

Application of Asphyxiation Technique in Thoracoscopic Segmentectomy
-
摘要:
目的 观察窒息氧合技术对肺段间平面显示速率、术中氧代谢指标、血清低氧诱导因子1α(HIF-1α)及术后并发症的影响。 方法 择期行胸腔镜肺段切除术患者75例,年龄22~65岁,ASA 分级为I~II级,随机分为3组,每组25例。C 组:单肺机械通气组;T1组:经双腔气管导管通气侧给氧3 L/min行窒息氧合组;T2组:经双腔气管导管通气侧给氧7 L/min行窒息氧合组。监测并记录麻醉诱导前(T0)、双肺通气15 min(T1)、单肺通气15 min(T2)、纯氧双肺复张后(T3)、段间平面显示即刻(T4)、气管拔管后15 min(T5)各时间点患者的SpO2、HR、MAP、CO、CI、SV、pH、Hb、PO2/FiO2、PaCO2、A-aO2、Lac、O2Hb、hHb、ScvO2、CvO2并计算DO2、VO2及O2ER;分别于术前、术后即刻、术后24 h抽静脉血检测HIF-1α水平;记录理想段间平面出现时间、单肺通气时间、手术时间、术后苏醒时间、拔管时间、术中输液量、尿量、失血量、术后住院天数、及术后并发症发生情况。 结果 (1)T1组、T2组段间平面显示时间较C组缩短,差异有统计学意义(P < 0.05);(2)3组患者术后即刻及术后24 h血清低氧诱导因子1α水平分别高于同组术前水平,差异有统计学意义(P < 0.05);(3)T4时刻,T1组、T2组VO2、O2ER、pH、PO2/FiO2、A-aO2、O2Hb均低于C组,差异有统计学意义(P < 0.05)。ScvO2、PCO2、hHb均高于C组,差异有统计学意义(P < 0.05)。 结论 窒息氧合技术可有效加快段间平面显示速率,保证术中充足的氧供量,对机体氧供需平衡及细胞内氧环境无明显影响,在细胞、组织及器官水平均具有较好的安全性,可推广应用于临床。 -
关键词:
- 胸腔镜肺段切除术 /
- 窒息氧合技术 /
- 肺段间平面 /
- 氧代谢指标 /
- 血清低氧诱导因子1α
Abstract:Objective To observe the effects of asphyxia oxygenation on intersegment plane display rate, intraoperative oxygen metabolism indexes, serum hypoxia inducible factor 1α (HIF-1α) and postoperative complications. Methods 75 patients aged 22 to 65 years with ASA grade I to II were randomly divided into 3 groups, with 25 cases in each group. Group C was given one-lung mechanical ventilation; In T1 group, oxygen was given at the ventilation side of double-lumen endotracheal tube for 3 L/min for asphyxia and oxygenation; In T2 group, oxygen was given for 7L/min through the ventilation side of double-lumen endotracheal tube for asphyxia oxygenation. SpO2, HR, MAP, CO, CI, SV, pH, Hb, PO2/FiO2, PaCO2, A-aO2, Lac, O2Hb, hHb, ScvO2, CvO2, were monitored and recorded before the anesthesia induction (T0), 15 min after bilateral ventilation (t1), 15 min after one-lung ventilation (T2), after double-lung recruitment with pure oxygen (T3), immediately after the interval plane display (T4) and 15 min after tracheal extubation and DO2, VO2 and O2ER were calculated. The level of HIF-1α was detected by venous blood samples before the surgery, immediately after the surgery and 24 hours after the surgery. The occurrence time of ideal intersegment plane, single lung ventilation time, operation time, postoperative recovery time, extubation time, intraoperative infusion volume, urine volume, blood loss, postoperative hospitalization days, and postoperative complications were recorded. Results (1) The interval plane display time of T1 and T2 groups was shorter than that of C group, and the difference was statistically significant (P < 0.05). (2) The serum hypoxia induction factor 1α level immediately after the surgery and 24 h after the surgery in 3 groups was higher than that before the surgery, the difference was statistically significant (P < 0.05). (3) At T4, VO2, O2ER, pH, PO2/FiO2, A-aO2 and O2Hb in groups T1 and T2 were lower than those in group C, with the statistical significance (P < 0.05). ScvO2, PCO2 and hHb were higher than those in group C, and the difference was statistically significant (P < 0.05). Conclusion Asphyxiation technique can effectively accelerate the intersegmental plane display rate and ensure the adequate oxygen supply during the operation. It has no obvious influence on the balance of oxygen supply and demand of the body and the intracellular oxygen environment. It has good safety at the level of cells, tissues and organs, and can be applied in the clinical practice. -

图 1 术中单肺机械通气组(C组)示意图
Figure 1. Schematic diagram of the single lung mechanical ventilation group (group C) during operation

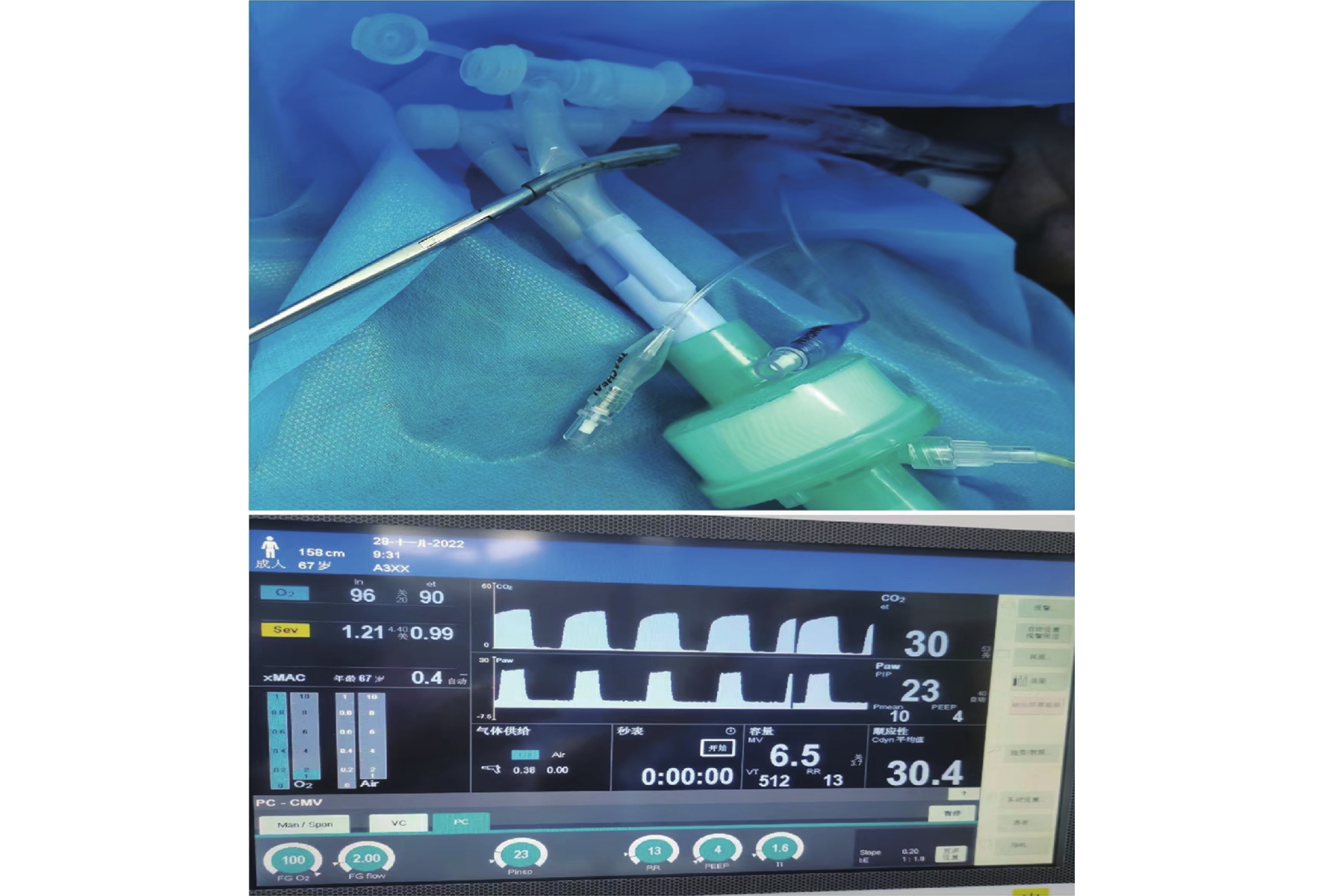
图 2 术中窒息氧合组(T1、T2组)示意图
Figure 2. Schematic diagram of intraoperative asphyxia oxygenation group (T1 and T2 groups)
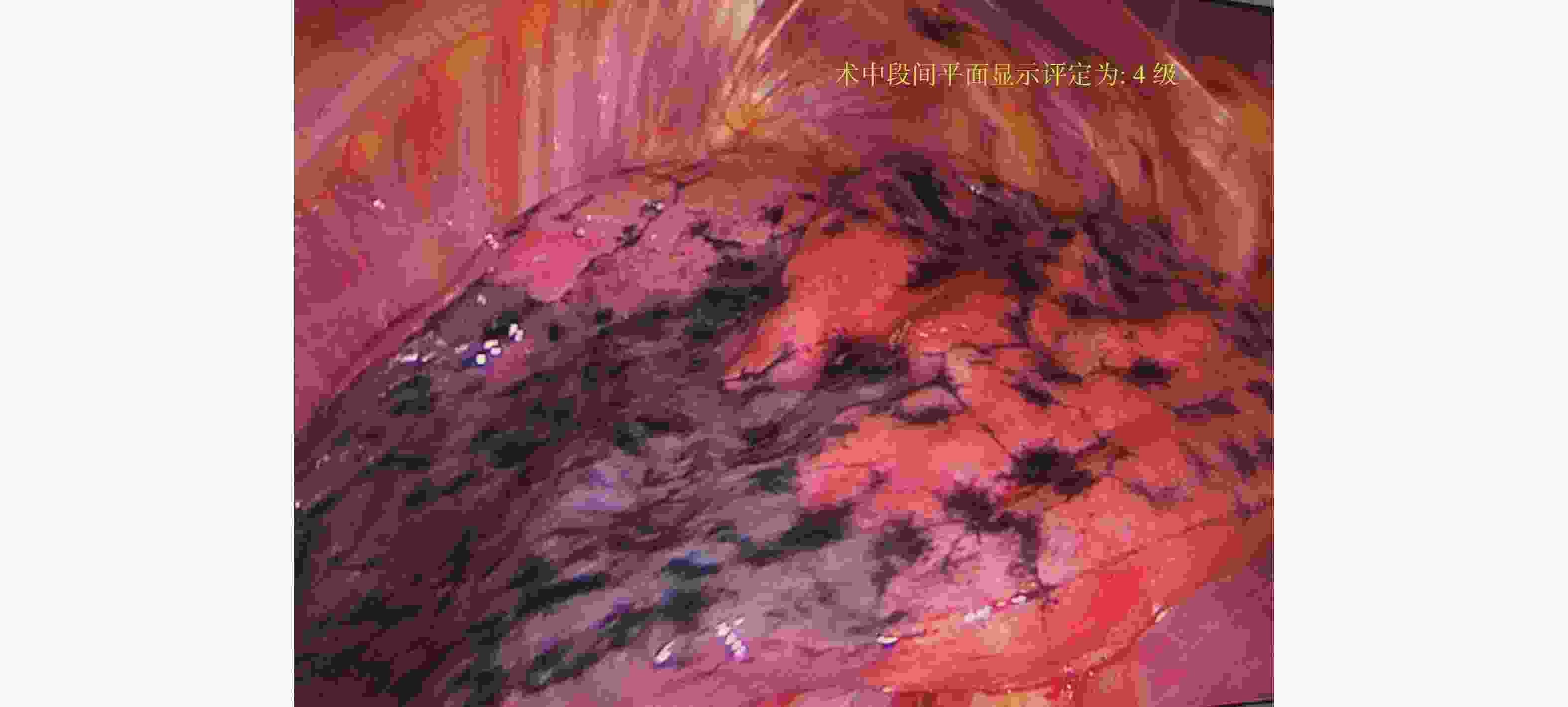
图 3 术中段间平面显示4级示例图
Figure 3. An example diagram showing the level 4 in the plane between the middle operations

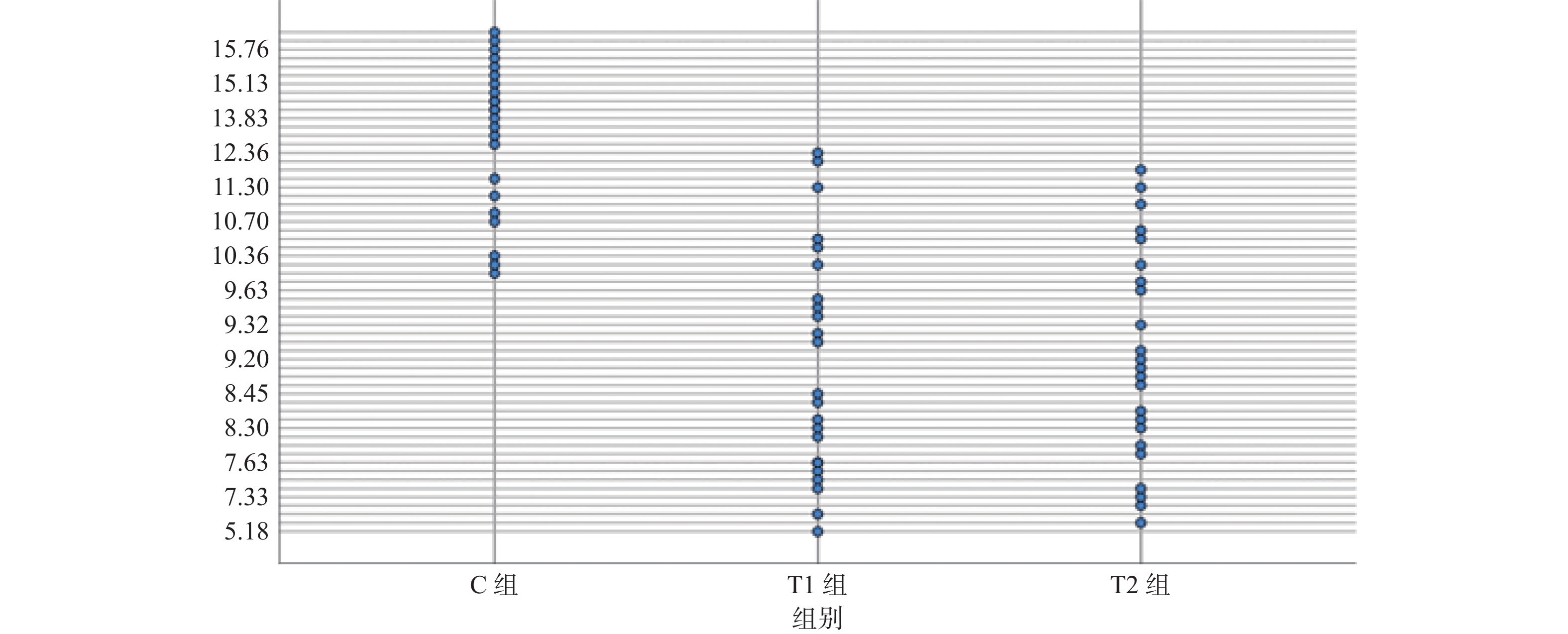
图 4 3组患者段间平面显示时间散点图(min)
Figure 4. Among three groups of patients section plane shows time scatter plot(min)

图 5 3组患者不同时间点氧代谢率变化趋势
Figure 5. Variation trend of oxygen metabolic rate of patients in three groups at different time points
表 1 3组患者临床资料的比较[(
$ \bar x \pm s $ )/ n(%),n = 75]Table 1. Comparison of clinical data among the three groups[(
$ \bar x \pm s $ )/ n(%),n = 75]临床资料 C组(n=25) T1组(n = 25) T2组(n = 25) F/χ2 P 性别(男/女) 8/17 7/18 10/15 0.529 0.755 年龄(岁) 52.6 ± 9.0 48.8 ± 11.15 50.1 ± 11.6 0.765 0.469 身高(cm) 161.2 ± 6.6 163.5 ± 5.9 162.8 ± 8.7 0.608 0.547 体重(kg) 57.0 ± 7.4 58.0 ± 5.8 57.7 ± 7.2 0.127 0.881 吸烟史 8(32.00) 7(28.00) 7(28.00) 0.935 0.119 结节大小(cm) 1.11 ± 0.38 0.99 ± 0.30 1.13 ± 0.36 1.073 0.348 结节位置 0.722 0.699 左肺上叶/左肺下叶 5/3 4/4 6/6 − − 右肺上叶/右肺下叶 11/6 9/8 8/5 − − FEV1(L/s) 2.52 ± 0.46 2.56 ± 0.49 2.55 ± 0.52 0.035 0.965 FEV1(%) 98.51 ± 12.7 93.05 ± 8.02 94.99 ± 12.81 1.355 0.265 FEVI/FVC(%) 86.23 ± 4.58 85.40 ± 7.19 83.50 ± 4.86 1.403 0.253 RV/TLC(%) 49.67 ± 7.39 47.47 ± 4.45 48.30 ± 5.63 1.044 0.358  下载: 导出CSV
下载: 导出CSV
表 2 术中一般资料的比较[(
$ \bar x \pm s $ ),n = 75]Table 2. Comparison of intraoperative general data [(
$ \bar x \pm s $ ),n = 75]组别 C组 T1组 T2组 F P 单肺通气时间(h) 1.60 ± 0.52 1.34 ± 0.48 1.60 ± 0.63 1.630 0.204 手术时间(h) 1.94 ± 0.66 1.67 ± 0.47 1.95 ± 0.62 1.659 0.198 失血量(mL) 53.47 ± 37.12 46.52 ± 19.68 48.26 ± 17.75 0.435 0.649 尿量(mL) 360.87 ± 124.28 300 ± 119.66 365.22 ± 185.52 1.429 0.247 输液量(mL) 735.43 ± 284.29 754.35 ± 318.35 728.26 ± 171.11 0.943 0.943
下载: 导出CSV
表 3 围术期不同时间点DO2(mL/min/m2)的比较[(
$ \bar x \pm s $ ),n = 75]Table 3. Comparison of DO2(mL/min/m2) at different time points in perioperative period [(
$ \bar x \pm s $ ),n = 75组别 n T0 T1 T2 T3 T4 T5 C组 25 547.02 ± 109.70 529.93 ± 93.62# 474.54 ± 61.80# 493.78 ± 79.57# 472.64 ± 73.11# 556.56 ± 82.76 T1组 25 562.59 ± 105.27 527.25 ± 86.05# 495.73 ± 61.14# 507.09 ± 89.40# 499.04 ± 72.61# 544.46 ± 82.10 T2组 25 574.49 ± 106.66 519.04 ± 82.81# 493.64 ± 63.23# 492.96 ± 60.64# 484.96 ± 52.09# 565.478 ± 61.82 F组间/时间/交互 1.197/21.979/0.957 P组间/时间/交互 0.309/< 0.001/0.465 与T0比较,#P < 0.05。
下载: 导出CSV
表 4 围术期不同时间点VO2(ml/min/m2)的比较[(
$ \bar x \pm s $ ),n = 75]Table 4. Comparison of VO2(mL/min/m2) at different time points in perioperative period [(
$ \bar x \pm s $ ),n = 75]组别 n T0 T1 T2 T3 T4 T5 C组 25 162.25 ± 35.90 141.03 ± 30.84# 128.52 ± 28.94# 128.96 ± 26.78# 131.83 ± 32.00# 127.88 ± 43.22 T1组 25 182.83 ± 54.88 155.44 ± 80.475# 128.28 ± 36.09# 149.04 ± 85.10# 97.54 ± 24.84*# 133.29 ± 55.74 T2组 25 174.44 ± 54.02 165.82 ± 73.99# 136.70 ± 75.48# 135.08 ± 40.67# 103.80 ± 46.29*# 132.63 ± 28.12 F组间/时间/交互 0.304/17.116/2.101 P组间/时间/交互 0.739/< 0.001/0.039 与C组比较,*P < 0.05;与T0比较,#P < 0.05。
下载: 导出CSV
表 5 围术期不同时间点O2ER(%)的比较[(
$ \bar x \pm s $ ),n = 75]Table 5. Comparison of O2ER (%) at different time points in perioperative period [(
$ \bar x \pm s $ ),n = 75]组别 n T0 T1 T2 T3 T4 T5 C组 25 29.74 ± 3.97 26.67 ± 3.97# 27.11 ± 4.92# 26.29 ± 4.80# 27.75 ± 4.28# 29.35 ± 19.59 T1组 25 30.03 ± 3.12 28.97 ± 15.11# 25.65 ± 5.89# 28.95 ± 14.13# 19.55 ± 4.55*# 28.70 ± 10.75 T2组 25 29.95 ± 4.02 28.53 ± 10.15# 26.91 ± 10.52# 27.89 ± 10.72# 22.85 ± 6.76*# 25.64 ± 4.26 F组间/时间/交互 0.254/6.071/1.763 P组间/时间/交互 0.777/< 0.001/0.019 与C组比较,*P < 0.05;与T0比较,#P < 0.05。
下载: 导出CSV
表 6 围术期不同时间点Lac(mmol/L)的比较[(
$ \bar x \pm s $ ),n = 75]Table 6. Comparison of Lac(mmol/L) at different time points in perioperative period [(
$ \bar x \pm s $ ),n = 75]组别 n T0 T1 T2 T3 T4 T5 C组 25 1.58 ± 0.54 1.48 ± 0.25 1.56 ± 0.38 1.53 ± 0.30 1.53 ± 0.39 1.51 ± 0.22 T1组 25 1.52 ± 0.49 1.53 ± 0.35 1.46 ± 0.32 1.55 ± 0.31 1.53 ± 0.33 1.49 ± 0.36 T2组 25 1.48 ± 0.35 1.45 ± 0.26 1.54 ± 0.26 1.58 ± 0.20 1.59 ± 0.21 1.54 ± 0.26 F组间/时间/交互 0.354/0.814/0.816 P组间/时间/交互 0.703/0.269/0.561
下载: 导出CSV
表 7 3组患者术前、术后即刻及术后24h血清HIF-1α水平比较[(
$ \bar x \pm s $ ),n = 75]Table 7. Comparison of serum hypoxia inducible factor 1α levels before,immediately after and 24h after surgery among the three groups [(
$ \bar x \pm s $ ),n = 75]组别 n 术前 术后即刻 术后24h C组 25 11.80 ± 1.63 18.59 ± 2.27* 17.32 ± 2.03* T1组 25 12.09 ± 1.78 17.63 ± 2.12* 16.58 ± 1.87* T2组 25 12.36 ± 1.81 18.02 ± 2.84* 18.04 ± 2.24* F组间/时间/交互 0.594/5.994/0.693 P组间/时间/交互 0.555/0.005/0.579 与术前比较,*P < 0.05。
下载: 导出CSV
表 8 术后一般资料分析[(
$ \bar x \pm s $ )/n(%),n = 75]Table 8. Analysis of postoperative general data[(
$ \bar x \pm s $ )/n(%),n = 75]组别 C组 T1组 T2组 F /χ2 P 苏醒时间(min) 10.83 ± 5.19 11.52 ± 7.20 10.71 ± 4.02 0.136 0.873 拔管时间(min) 17.45 ± 5.82 17.93 ± 8.22 16.62 ± 5.14 0.239 0.788 术后住院天数(d) 4.04 ± 2.23 3.83 ± 1.64 3.57 ± 0.95 5.029 0.199 术后病检结果
良性肿瘤
肺原发恶性肿瘤
肺转移瘤
8(32.00)
16(64.00)
1(4.00)
10(40.00)
14(56.00)
1(4.00)
7(28.00)
16(64.00)
2(8.00)0.865 0.078 术后3月心脑血管并发症 0(0.00) 0(0.00) 0(0.00) - 1.000
下载: 导出CSV
-
[1] 陈亮,王俊,吴卫兵,等. 胸腔镜精准肺段切除术技术流程和质量控制[J]. 中国胸心血管外科临床杂志,2019,26(1):21-28. [2] Fu H H,Feng Z,Li M,et al. The arterial-ligation-alone method for identifying the intersegmental plane during thoracoscopic anatomic segmentectomy[J]. Thorac Dis,2020,12(5):2343-2351. doi: 10.21037/jtd.2020.03.83 [3] Andolfi M,Potenza R,Seguin-Givelet A,et al. Identification of the intersegmental plane during thoracoscopic segmentectomy: State of the art[J]. Interact Cardiovasc Thorac Surg,2020,30(3):329-336. doi: 10.1093/icvts/ivz278 [4] Ettinger D S,Wood D E,Aisner D L,et al. Non-small cell lung cancer,version 3.2022,NCCN clinical practice guidelines in oncology[J]. Natl Compr Canc Netw,2022,20(5):497-530. doi: 10.6004/jnccn.2022.0025 [5] Zhang X,Li C,Jin R,et al. Intraoperative identification of the intersegmental plane: From the beginning to the future[J]. Front Surg,2022,8(9):948878. [6] 朱开彬,宁金峰,刘孟锋,等. 靶肺段萎陷法在单孔胸腔镜联合肺段切除术中的应用[J]. 现代肿瘤医学,2023,31(2):264-267. [7] 孙伟杰,张敏,陈旭,等. 肺循环单向阻断段间平面识别法在肺段切除术中的应用[J]. 中国胸心血管外科临床杂志,2023,30(1):52-57. [8] Yang W,Liu Z,Yang C,et al. Combination of nitrous oxide and the modified inflation-deflation method for identifying the intersegmental plane in segmentectomy: A randomized controlled trial[J]. Thorac Cancer,2021,12(9):1398-1406. doi: 10.1111/1759-7714.13919 [9] 胡俊熙,陆世春,孙超,等. 三维计算机断层扫描支气管血管成像联合荧光腔镜反染法在解剖性肺段切除术中的应用价值[J]. 中国微创外科杂志,2022,22(10):820-824. doi: 10.3969/j.issn.1009-6604.2022.10.010 [10] Krause K,Schumacher L Y,Sachdeva U M. Advances in imaging to aid segmentectomy for lung cancer[J]. Surg Oncol Clin N Am,2022,31(4):595-608. doi: 10.1016/j.soc.2022.06.003 [11] 刘俊,龚军,熊薇,等. 三维重建联合腔镜超声在解剖性肺段切除术中的临床应用[J]. 中国医学创新,2022,19(32):20-23. doi: 10.3969/j.issn.1674-4985.2022.32.005 [12] 徐正新. 膨胀萎陷法行肺段切除术时影响段间界面出现的因素研究[D]. 济南: 山东大学硕士学位论文, 2021. [13] Perl A,Whitwam JG,Chakrabarti M K,et al. Continuous flow ventilation without respiratory movement in cat,dog and human[J]. Br J Anaesth,1986,58(5):544-550. doi: 10.1093/bja/58.5.544 [14] Jung D M,Ahn H J,Jung S H,et al. Apneic oxygen insufflation decreases the incidence of hypoxemia during one-lung ventilation in open and thoracoscopic pulmonary lobectomy: A randomized controlled trial[J]. Thorac Cardiovasc Surg,2017,154(1):360-366. doi: 10.1016/j.jtcvs.2017.02.054 [15] Crewdson K,Heywoth A,Rehn M,et al. Apnoeic oxygenation for emergency anaesthesia of pre-hospital trauma patients[J]. Scand J Trauma Resusc Emerg Med,2021,29(1):10. doi: 10.1186/s13049-020-00817-7 [16] Soneru C N,Hurt H F,Petersen T R,et al. Apneic nasal oxygenation and safe apnea time during pediatric intubations by learners[J]. Paediatr Anaesth,2019,29(6):628-634. doi: 10.1111/pan.13645 [17] Grude O,Solli H J,Andersen C,et al. Effect of nasal or nasopharyngeal apneic oxygenation on desaturation during induction of anesthesia and endotracheal intubation in the operating room: A narrative review of randomized controlled trials[J]. Clin Anesth,2018,51(2):1-7. [18] Hamp T,Prager G,Baron-Stefaniak J,et al. Duration of safe apnea in patients with morbid obesity during passive oxygenation using high-flow nasal insufflation versus regular flow nasal insufflation,a randomized trial[J]. Surg Obes Relat Dis,2021,17(2):347-355. doi: 10.1016/j.soard.2020.09.027 [19] Liang C,Lv Y,Shi Y,et al. The fraction of nitrous oxide in oxygen for facilitating lung collapse during one-lung ventilation with double lumen tube[J]. BMC Anesthesiol,2020,20(1):180. doi: 10.1186/s12871-020-01102-x [20] Graf P T,Boesing C,Brumm I,et al. Ultraprotective versus apneic ventilation in acute respiratory distress syndrome patients with extracorporeal membrane oxygenation:A physiological study[J]. Intensive Care,2022,10(1):12. doi: 10.1186/s40560-022-00604-9 [21] Hochberg C H,Semler M W,Brower R G. Oxygen toxicity in critically ill adults[J]. Am J Respir Crit Care Med,2021,204(6):632-641. doi: 10.1164/rccm.202102-0417CI [22] Yin K,Xu Q,Wang J,et al. The predictive value of lung ultrasound combined with central venous oxygen saturation variations in the outcome of ventilator weaning in patients after thoracic surgery[J]. Am J Transl Res,2022,14(12):8621-8631. -




















 点击查看大图
点击查看大图
计量
- 文章访问数: 2439
- HTML全文浏览量: 1835
- PDF下载量: 6
- 被引次数: 0
