

The Relationship between PBEF,KLF2,IL-26 and The Condition and Prognosis of Severe Pneumonia in Children
-
摘要:
目的 讨论血清前B细胞克隆增强因子(pre-B cell colony-enhancing factor,PBEF)、Kruppel样转录因子2(kruppel like factor 2,KLF2)、白介素-26(Interleukin-26,IL-26)与重症肺炎(severe pneumonia,SP)患儿病情严重程度及预后转归的关系。 方法 选择西安市儿童医院2023年3月-2025年3月收治的180例SP患儿作为研究对象,使用ELISA试剂盒分别检测血清中PBEF、KLF2、IL-26的蛋白水平;根据急性生理与慢性健康评分Ⅱ(acute physiology and chronic health score,APACHE Ⅱ评分)判定患儿的病情严重程度并分组为非危重症组(n = 60)、危重症组(n = 75)和极危重症组(n = 45);根据SP患儿预后分为预后良好组(n = 127)和预后不良组(n = 53);血清PBEF、KLF2、IL-26水平与APACHE Ⅱ评分的相关性采用Pearson法分析;多因素Logistics回归分析影响SP患儿预后转归的因素;ROC曲线分析血清PBEF、KLF2、IL-26水平对SP患儿预后转归的预测价值。 结果 与非危重症组比较,危重症组、极危重症组APACHE Ⅱ评分及血清PBEF、IL-26水平升高(P < 0.05),血清KLF2水平均低(P < 0.05);与危重症组比较,极危重症组APACHE Ⅱ评分及血清PBEF、IL-26水平升高,血清KLF2水平降低(P < 0.05);SP患儿血清PBEF、IL-26水平与APACHE Ⅱ评分呈正相关,血清KLF2水平与APACHE Ⅱ评分呈负相关(P < 0.05);预后不良组较预后良好组极危重症患者比例、APACHE Ⅱ评分及血清PBEF、IL-26水平升高,血清KLF2水平降低(P < 0.05);血清PBEF、IL-26水平升高,KLF2水平降低是SP患儿发生预后不良的危险因素(P < 0.05);血清PBEF、KLF2、IL-26水平单独及联合预测患儿预后不良的AUC分别为0.769、0.820、0.814、0.933,三者联合预测价值更高(Z = 4.112、3.893、4.035,P < 0.001)。 结论 伴随SP患儿病情严重程度的增加,血清PBEF、IL-26水平升高,KLF2水平降低,三者可作为预测患儿预后转归的指标。 -
关键词:
- 重症肺炎 /
- 前B细胞克隆增强因子 /
- Kruppel样转录因子2 /
- 白介素-26 /
- 病情严重程度 /
- 预后转归
Abstract:Objective To discuss the relationship between serum pre-B cell colony-enhancing factor (PBEF), Kruppel like factor 2 (KLF2), interleukin-26 (IL-26) and the severity and prognosis of severe pneumonia (SP) in children. Methods A total of 180 children with SP admitted to Xi’ an Children’ s Hospital from March 2023 to March 2025 were selected as the research subjects. The protein levels of PBEF, KLF2 and IL-26 in serum were detected respectively using ELISA kits. The severity of the children's conditions was determined based on the acute physiology and chronic health score Ⅱ (APACHE Ⅱ score), and they were grouped into the non-critical group (n = 60), the critical group (n = 75), and the extremely critical group (n = 45). According to the prognosis of children with SP, they were divided into the good prognosis group (n = 127) and the poor prognosis group (n = 53). The correlations between the levels of serum PBEF, KLF2 and IL-26 and the APACHE Ⅱ score were analyzed by the Pearson method. Multivariate logistic regression analysis was conducted to analyze the factors influencing the prognosis and outcome of children with SP. ROC curve was used to analyze the predictive value of serum PBEF, KLF2 and IL-26 levels for the prognosis and outcome of children with SP. Results Compared with the non-critical group, the APACHE Ⅱ score, serum PBEF and IL-26 levels in the critical group and the extremely critical group were all increased (P < 0.05), and the serum KLF2 level was all decreased (P < 0.05). Compared with the critical group, the APACHE Ⅱ score and the levels of serum PBEF and IL-26 in the extremely critical group were increased, while the level of serum KLF2 was decreased (P < 0.05). The levels of serum PBEF and IL-26 in children with SP were positively correlated with the APACHE Ⅱ score, while the level of serum KLF2 was negatively correlated with the APACHE Ⅱ score (P < 0.05). The proportion of extremely critical patients, APACHE Ⅱ score, serum PBEF and IL-26 levels in the poor prognosis group were increased compared with those in the good prognosis group, while the serum KLF2 level was decreased (P < 0.05). The elevated levels of serum PBEF and IL-26 and the decreased level of KLF2 are risk factors for poor prognosis in children with SP (P < 0.05). The AUCs of serum PBEF, KLF2, and IL-26 levels alone and in combination for predicting poor prognosis in children were 0.769, 0.820, 0.814, and 0.933, respectively. The combined predictive value of the three was higher (Z=4.112, 3.893, 4.035, all P < 0.001). Conclusion With the increase of the severity of the disease in children with SP, the levels of serum PBEF and IL-26 were increased, and the level of KLF2 was decreased. The three can be used as indicators for predicting the prognosis and outcome of children. -
表 1 不同病情SP患儿基本资料及血清PBEF、KLF2、IL-26水平比较[($\bar x \pm s $)/n(%)]
Table 1. Basic Information of SP children with different conditions and comparison of serum PBEF,KLF2,and IL-26 levels [($\bar x \pm s $) /n (%)]
项目 非危重症组(n=60) 危重症组(n=75) 极危重症组(n=45) F/χ2 P 性别 2.164 0.339 男性 31(51.67) 39(52.00) 29(64.44) 女性 29(48.33) 36(48.00) 16(35.56) 年龄(岁) 8.15 ± 2.20 8.32 ± 2.33 8.71 ± 2.57 0.749 0.474 身高(cm) 125.34 ± 15.47 128.46 ± 18.33 124.85 ± 14.77 0.895 0.410 体重(kg) 30.23 ± 8.31 31.98 ± 8.17 30.22 ± 7.54 1.035 0.357 APACHE Ⅱ评分(分) 16.20 ± 4.15 21.26 ± 4.13△ 24.56 ± 4.75△# 51.205 <0.001* PBEF(ng/mL) 4.47 ± 0.78 4.93 ± 1.02△ 5.40 ± 1.10△# 11.936 <0.001* KLF2(ng/mL) 8.55 ± 1.49 7.06 ± 1.25△ 5.18 ± 1.04△# 87.876 <0.001* IL-26(pg/mL) 272.52 ± 41.19 335.07 ± 52.06△ 364.26 ± 59.78△# 46.392 <0.001* *P < 0.05;与非危重症比较,△P < 0.05;与危重症组比较,#P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 相关性分析
Table 2. Correlation Analysis
指标 APACHE Ⅱ评分 r P PBEF 0.445 <0.001* KLF2 −0.433 <0.001* IL-26 0.506 <0.001* *P < 0.05。
下载: 导出CSV
表 3 不同预后SP患儿基本资料及血清PBEF、KLF2、IL-26水平比较[($\bar x \pm s $)/n(%)]
Table 3. Comparison of basic Information and serum levels of PBEF,KLF2,and IL-26 in children with SP with different prognostic conditions [($\bar x \pm s $) /n (%)]
项目 预后良好组(n=127) 预后不良组(n=53) t/χ2 P 性别 0.499 0.480 男性 72(56.69) 27(50.94) 女性 55(43.31) 26(49.06) 年龄(岁) 8.19 ± 2.16 8.77 ± 2.44 1.580 0.116 身高(cm) 116.25 ± 15.52 117.16 ± 15.23 0.361 0.719 体重(kg) 41.39 ± 10.45 39.92 ± 10.60 0.857 0.393 APACHE Ⅱ评分(分) 17.13 ± 4.05 28.23 ± 4.70 15.971 <0.001* 病情严重程度 74.118 <0.001* 非危重症 51(40.16) 9(16.98) 危重症 67(52.76) 8(15.09) 极危重症 9(7.08) 36(67.93) PBEF(ng/mL) 4.55 ± 0.83 5.72 ± 1.09 7.831 <0.001* KLF2(ng/mL) 7.54 ± 1.32 6.00 ± 1.18 7.353 <0.001* IL-26(pg/mL) 303.16 ± 50.37 365.51 ± 58.39 7.216 <0.001* *P < 0.05。
下载: 导出CSV
表 4 多因素Logistic回归分析
Table 4. Multivariate Logistic regression analysis
影响因素 B SE Waldχ2 OR 95%CI P PBEF 1.165 0.336 12.016 3.205 1.659-6.192 <0.001* KLF2 −0.892 0.242 13.574 0.410 0.255-0.659 <0.001* IL-26 0.632 0.212 8.897 1.882 1.242-2.852 0.003* *P < 0.05。
下载: 导出CSV
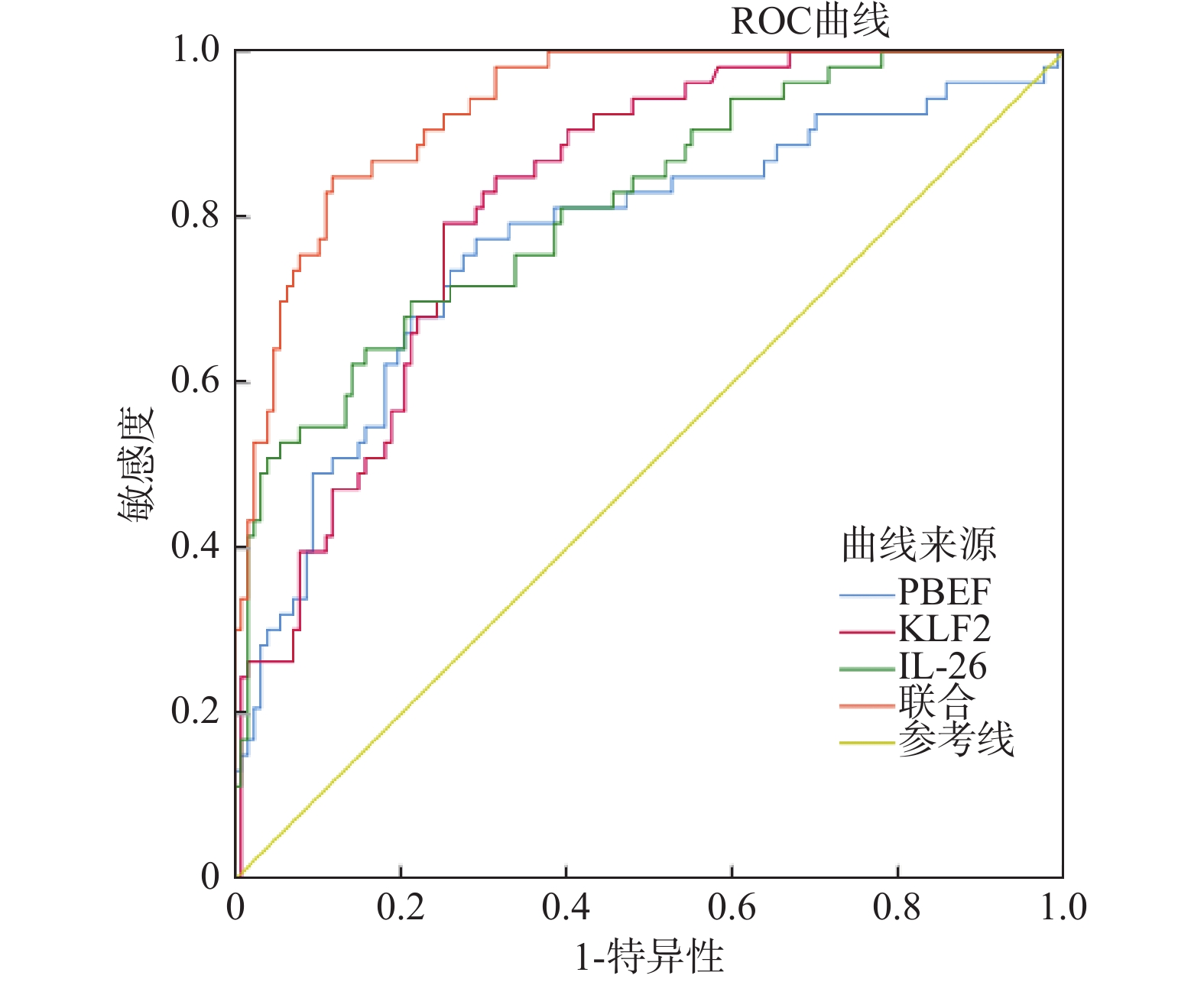
表 5 血清PBEF、KLF2、IL-26水平预测SP患儿预后转归的价值分析
Table 5. Value Analysis of Serum PBEF,KLF2 and IL-26 levels in predicting the prognosis and outcome of children with SP
指标 AUC 95%CI 敏感度(%) 特异性(%) 截断值 PBEF 0.769 0.700~0.828 77.36 70.87 5.02 ng/mL KLF2 0.820 0.756~0.874 79.25 74.80 6.75 ng/mL IL-26 0.814 0.749~0.868 69.81 78.74 332.34 pg/mL 联合 0.933 0.886~0.965 84.91 88.19 −
下载: 导出CSV
-
[1] Ching P R, Pedersen L L. Severe pneumonia[J]. Med Clin North Am, 2025, 109(3): 705-720. doi: 10.1016/j.mcna.2024.12.011 [2] Niederman M S, Torres A. Severe community-acquired pneumonia[J]. Eur Respir Rev, 2022, 31(166): 220123. doi: 10.1183/16000617.0123-2022 [3] 王丽阳, 王艺璁, 刘欢, 等. 血清RAGE、PBEF水平对重症肺炎患儿继发急性呼吸窘迫综合征的预测价值[J]. 疑难病杂志, 2024, 23(9): 1085-1089, 1099. [4] 袁丹, 曾丹, 李三, 等. KLF2在呼吸系统疾病治疗中的作用研究[J]. 临床肺科杂志, 2024, 29(8): 1270-1274. [5] 陈丁丁, 刘冬, 张文文, 等. AECOPD病情严重程度与血清IL-8、IL-26水平的相关性研究[J]. 临床医学研究与实践, 2025, 10(9): 37-41. [6] 中国医师协会急诊医师分会. 中国急诊重症肺炎临床实践专家共识[J]. 中国急救医学, 2016, 36(2): 97-107. doi: 10.3969/j.issn.1002-1949.2016.02.001 [7] 付玉茹, 孙振康, 刘成, 等. C反应蛋白/白蛋白比值与重症肺炎患者病情严重程度的关系及其对28 d死亡风险的预测价值[J]. 解放军医学杂志, 2025, 50(3): 309-317. [8] 中华人民共和国国家健康委员会, 国家中医药局. 儿童社区获得性肺炎诊疗规范(2019年版)[J]. 中华临床感染病杂志, 2019, 12(1): 6-13. [9] Yang S, Lu S, Guo Y, et al. A comparative study of general and severe mycoplasma pneumoniae pneumonia in children[J]. BMC Infect Dis, 2024, 24(1): 449. doi: 10.1186/s12879-024-09340-x [10] Lee K L, Lee C M, Yang T L, et al. Severe mycoplasma pneumoniae pneumonia requiring intensive care in children, 2010-2019[J]. J Formos Med Assoc, 2021, 120(1): 281-291. doi: 10.1016/j.jfma.2020.08.018 [11] 张宇坤, 郭文娟. 影响重症肺炎患儿预后的因素分析[J]. 中外医学研究, 2025, 23(18): 131-134. [12] Recinella L, Orlando G, Ferrante C, et al. Adipokines: New potential therapeutic target for obesity and metabolic, rheumatic, and cardiovascular diseases[J]. Front Physiol, 2020, 11: 578966. doi: 10.3389/fphys.2020.578966 [13] Lu C, Yang W, Zhou J, et al. Inhibition of pre-B cell colony enhancing factor reduces lung injury in rats receiving cardiopulmonary bypass[J]. Drug Des Devel Ther, 2021, 15: 51-60. doi: 10.2147/DDDT.S281554 [14] Garcia A N, Casanova N G, Valera D G, et al. Involvement of eNAMPT/TLR4 signaling in murine radiation pneumonitis: protection by eNAMPT neutralization[J]. Transl Res, 2022, 239: 44-57. doi: 10.1016/j.trsl.2021.06.002 [15] 朱丽娟, 薛乾隆, 林雪容, 等. MMP-9、PBEF及炎性因子预测重症急性胰腺炎肺损伤预后[J]. 分子诊断与治疗杂志, 2021, 13(7): 1142-1145. [16] Wittner J, Schuh W. Krüppel-like Factor 2 (KLF2) in immune cell migration[J]. Vaccines (Basel), 2021, 9(10): 1171. doi: 10.3390/vaccines9101171 [17] Wu D, Lee T H, Huang R T, et al. SARS-CoV-2 infection is associated with reduced Krüppel-like Factor 2 in human lung autopsy[J]. Am J Respir Cell Mol Biol, 2021, 65(2): 222-226. doi: 10.1165/rcmb.2020-0564LE [18] Han M, Pandey D. ZMPSTE24 regulates SARS-CoV-2 spike protein-enhanced expression of endothelial PAI-1[J]. Am J Respir Cell Mol Biol, 2021, 65(3): 300-308. doi: 10.1165/rcmb.2020-0544OC [19] Chrysanthopoulou A, Antoniadou C, Natsi A M, et al. Down-regulation of KLF2 in lung fibroblasts is linked with COVID-19 immunofibrosis and restored by combined inhibition of NETs, JAK-1/2 and IL-6 signaling[J]. Clin Immunol, 2023, 247: 109240. doi: 10.1016/j.clim.2023.109240 [20] Li X, Xu W, Jing T. Mechanism of KLF2 in young mice with pneumonia induced by streptococcus pneumoniae[J]. J Cardiothorac Surg, 2024, 19(1): 509. doi: 10.1186/s13019-024-02995-2 [21] Gilliet M, Modlin R L. Immunobiology of IL-26[J]. J Invest Dermatol, 2024, 144(6): 1217-1222. doi: 10.1016/j.jid.2023.10.038 [22] Cardenas E I, Ekstedt S, Piersiala K, et al. Increased IL-26 associates with markers of hyperinflammation and tissue damage in patients with acute COVID-19[J]. Front Immunol, 2022, 13: 1016991. doi: 10.3389/fimmu.2022.1016991 [23] Cardenas E I, Robertson J, Misaghian S, et al. Systemic increase in IL-26 is associated with severe COVID-19 and comorbid obstructive lung disease[J]. Front Immunol, 2024, 15: 1434186. doi: 10.3389/fimmu.2024.1434186 [24] Caterino M, Gelzo M, Sol S, et al. Dysregulation of lipid metabolism and pathological inflammation in patients with COVID-19[J]. Sci Rep, 2021, 11(1): 2941. doi: 10.1038/s41598-021-82426-7 [25] Che K F, Paulsson M, Piersiala K, et al. Complex involvement of Interleukin-26 in bacterial lung infection[J]. Front Immunol, 2021, 12: 761317. doi: 10.3389/fimmu.2021.761317 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 326
- HTML全文浏览量: 222
- PDF下载量: 36
- 被引次数: 0
