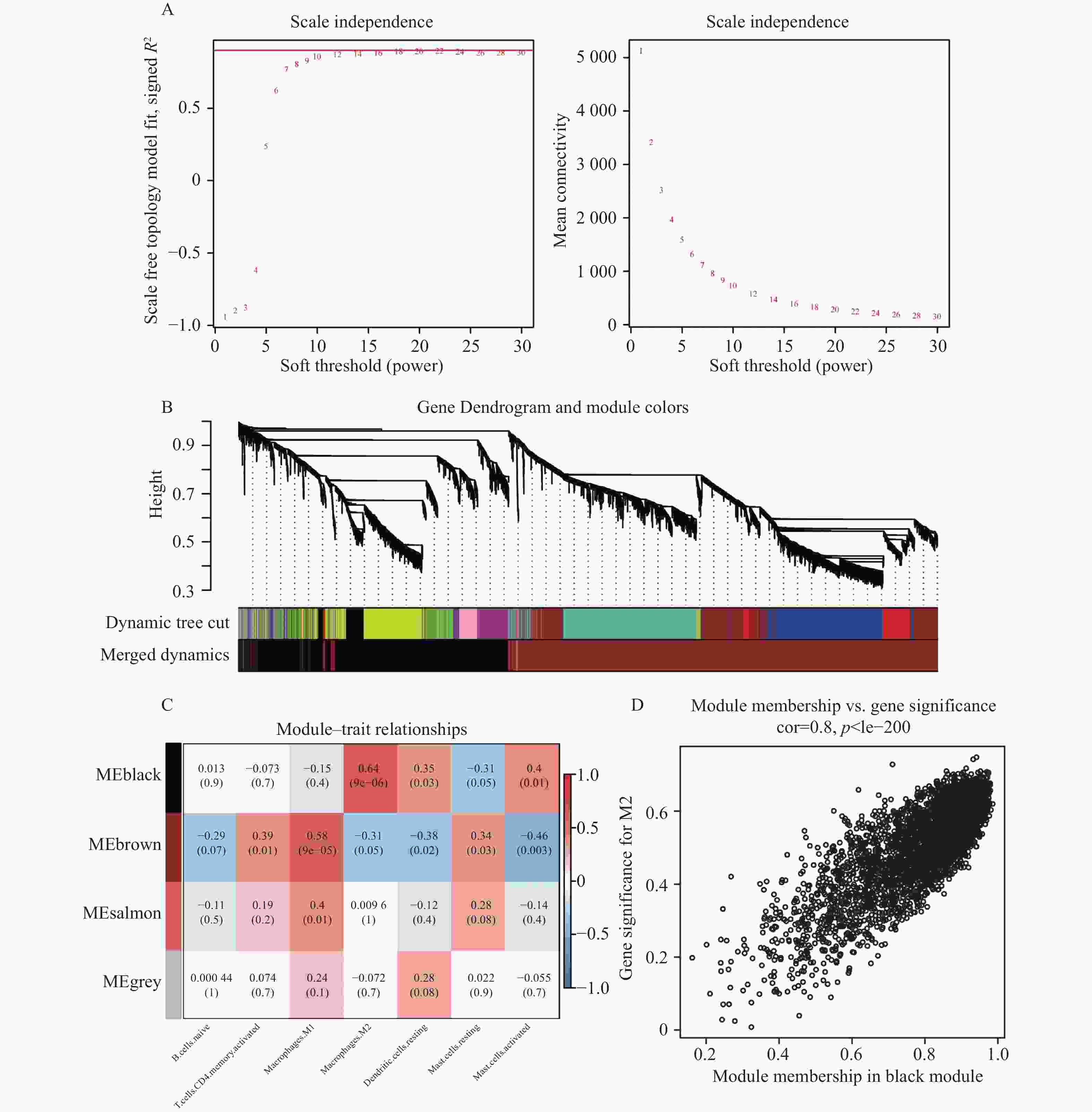
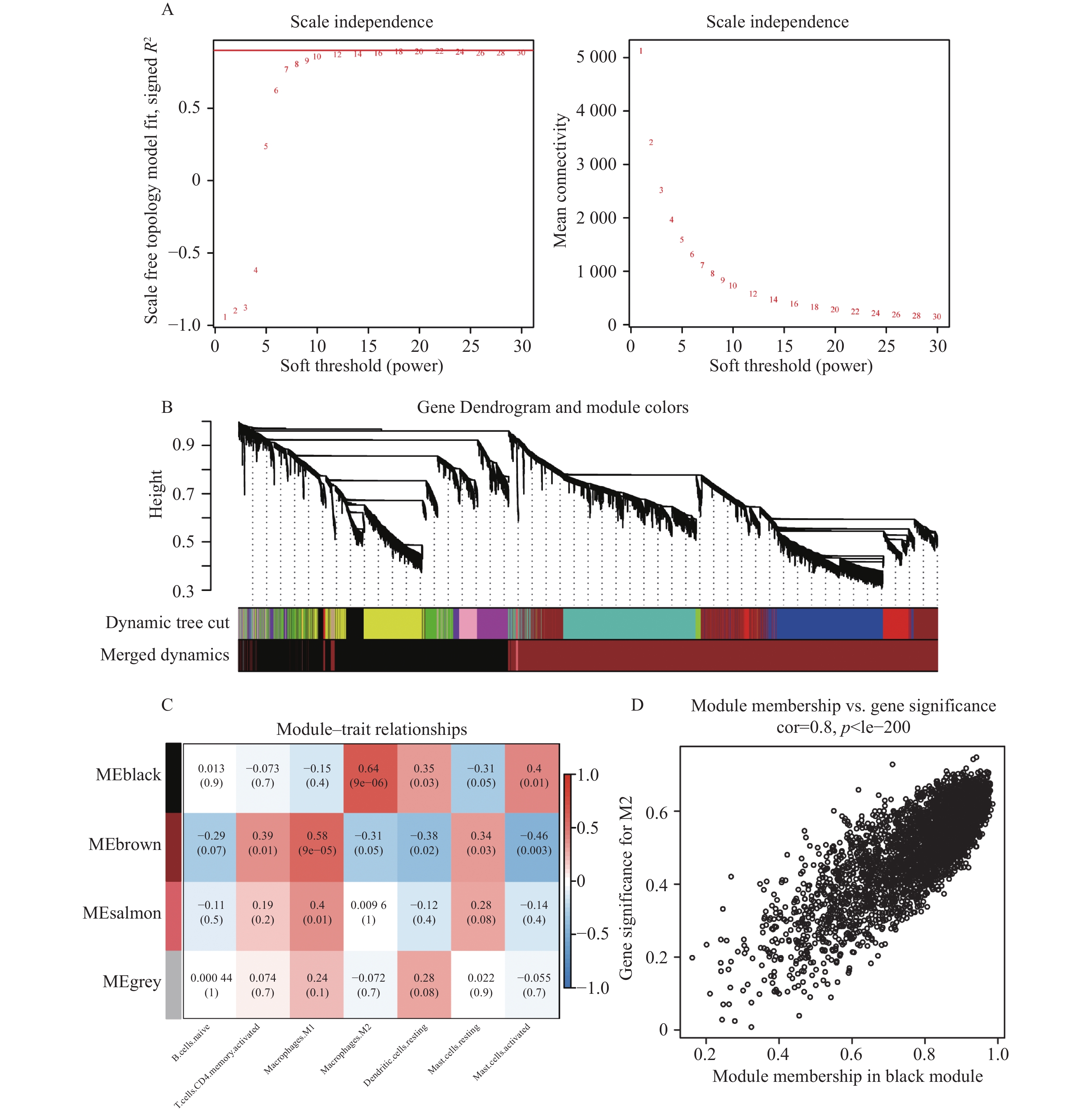
图 4 WGCNA分析
A:无尺度分布网络的软阈值选择(β=10);B:WGCNA网络模块分类(mergeCutHeight=0.25);C:4种模块与7种免疫细胞亚型之间关联的热图;D:黑色模块与M2巨噬细胞之间的相关性散点图。
Figure 4. WGCNA analysis

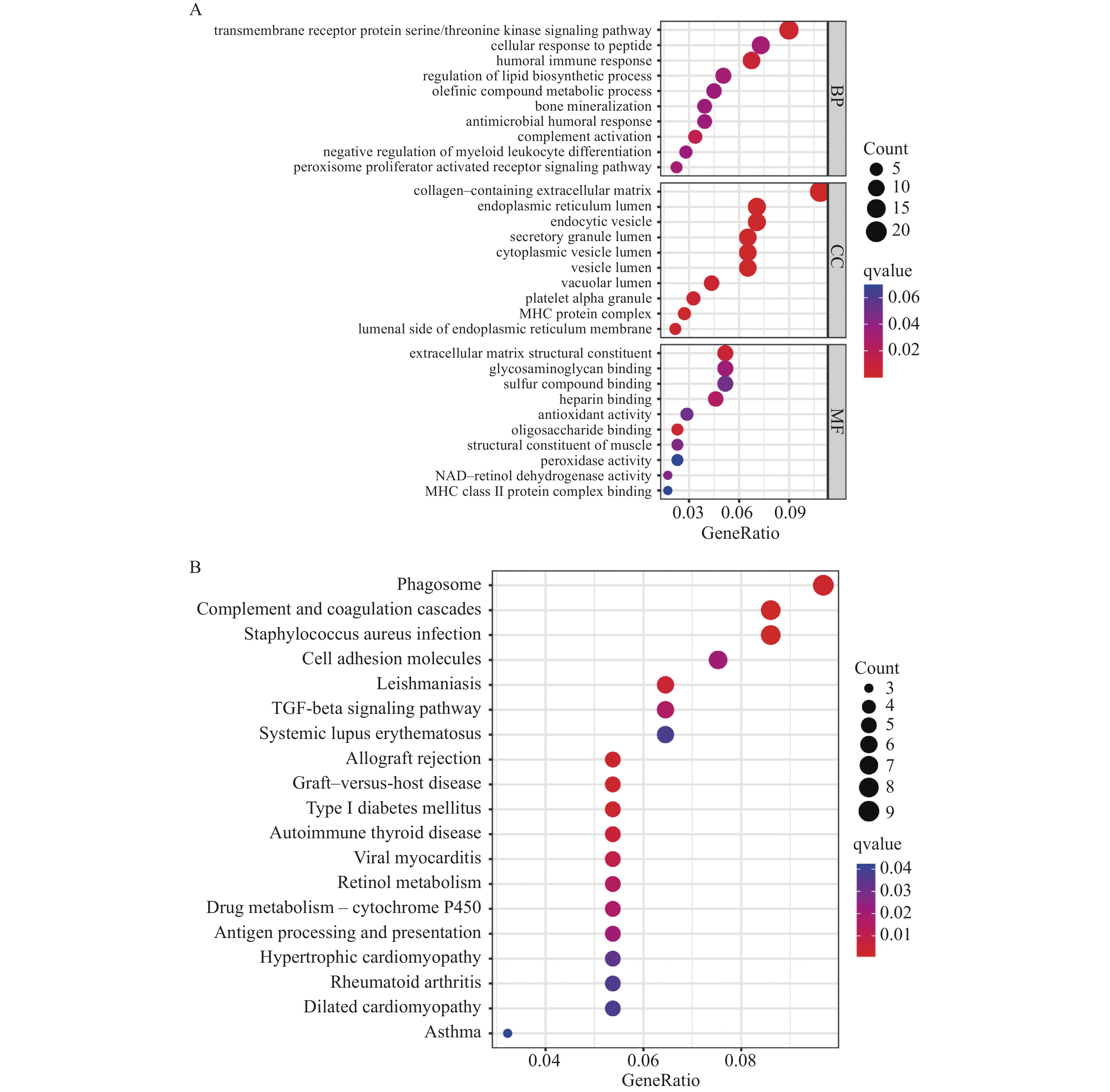
图 5 DEIRGs的GO和KEGG功能富集分析
A:GO分析气泡图;B:KEGG分析气泡图。
Figure 5. GO and KEGG functional enrichment analysis of the DEIRGs
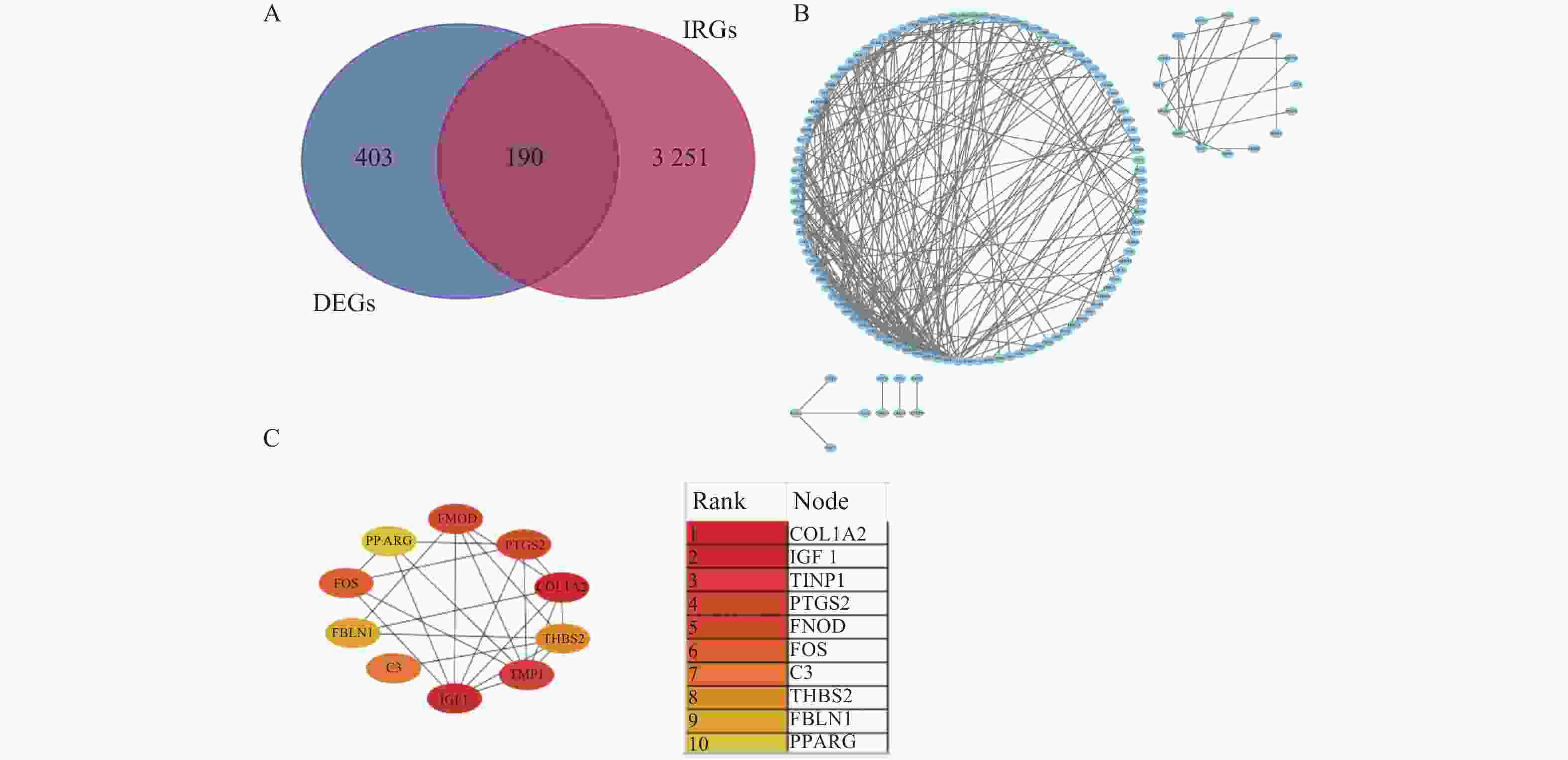
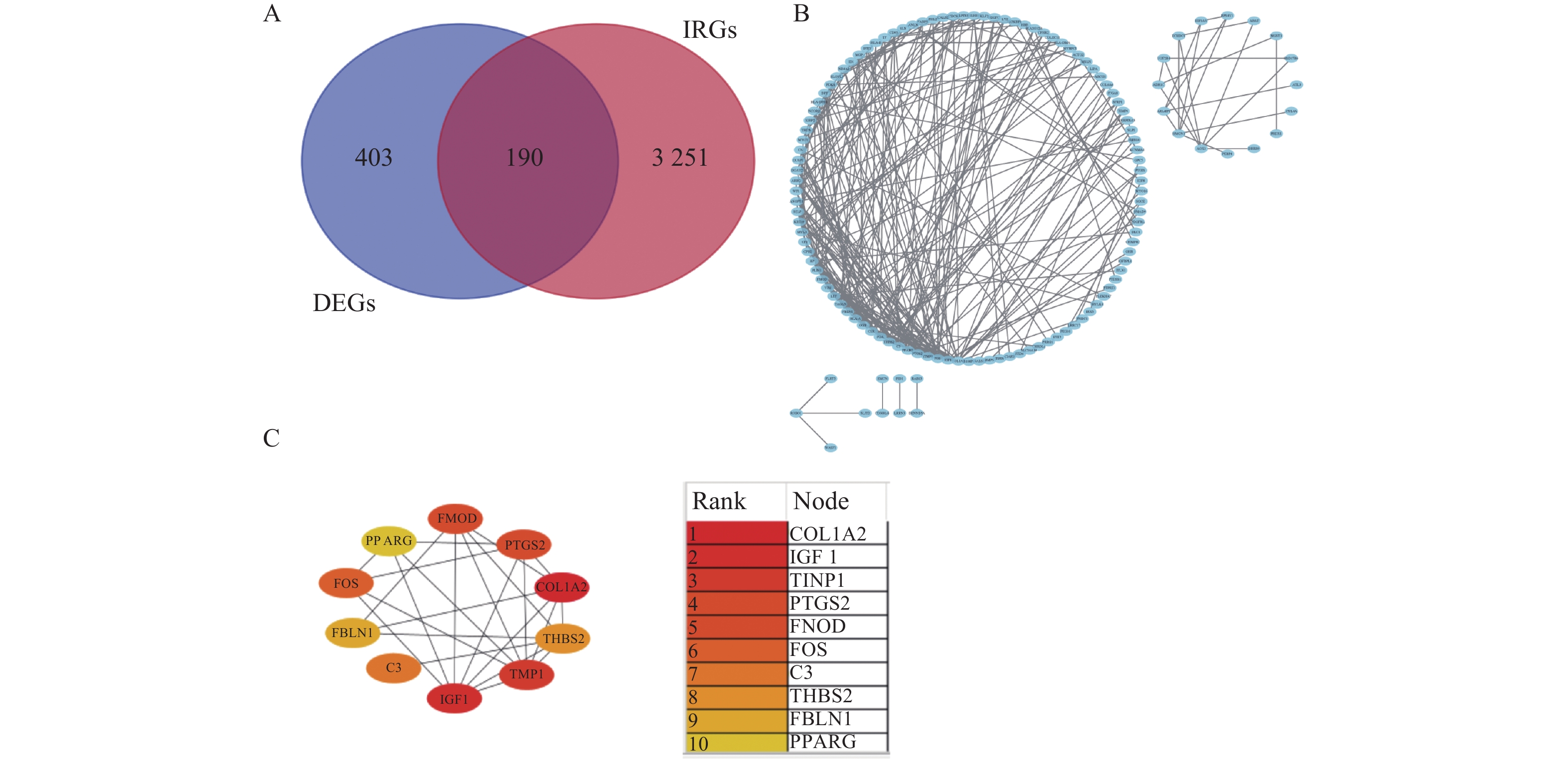
图 6 PPI网络筛选候选基因
A:DEGs与IRGs交集的韦恩图;B:PPI网络图;C:10个候选基因相关性及排名。
Figure 6. PPI network screening for candidate genes
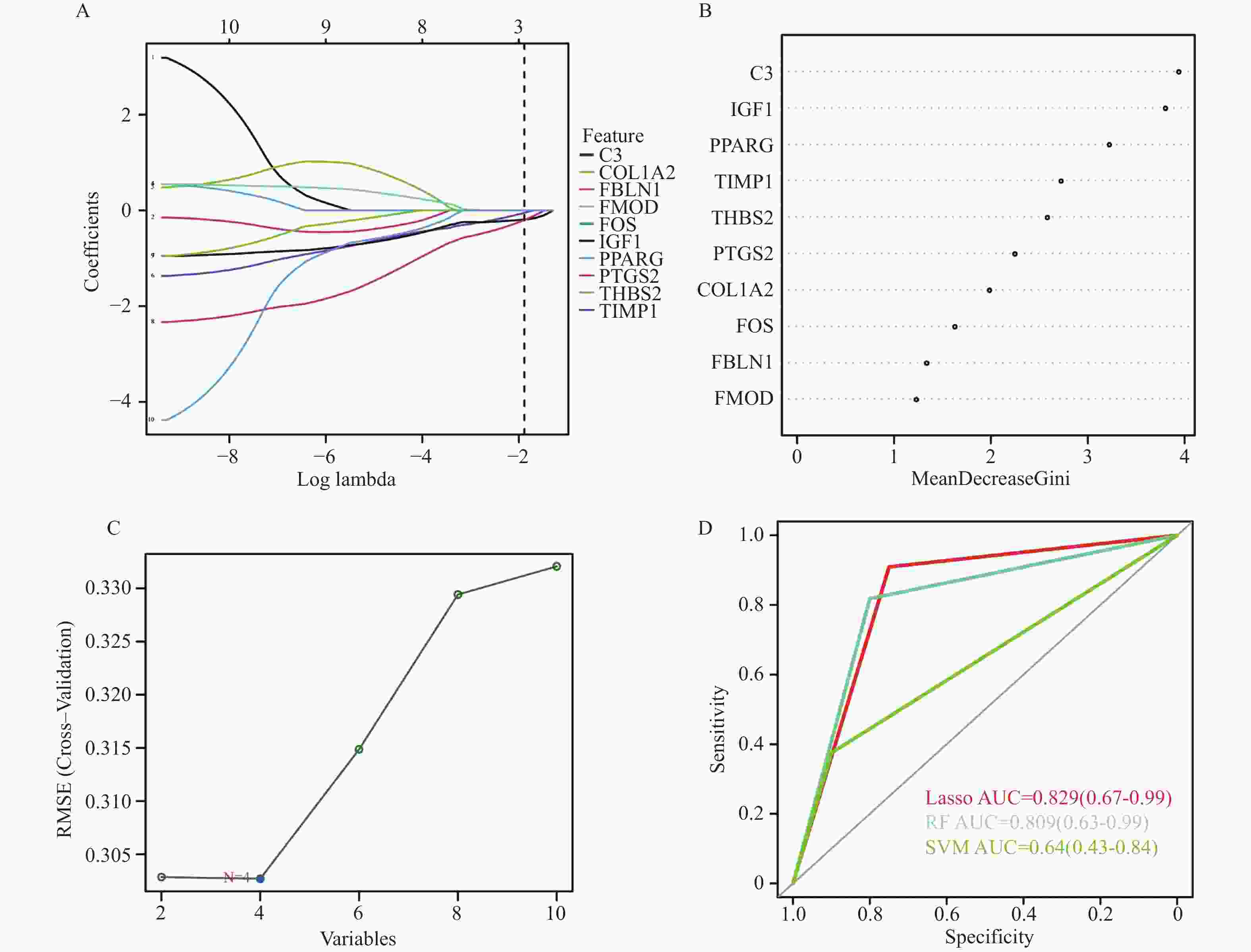
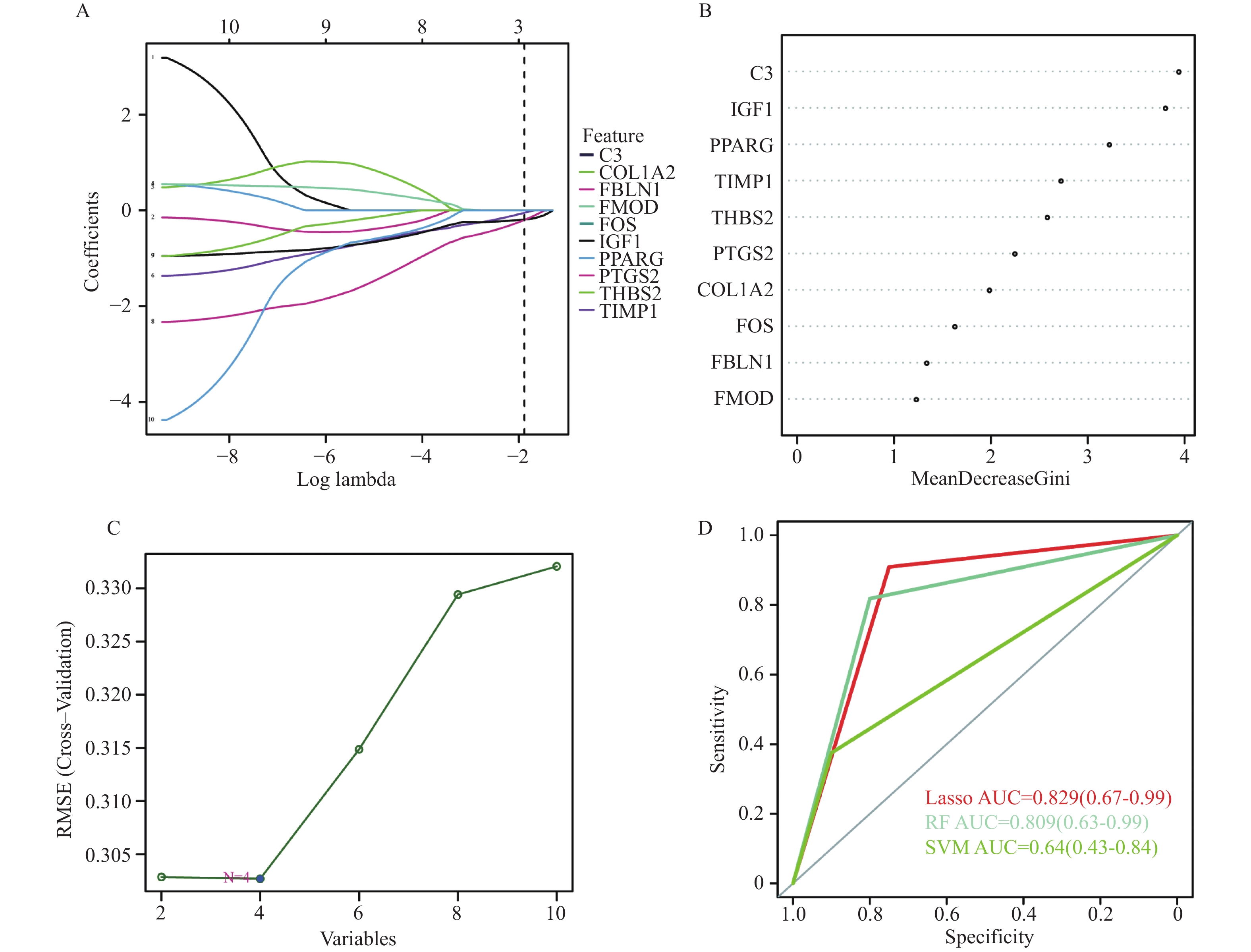
图 7 机器学习算法识别 AF 生物标志物
A:LASSO;B:RF;C:SVM-RFE;D:3种预测模型ROC曲线比较。
Figure 7. Machine learning algorithm identifies AF biomarkers
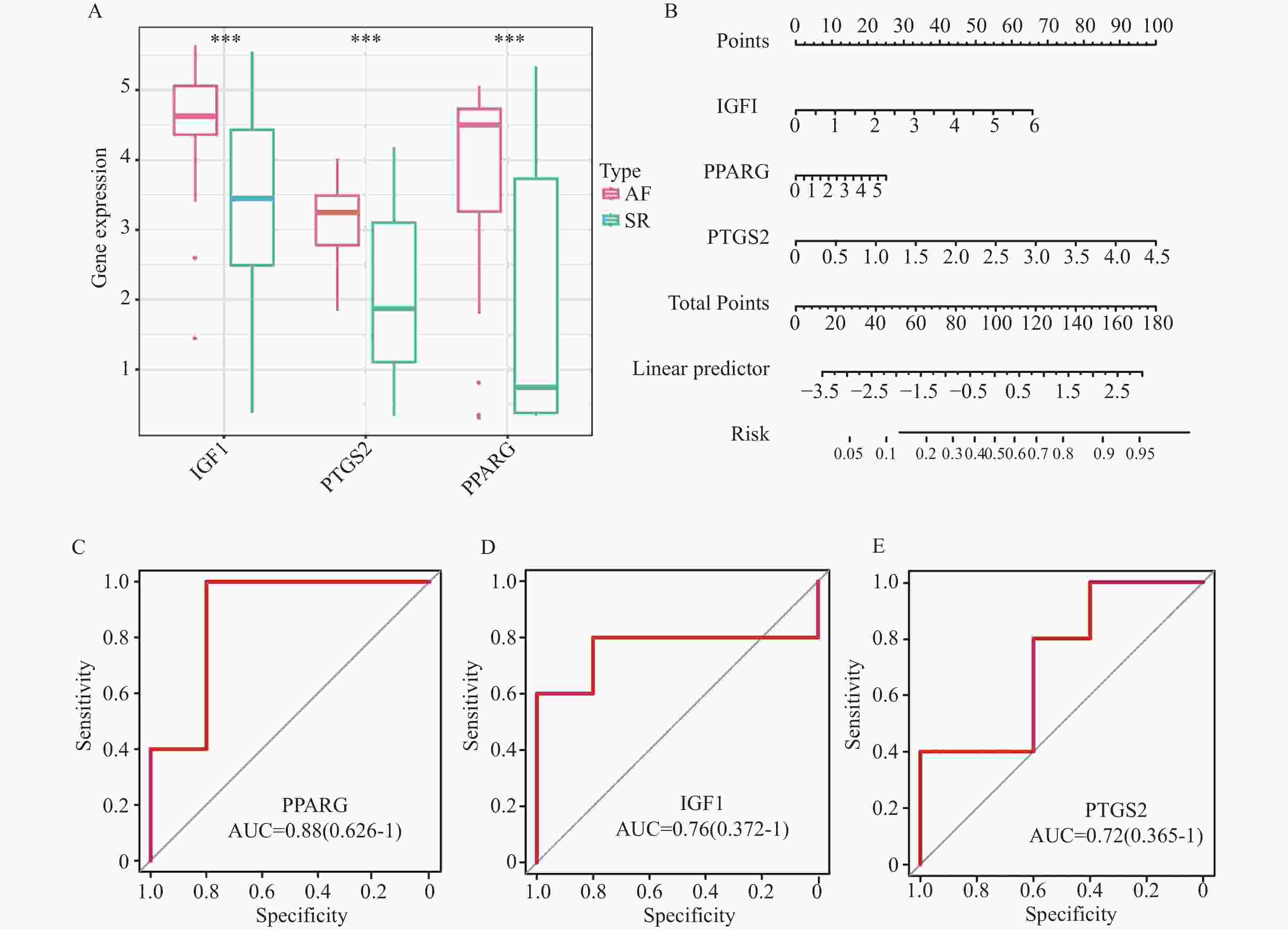
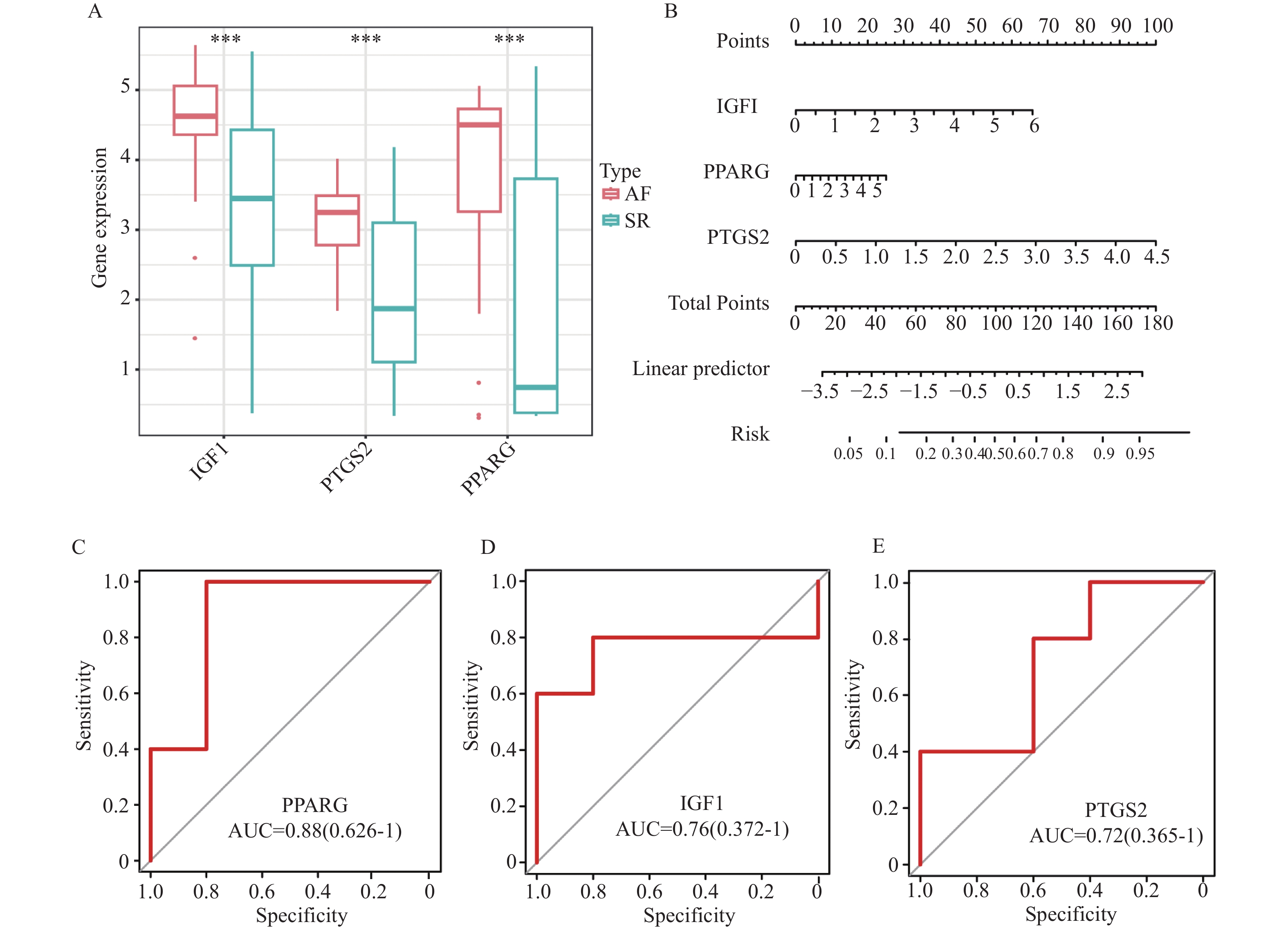
图 8 生物标志物的诊断及预测效能
A:3个关键基因在AF和SR组间的差异表达箱线图;B:诊断模型的列线图;C~E:ROC曲线验证3个关键基因在外部数据集中的诊断有效性。***P<0.001。
Figure 8. Diagnostic and predictive efficacy of the biomarkers
-
[1] Zhu Y,Shi J,Zheng B,et al. Genetic findings in patients with primary fibrotic atrial cardiomyopathy[J]. European Journal of Medical Genetics,2022,65(3):104429. doi: 10.1016/j.ejmg.2022.104429 [2] Litviňuková M,Talavera-López C,Maatz H,et al. Cells of the adult human heart[J]. Nature,2020,588(7838):466-472. doi: 10.1038/s41586-020-2797-4 [3] Zaidi Y, Aguilar E G, Troncoso M, et al. Immune regulation of cardiac fibrosis post myocardial infarction. [Z]. 2021: 77, 109837. [4] Tian Y,Liu S,Zhang Y,et al. Immune infiltration and immunophenotyping in atrial fibrillation[J]. Aging (Albany NY),2023,15(1):213-229. doi: 10.18632/aging.204470 [5] Wynn T A,Vannella K M. Macrophages in tissue repair,regeneration,and fibrosis[J]. Immunity,2016,44(3):450-462. doi: 10.1016/j.immuni.2016.02.015 [6] Newman A M,Liu C L,Green M R,et al. Robust enumeration of cell subsets from tissue expression profiles[J]. Nat Methods,2015,12(5):453-457. doi: 10.1038/nmeth.3337 [7] Langfelder P,Horvath S. WGCNA: An R package for weighted correlation network analysis[J]. BMC Bioinformatics,2008,9(1):559. doi: 10.1186/1471-2105-9-559 [8] Liu Y, Shi Q, Ma Y, et al. The role of immune cells in atrial fibrillation[J]. J Mol Cell Cardiol, 2018: 123, 198-208. [9] Zhang Y L,Teng F,Han X,et al. Selective blocking of CXCR2 prevents and reverses atrial fibrillation in spontaneously hypertensive rats[J]. J Cell Mol Med,2020,24(19):11272-11282. doi: 10.1111/jcmm.15694 [10] Hulsmans M,Schloss M J,Lee I H,et al. Recruited macrophages elicit atrial fibrillation[J]. Science,2023,381(6654):231-239. doi: 10.1126/science.abq3061 [11] Grune J,Yamazoe M,Nahrendorf M. Electroimmunology and cardiac arrhythmia[J]. Nature reviews cardiology,2021,18(8):547-564. doi: 10.1038/s41569-021-00520-9 [12] Sun Z,Zhou D,Xie X,et al. Cross-talk between macrophages and atrial myocytes in atrial fibrillation[J]. Basic Res Cardiol,2016,111(6):63. doi: 10.1007/s00395-016-0584-z [13] Bosco M C. Macrophage polarization: reaching across the aisle?[J]. J Allergy Clin Immunol,2019,143(4):1348-1350. doi: 10.1016/j.jaci.2018.12.995 [14] Wen S,Yan W,Wang L. mRNA expression disturbance of complement system related genes in acute arterial thrombotic and paroxysmal atrial fibrillation patients[J]. Ann Palliat Med,2020,9(3):835-846. doi: 10.21037/apm.2020.04.18 [15] Liu L,Zheng Q,Lee J,et al. PD-1/PD-L1 expression on CD(4+) T cells and myeloid DCs correlates with the immune pathogenesis of atrial fibrillation[J]. J Cell Mol Med,2015,19(6):1223-1233. doi: 10.1111/jcmm.12467 [16] Cheng W L,Kao Y H,Chen Y C,et al. Macrophage migration inhibitory factor increases atrial arrhythmogenesis through CD74 signaling[J]. Transl Res,2020,216:43-56. doi: 10.1016/j.trsl.2019.10.002 [17] Chen Y,Fu L,Pu S,et al. Systemic lupus erythematosus increases risk of incident atrial fibrillation: A systematic review and meta-analysis[J]. Int J Rheum Dis,2022,25(10):1097-1106. doi: 10.1111/1756-185X.14403 [18] Kunamalla A,Ng J,Parini V,et al. Constitutive expression of a dominant-negative TGF-β type II receptor in the posterior left atrium leads to beneficial remodeling of atrial fibrillation substrate[J]. Circ Res,2016,119(1):69-82. doi: 10.1161/CIRCRESAHA.115.307878 [19] Liang Y,Zhou Y,Wang J,et al. Downregulation of fibromodulin attenuates inflammatory signaling and atrial fibrosis in spontaneously hypertensive rats with atrial fibrillation via inhibiting TLR4/NLRP3 signaling pathway[J]. Immun Inflamm Dis,2023,11(10):e1003. doi: 10.1002/iid3.1003 [20] Gao L,Kan C,Chen X,et al. Mechanism of action of Zhi Gan Cao decoction for atrial fibrillation and myocardial fibrosis in a mouse model of atrial fibrillation: A network pharmacology-based study[J]. Comput Math Methods Med,2022,2022:4525873. [21] Raman K,Aeschbacher S,Bossard M,et al. Whole blood gene expression differentiates between atrial fibrillation and sinus rhythm after cardioversion[J]. PLoS One,2016,11(6):e157550. [22] Troncoso R,Ibarra C,Vicencio J M,et al. New insights into IGF-1 signaling in the heart[J]. Trends Endocrinol Metab,2014,25(3):128-137. doi: 10.1016/j.tem.2013.12.002 [23] Fujita M,Takada Y K,Takada Y. Insulin-like growth factor (IGF) signaling requires αvβ3-IGF1-IGF type 1 receptor (IGF1R) ternary complex formation in anchorage independence,and the complex formation does not require IGF1R and Src activation[J]. J Biol Chem,2013,288(5):3059-3069. doi: 10.1074/jbc.M112.412536 [24] Zhao Z,Li R,Wang X,et al. Attenuation of atrial remodeling by aliskiren via affecting oxidative stress,inflammation and PI3K/Akt signaling pathway[J]. Cardiovasc Drugs Ther,2021,35(3):587-598. doi: 10.1007/s10557-020-07002-z [25] Cheng W,Zhu Y,Wang H. The MAPK pathway is involved in the regulation of rapid pacing-induced ionic channel remodeling in rat atrial myocytes[J]. Mol Med Rep,2016,13(3):2677-2682. doi: 10.3892/mmr.2016.4862 [26] Dalli J,Chiang N,Serhan C N. Elucidation of novel 13-series resolvins that increase with atorvastatin and clear infections[J]. Nat Med,2015,21(9):1071-1075. doi: 10.1038/nm.3911 [27] Kim S F,Huri D A,Snyder S H. Inducible nitric oxide synthase binds,S-nitrosylates,and activates cyclooxygenase-2[J]. Science,2005,310(5756):1966-1970. doi: 10.1126/science.1119407 [28] Wang Z,Zeng Z,Hu Y,et al. Network pharmacology and pharmacological mechanism of CV-3 in atrial fibrillation[J]. Evid Based Complement Alternat Med,2022,2022:5496299. [29] Barroso I,Gurnell M,Crowley V E,et al. Dominant negative mutations in human PPARgamma associated with severe insulin resistance,diabetes mellitus and hypertension[J]. Nature,1999,402(6764):880-883. doi: 10.1038/47254 [30] Park S H,Choi H J,Yang H,et al. Endoplasmic reticulum stress-activated C/EBP homologous protein enhances nuclear factor-kappaB signals via repression of peroxisome proliferator-activated receptor gamma[J]. J Biol Chem,2010,285(46):35330-35339. doi: 10.1074/jbc.M110.136259 [31] Chen Y L, Chuang J H, Wang H T, et al. Altered expression of circadian clock genes in patients with atrial fibrillation is associated with atrial high-rate episodes and left atrial remodeling[J]. Diagnostics (Basel), 2021, 11(1): 90. [32] Wang N,Yang G,Jia Z,et al. Vascular PPARgamma controls circadian variation in blood pressure and heart rate through Bmal1[J]. Cell Metab,2008,8(6):482-491. doi: 10.1016/j.cmet.2008.10.009 -

 下载:
下载:

 点击查看大图
点击查看大图

计量
- 文章访问数: 1866
- HTML全文浏览量: 901
- PDF下载量: 38
- 被引次数: 0
