

Value of Multimodal Ultrasonography Combined with Clinical Indicators in Predicting the Progression of Ischemic Stroke
-
摘要:
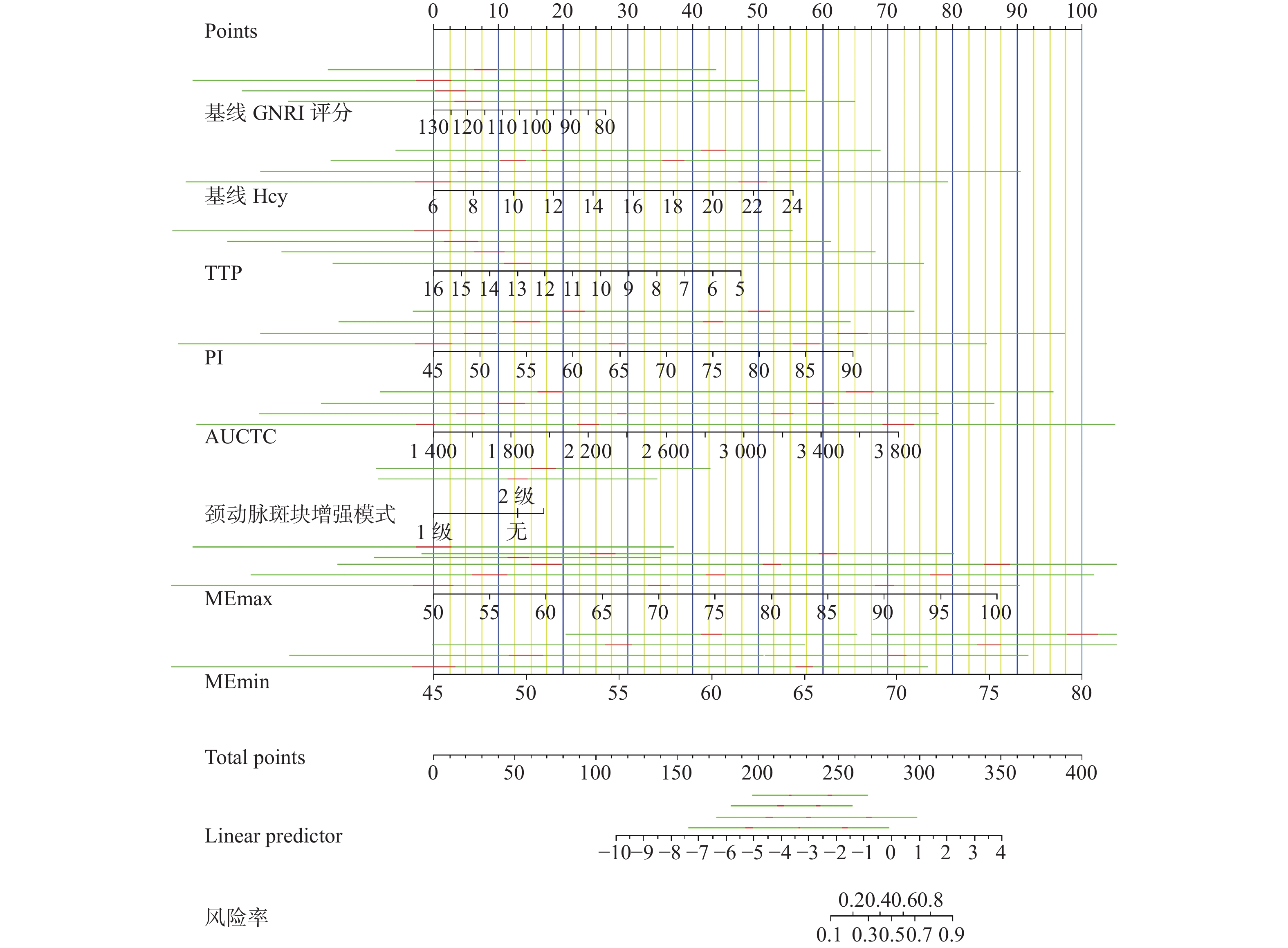
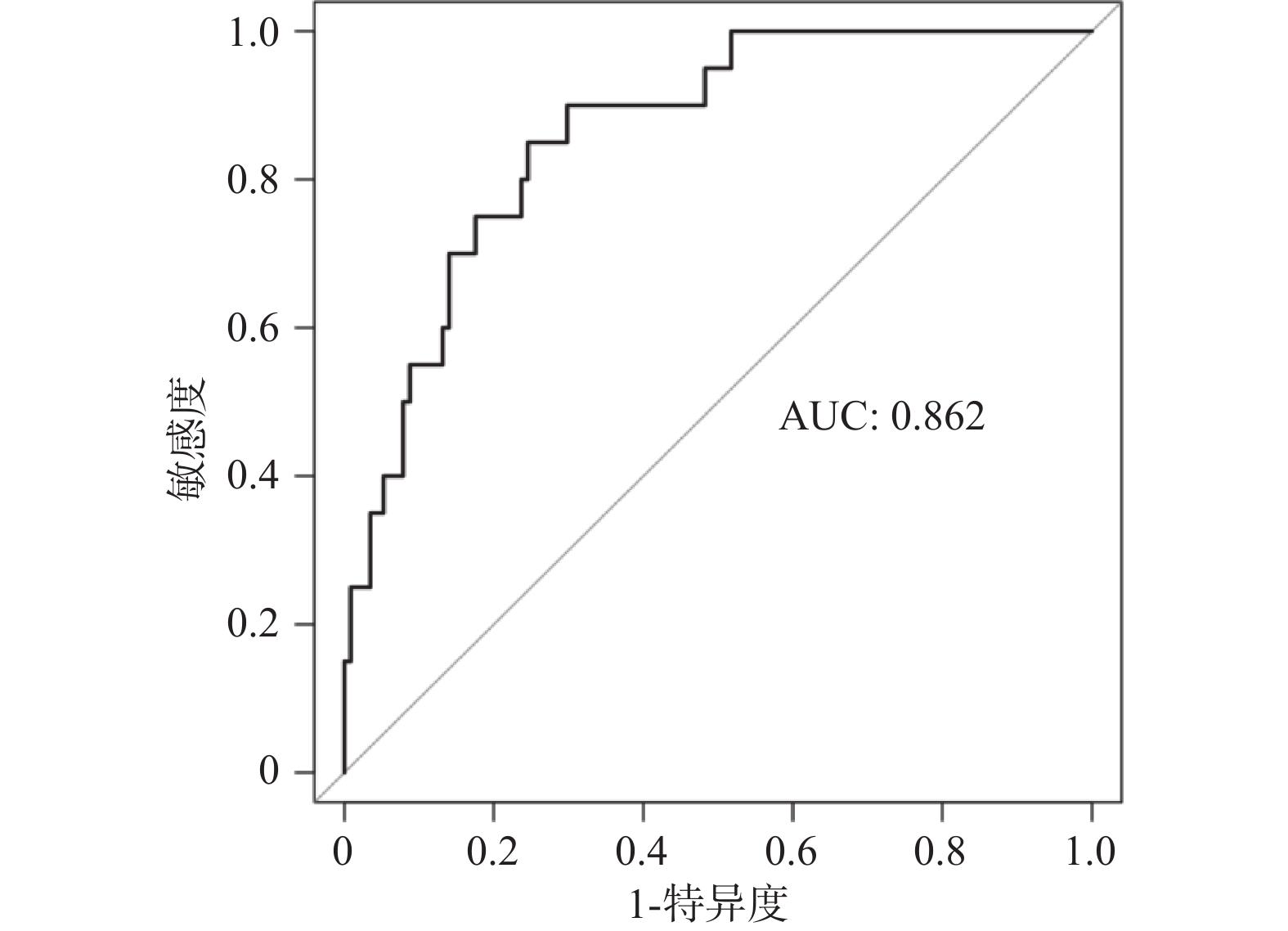
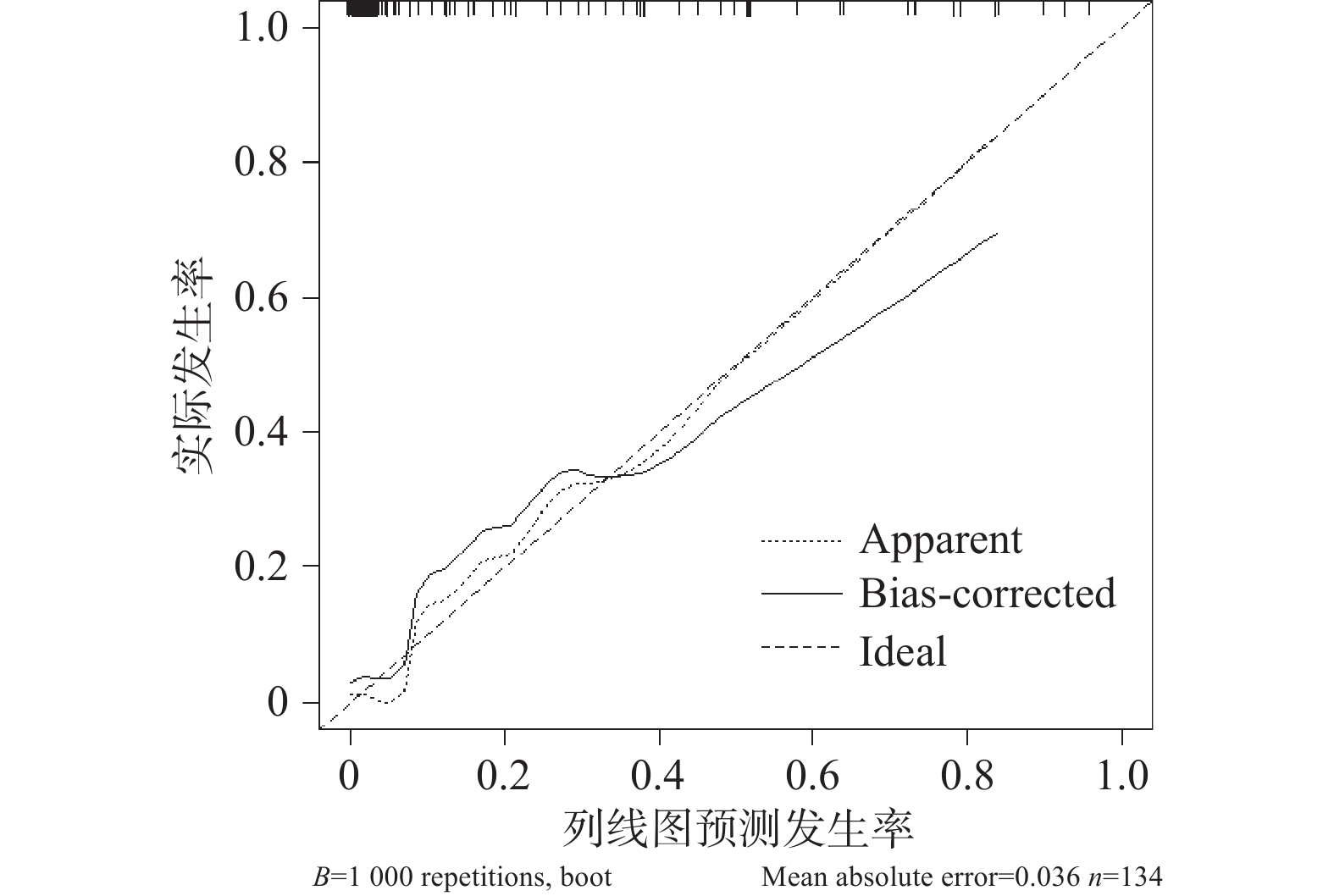
目的 探讨多模态超声影像联合临床指标预测缺血性脑卒中(ischemic stroke,IS)进展的临床价值。 方法 选取2020年1月至2022年10月云南省第三人民医院收治的134例IS患者作为研究对象,根据美国国立卫生研究院卒中量表(National Institute of Heath stroke scale,NIHSS)评分划分为进展性缺血性脑卒中(progressive ischemic stroke,PIS)组(n=20)、非进展缺血性脑卒中(NPIS)组(n=114),统计2组临床指标、多模态超声影像表现及相关参数,采用Logistic筛选PIS影响因素,并绘制列线图模型,采用受试者工作特征(receiver operating characteristic,ROC)曲线、校准曲线验证该列线图模型预测效能。 结果 2组年龄、基线老年营养风险指数(geriatric nutritional risk index,GNRI)评分、基线同型半胱氨酸(homocysteine,Hcy)、基线尿酸(uric acid,UA)比较,差异有统计学意义(P<0.05);2组峰值时间(time to peak,TTP)、峰值强度(peak intensity,PI)、曲线下面积(AUCTC)、颈动脉斑块增强模式、最大弹性模量的平均值(MEmax)、最小弹性模量的平均值(MEmin)比较,差异有统计学意义(P<0.05);Logistic分析显示,基线GNRI评分、基线UA、TTP、PI、AUCTC、颈动脉斑块增强模式、MEmax、MEmin是PIS影响因素(P<0.05);基于以上因素绘制列线图模型,ROC曲线、校准曲线显示,该模型具有较好预测效能,且预测效能与实际吻合较好。 结论 PIS影响因素包括基线GNRI评分、基线UA、TTP、PI、AUCTC、颈动脉斑块增强模式、MEmax、MEmin,基于上述因素绘制的列线图模型具有较好区分度和准确度。 Abstract:Objective To investigate the clinical value of multimodal ultrasonography combined with clinical indicators in predicting the progression of ischemic stroke (IS). Methods A total of 134 patients with IS admitted to Third People's Hospital of Yunnan Province from January 2020 to October 2022 were selected as study objects and were divided into progressive ischemic stroke (PIS) group (n=20) and non-progressive ischemic stroke (NPIS) group (n=114) according to the National Institutes of Health Stroke Scale (NIHSS) score. The clinical indicators, multi-modal ultrasonic image manifestations and related parameters of the two groups were counted, the influencing factors of PIS were screened by Logistics, the nomogram model was drawn, and the predictive efficiency of the nomogram model was evaluated by ROC curve and calibration curve. Results There were significant differences in age, baseline nutritional risk index (GNRI) score, baseline homocysteine (Hcy) and baseline uric acid (UA) between the two groups (P < 0.05). The peak time (TTP), peak intensity (PI), the area under the curve (AUC), carotid plaque enhancement mode, the mean value of maximum elastic modulus (MEmax) and mean value of minimum elastic modulus (MEmin) were compared between the two groups, and the differences were statistically significant ( P < 0.05). Logistic analysis showed that baseline GNRI score, baseline UA, TTP, PI, AUCTC, carotid plaque enhancement pattern, MEmax and MEmin were the influencing factors of PIS ( P< 0.05). Based on the above factors, the nomogram model was drawn. ROC curve and calibration curve showed that the model had good prediction efficiency, and the prediction efficiency was in good agreement with the reality. Conclusion The influencing factors of PIS include baseline GNRI score, baseline UA, TTP, PI, AUCTC, carotid plaque enhancement pattern, MEmax, MEmin, and the neagram model based on the above factors has good differentiation and accuracy. -
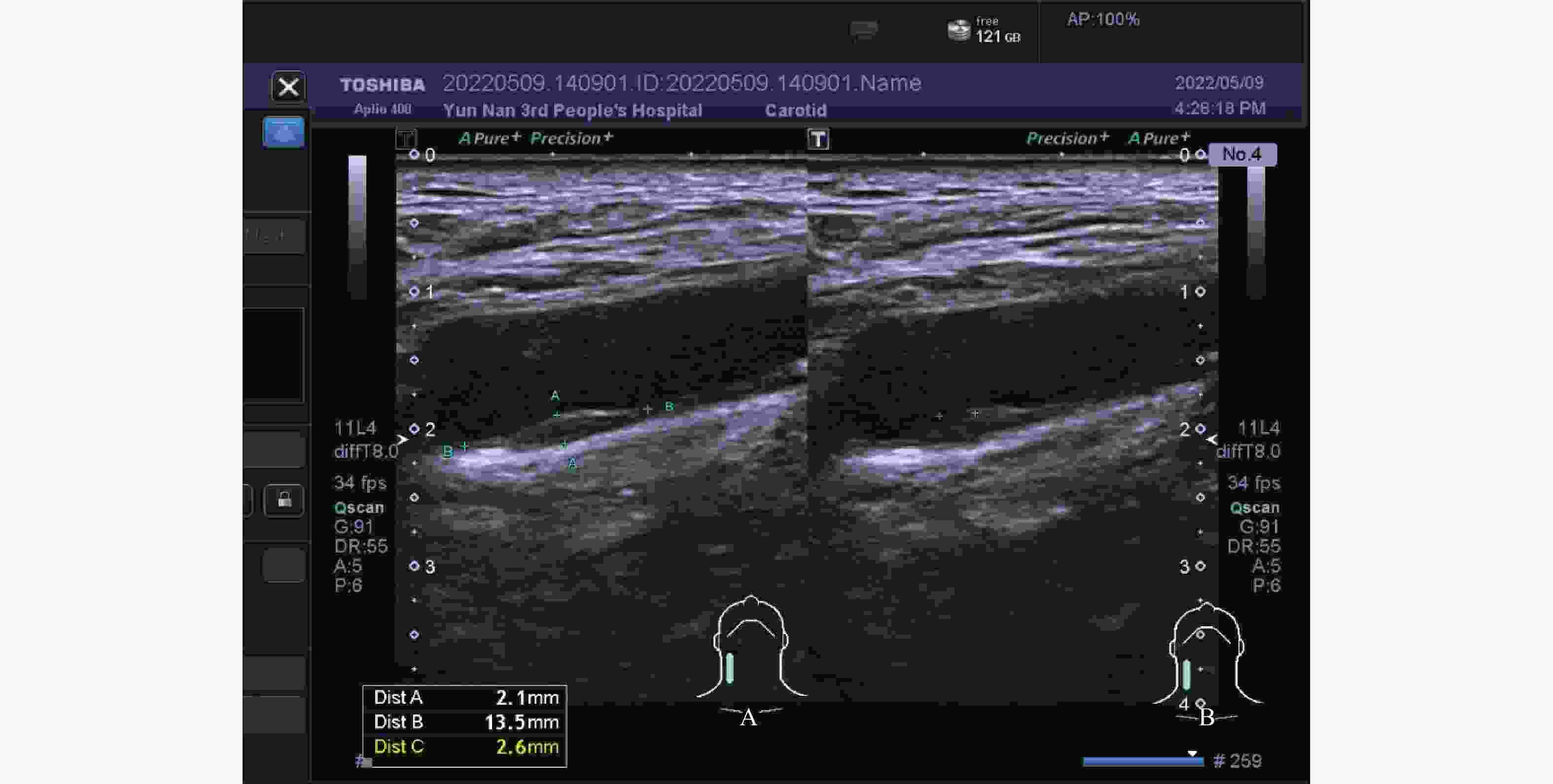
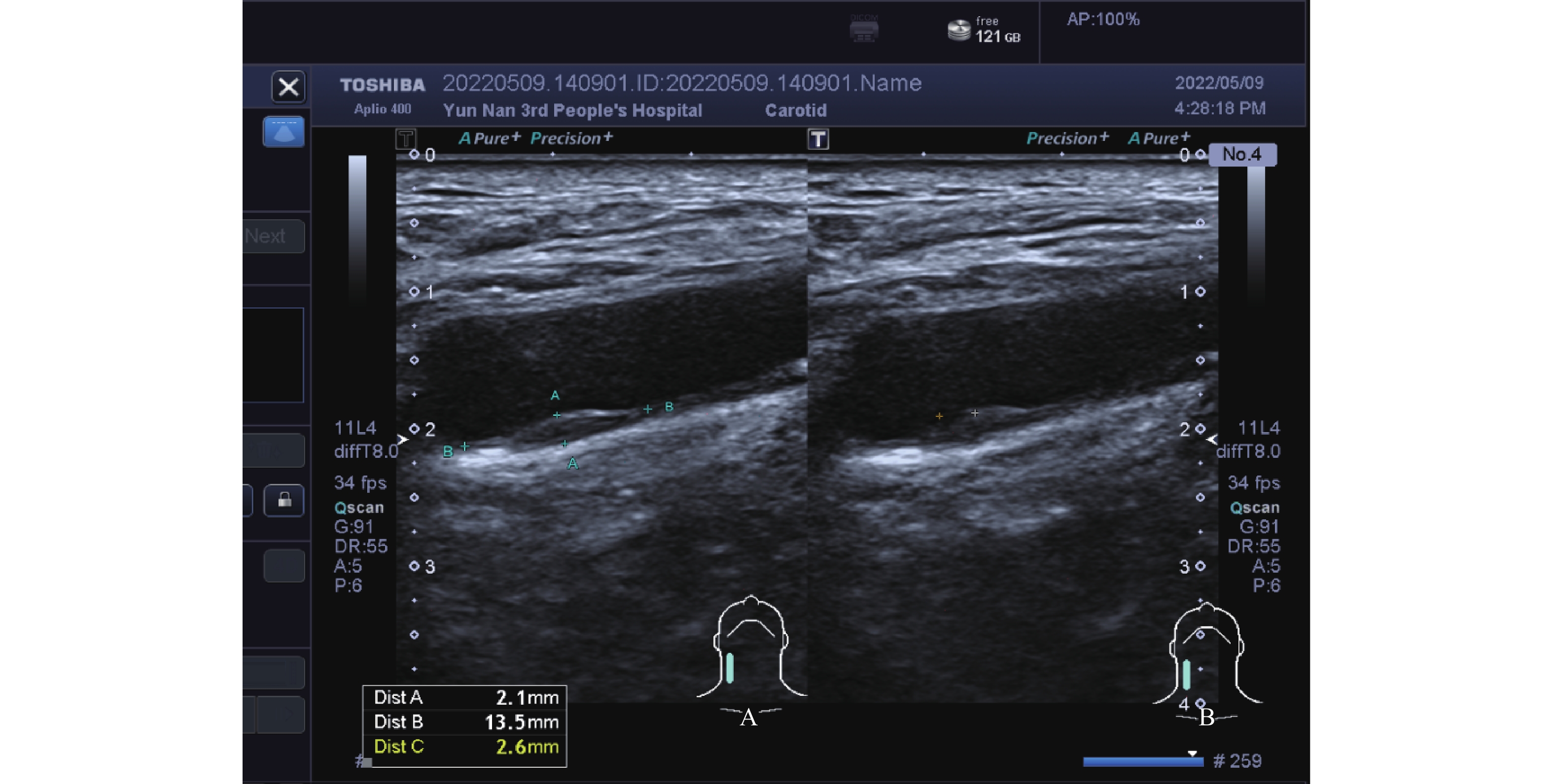
图 1 常规超声影像学表现
A:右侧颈总动脉后壁低回声斑块,内回声不均;B:右侧颈总动脉后壁斑块内无回声脂质区。
Figure 1. Routine ultrasound imaging findings
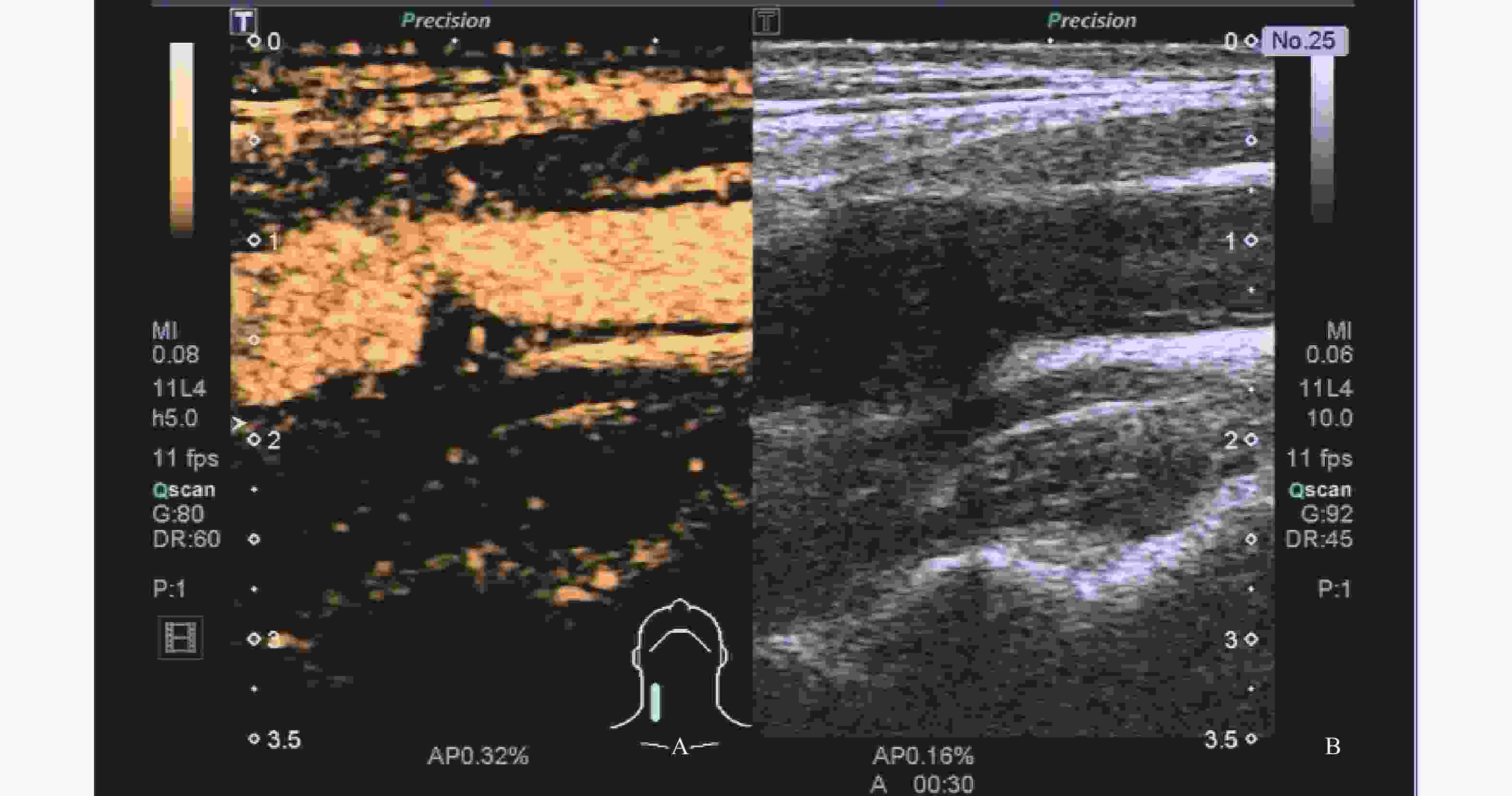
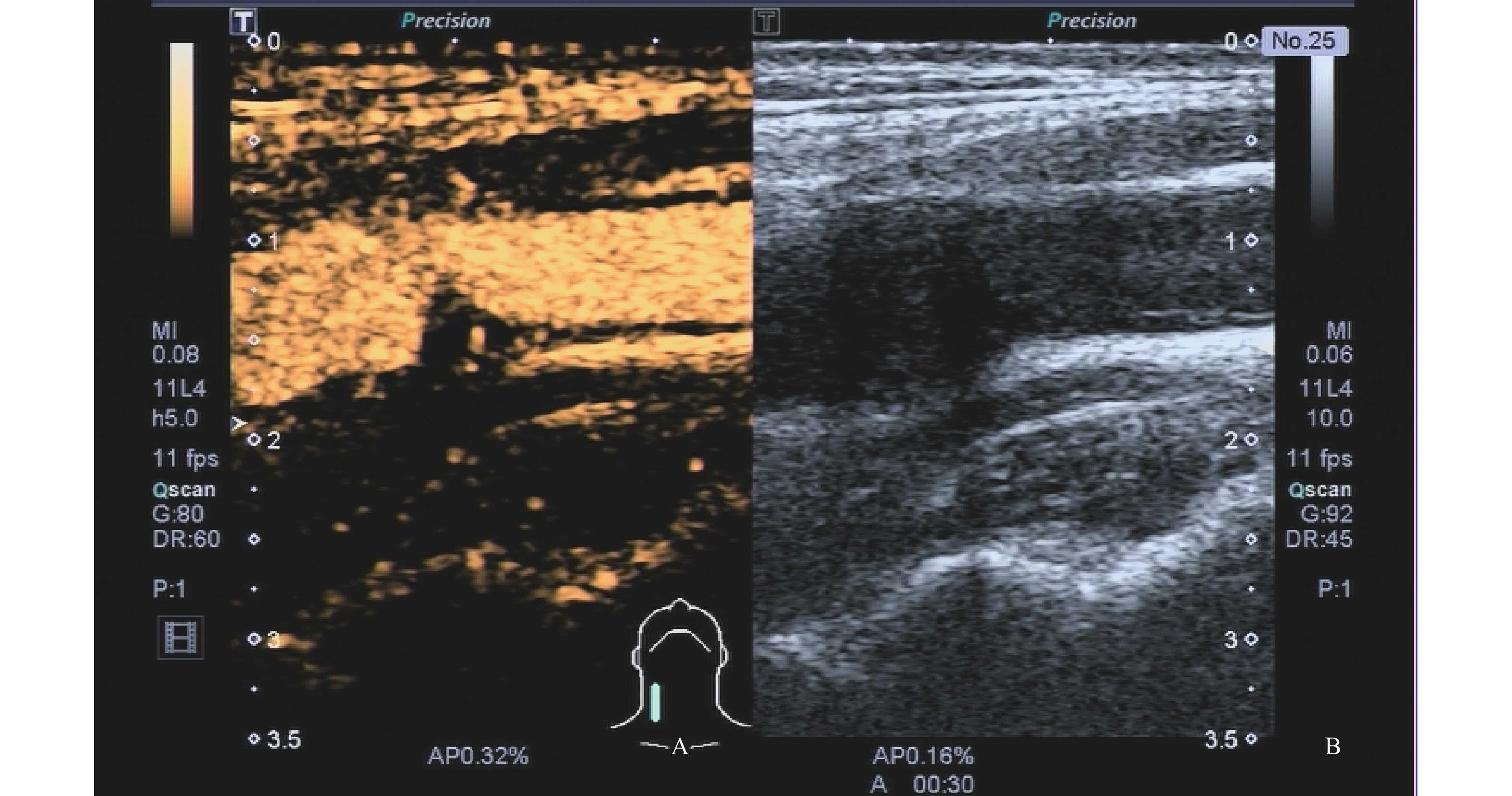
图 2 超声造影检查
A:超声造影示斑块内新生血管;B:颈动脉斑块二维声像图。
Figure 2. Contrast enhanced ultrasound examination
表 1 2组临床指标[( $ \bar x \pm s $)/n(%)] (1)
Table 1. Clinical indicators of patients in the two groups [ $ \bar x \pm s$)/n(%)] (1)
组别 性别(男/女) 年龄(岁) BMI(kg/m2) 发病至入院时间(h) 基线NIHSS评分(分) 基线GNRI评分(分) PIS组(n=20)
14/6 68.68±3.51 21.89±0.63 4.14±1.32 13.32±1.15 91.12±8.89 NPIS组(n=114) 63/51 62.21±4.45 21.76±0.88 4.34±1.01 12.78±1.67 103.21±10.33 t/χ2 1.512 6.167 0.632 0.778 1.387 4.920 P 0.219 <0.001* 0.529 0.438 0.168 <0.001* *P<0.05。  下载: 导出CSV
下载: 导出CSV
表 1 2组临床指标[( $\bar x \pm s $)/n(%)] (2)
Table 1. Clinical indicators of patients in the two groups [ $\bar x \pm s$)/n(%)] (2)
组别 基线Hcy(μmol/L) 基线UA(μmol/L) 基线WBC(×109/L) 基线CRP(mg/L) 吸烟史 饮酒史 脑卒中史 PIS组(n=20)
18.22±2.34 300.02±15.56 8.11±0.56 291.12±41.12 9(45.00) 11(55.00) 5(25.00) NPIS组(n=114) 13.38±1.51 212.21±13.35 7.89±0.73 289.99±42.86 49(42.98 58(50.88) 20(17.54) t/χ2 12.061 26.458 1.282 0.109 0.028 0.116 0.229 P <0.001* <0.001* 0.202 0.913 0.867 0.734 0.430 *P<0.05。
下载: 导出CSV
表 1 2组临床指标[( $ \bar x \pm s $)/n(%)] (3)
Table 1. Clinical indicators of patients in the two groups [ $ \bar x \pm s $)/n (%)] (3)
组别 TOAST分型 合并疾病 2SUE CE SAO SOE LAA 高脂血症 糖尿病 高血压 冠心病 PIS组(n=20)
3(15.00) 3(15.00) 3(15.00) 1(5.00) 10(50.00) 10(50.00) 8(40.00) 6(30.00) 5(25.00) NPIS组(n=114) 19(16.67) 17(14.91) 15(13.16) 4(3.51) 59(51.75) 41(35.96) 37(32.46) 29(25.44) 23(20.18) t/χ2 0.003 1.422 0.434 0.183 0.037 P 0.998 0.233 0.510 0.668 0.848 *P<0.05。
下载: 导出CSV
表 2 2组常规超声表现[n(%)]
Table 2. Routine ultrasound manifestations of patients in the two groups[n(%)]
组别 颈动脉斑块 颈动脉斑块性质 颈动脉斑块回声特征 有 无 扁平斑 硬斑 溃疡斑 软斑 低回声 等回声 强回声 PIS组(n=20)
12(60.00) 8(40.00) 3(15.00) 4(20.00) 2(10.00) 3(15.00) 5(25.00) 5(25.00) 2(10.00) NPIS组(n=114) 68(59.65) 46(40.35) 19(16.67) 24(21.05) 6(5.26) 19(16.67) 23(20.18) 30(26.32) 15(13.16) t/χ2/z 0.001 0.703 0.333 P 0.976 0.873 0.847 *P<0.05。
下载: 导出CSV
表 3 CUES定量参数[n(%)]
Table 3. CUES quantitative parameters [n(%)]
组别 始增时间
(s)TTP
(s)曲线上升
支斜率MTT
(s)AUCTC
(dB·s)PI
(dB)颈动脉斑块 颈动脉斑块增强模式 有 无 1级
2级 3级 PIS组
(n=20)5.49±
0.438.67±
1.230.88±
0.4027.11±
4.433005.51±
468.8172.88±
6.6715
(75.00)5
(25.00)1
(5.00)6
(30.00)8
(40.00)NPIS组
(n=114)5.41±
0.5511.12±
2.310.85±
0.4628.50±
3.722371.68±
400.2465.52±
7.2980
(70.18)34
(29.82)21
(18.42)45
(39.47)14
(12.28)t/χ2/z 0.618 4.620 0.000 1.497 6.364 4.214 0.192 9.717 P 0.538 <0.001* 1.000 0.137 <0.001* <0.001* 0.661 0.008 *P<0.05。
下载: 导出CSV
表 4 SWE定量参数 ( $\bar x \pm s $,kPa)
Table 4. SWE quantitative parameters ( $\bar x \pm s $,kPa)
组别 MEmean MEmax MEmin PIS组(n=20)
70.08±7.56 84.42±10.13 67.55±5.53 NPIS组(n=114) 68.96±8.04 73.95±8.87 60.33±6.12 t/χ2 0.579 4.766 4.932 P 0.563 <0.001* <0.001* *P<0.05。
下载: 导出CSV
表 5 PIS发病多因素分析
Table 5. Multivariate analysis of PIS incidence
自变量 赋值 β SE Wald χ2 OR 95%CI P 常量 16.612 年龄 实测值 0.155 0.412 0.142 1.168 0.871~1.566 0.044 基线GNRI评分 实测值 −0.581 0.135 18.531 0.559 0.432~0.724 0.001* 基线UA 实测值 0.226 0.369 0.374 1.253 0.669~2.347 0.341 基线Hcy 实测值 1.550 0.402 14.875 4.714 1.338~16.605 0.001* TTP 实测值 −0.820 0.171 22.990 0.440 0.376~0.516 0.001* PI 实测值 1.645 0.365 20.314 5.182 1.568~17.123 0.001* AUCTC 实测值 1.727 0.417 17.150 5.623 2.224~14.218 0.001* 颈动脉斑块增强模式 1级=1,2级=2,3级=3 1.632 0.358 20.779 5.114 1.376~19.004 0.001* MEmax 实测值 1.800 0.436 17.036 6.047 2.268~16.123 0.001* MEmin 实测值 1.725 0.517 11.130 5.611 2.004~15.712 0.001* *P<0.05。
下载: 导出CSV
-
[1] Feske S K. Ischemic stroke[J]. Am J Med,2021,134(12):1457-1464. doi: 10.1016/j.amjmed.2021.07.027 [2] DeLong J H,Ohashi S N,O'Connor K C,et al. Inflammatory responses after ischemic stroke[J]. Semin Immunopathol,2022,44(5):625-648. doi: 10.1007/s00281-022-00943-7 [3] Zhao T,Zhu T,Xie L,et al. Neural stem cells therapy for ischemic stroke: Progress and challenges[J]. Transl Stroke Res,2022,13(5):665-675. doi: 10.1007/s12975-022-00984-y [4] Yang D B,Zhou J,Feng L,et al. Value of superb micro-vascular imaging in predicting ischemic stroke in patients with carotid atherosclerotic plaques[J]. World J Clin Cases,2019,7(7):839-848. doi: 10.12998/wjcc.v7.i7.839 [5] Rabelo N N,Telles J P M,Pipek L Z,et al. Homocysteine is associated with higher risks of ischemic stroke: A systematic review and meta-analysis[J]. PLoS One,2022,17(10):e0276087. doi: 10.1371/journal.pone.0276087 [6] 王娅,周厚援,罗志强,等. 新预测模型AULTS评分对缺血性脑卒中的预测价值[J]. 中华全科医学,2021,19(10):1666-1668,1696. [7] 中华医学会神经病学分会,中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志,2018,51(9):666-682. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004 [8] 张秀玲. 实时超声弹性成像技术评估脑卒中患者颈动脉斑块稳定性的应用研究[J]. 广州医药,2020,51(1):14-18. doi: 10.3969/j.issn.1000-8535.2020.01.004 [9] 乐元洁,陈慧敏,贲志飞. 颈动脉斑块患者超声造影评级与脑卒中危险因素的相关性分析[J]. 现代实用医学,2017,29(4):438-439. doi: 10.3969/j.issn.1671-0800.2017.04.011 [10] Martinez-Sanchez P,Alexandrov A V. Ultrasonography of carotid plaque for the prevention of stroke[J]. Expert Rev Cardiovasc Therm,2013,11(10):1425-40. doi: 10.1586/14779072.2013.816475 [11] 陈欣,马赟英,尹少华,等. 进展性缺血性脑卒中患者血糖、C-反应蛋白变化特点及与预后的相关性[J]. 河北医药,2021,43(17):2589-2593. doi: 10.3969/j.issn.1002-7386.2021.17.006 [12] 吴方玲,胡金花,黄菊霞,等. 颈动脉斑块超微血流成像联合颈动脉彩色多普勒血流成像血流动力学参数对进展性缺血性脑卒中的预测价值[J]. 中国医药导报,2023,20(8):91-94. [13] Yan D,Shen Z,Zhang S,et al. Prognostic values of geriatric nutritional risk index (GNRI) and prognostic nutritional index (PNI) in elderly patients with diffuse large b-Cell lymphoma[J]. J Cancer,2021,12(23):7010-7017. doi: 10.7150/jca.62340 [14] 姜逍瑶,赵旭东,鲍磊,等. 老年营养风险指数对急性缺血性脑卒中患者预后的预测价值[J]. 中华老年心脑血管病杂志,2023,25(1):35-38. doi: 10.3969/j.issn.1009-0126.2023.01.010 [15] Esse R,Barroso M,Tavares de Almeida I,et al. The contribution of homocysteine metabolism disruption to endothelial dysfunction: State-of-the-art[J]. Int J Mol Sci,2019,20(4):867. doi: 10.3390/ijms20040867 [16] Gherghina M E,Peride I,Tiglis M,et al. Uric acid and oxidative stress-relationship with cardiovascular,metabolic,and renal impairment[J]. Int J Mol Sci,2022,23(6):3188. doi: 10.3390/ijms23063188 [17] 张力维,谌雪,王义成,等. 颈动脉斑块SMI分级联合血清同型半胱氨酸对进展性缺血性脑卒中的预测价值[J]. 中国超声医学杂志,2022,38(2):125-128. doi: 10.3969/j.issn.1002-0101.2022.02.002 [18] 周媛,杨小迪. 血尿酸和脑钠肽水平与进展性缺血性脑卒中的相关性研究[J]. 蚌埠医学院学报,2016,41(9):1152-1154. [19] Xu M,Jin S,Li F,et al. The diagnostic value of radial and carotid intima thickness measured by high-resolution ultrasound for ischemic stroke[J]. J Am Soc Echocardiogr,2021,34(1):72-82. doi: 10.1016/j.echo.2020.09.006 [20] Hoyer U C I,Lennartz S,Abdullayev N,et al. Imaging of the extracranial internal carotid artery in acute ischemic stroke: assessment of stenosis,plaques,and image quality using relaxation-enhanced angiography without contrast and triggering (REACT)[J]. Quant Imaging Med Surg,2022,12(7):3640-3654. doi: 10.21037/qims-21-1122 [21] 李朝军,金琳,王枫,等. 应用剪切波弹性成像评价急性缺血性脑卒中患者颈动脉弹性及其相关因素[J]. 中华超声影像学杂志,2015,24(7):571-575. doi: 10.3760/cma.j.issn.1004-4477.2015.07.005 [22] 顾秀娟,张巍,郑帅,等. 颈动脉斑块常规超声及超声造影预测颈动脉狭窄患者缺血性脑卒中[J]. 中国介入影像与治疗学,2022,19(9):570-574. [23] 孙飞一,潘晓芳,贾晓东,等. 多模态超声检查结合临床预测颈动脉粥样硬化患者缺血性脑卒中或短暂性脑缺血复发[J]. 中国医学影像技术,2022,38(1):53-58. [24] Dabravolski S A,Markin A M,Andreeva E R,et al. Molecular mechanisms underlying pathological and therapeutic roles of pericytes in atherosclerosis[J]. Int J Mol Sci,2022,23(19):11663. doi: 10.3390/ijms231911663 [25] Yao J,Yang Z,Huang L,et al. Low-intensity focused ultrasound-responsive ferrite-encapsulated nanoparticles for atherosclerotic plaque neovascularization theranostics[J]. Adv Sci (Weinh),2021,8(19):e2100850. doi: 10.1002/advs.202100850 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1846
- HTML全文浏览量: 969
- PDF下载量: 25
- 被引次数: 0
