

Empirical Analysis of the Three-dimensional Structure of Clinical Reasoning Ability and Construction of Targeted Python Case Library from the Perspective of Cluster Analysis
-
摘要:
目的 明确临床医学实习生临床思维能力的内在结构与群体特征,构建针对性培养工具。 方法 采用多中心分层抽样,选取2023年7月至2024年4月期间在6所医院进行临床实习的321名临床医学实习生,通过自编《临床思维能力评估问卷》调查,结合相关分析、因子分析解析能力结构,K-means聚类识别群体特征,据此设计Python案例库并通过随机对照试验验证效果。 结果 临床思维能力为“诊断关联力、方案决策力、知识应用力”三维结构,累计方差解释率84.21%,多群体验证拟合良好(χ2/df = 2.31~2.45,RMSEA = 0.065~0.069);聚类分为高(33.33%)、中(42.68%)、低(23.99%)三类能力群体,各维度得分差异有统计学意义(P < 0.01)。案例库干预后,干预组各群体核心短板维度提升幅度显著高于对照组(高能力型诊断关联力F = 32.67,中能力型方案决策力F = 48.32,低能力型知识应用力F = 41.56,均P < 0.01)。 结论 临床思维能力三维结构与群体特征为精准培养提供靶向,Python案例库可推动临床思维培养向“数据驱动”转型。 Abstract:Objective To clarify the internal structure and population characteristics of clinical reasoning ability among clinical medical interns, construct targeted training tools, and provide evidence for clinical reasoning education reform. Methods A multi-center stratified sampling method was adopted to select 321 clinical medicine interns who underwent clinical internships in 6 hospitals from July 2023 to April 2024. A self-designed "Clinical Thinking Ability Assessment Questionnaire" was used for the survey. Correlation analysis and factor analysis were conducted to explore the ability structure, while K-means clustering was applied to identify group characteristics. Based on these findings, a Python case library was designed and its effectiveness was verified through a randomized controlled trial. Results Clinical thinking ability demonstrated a three-dimensional structure comprising "diagnostic association, decision-making for treatment planning, and knowledge application, " with a cumulative variance explanation rate of 84.21%. Multi-population validation showed good model fit (χ2/df = 2.31~2.45, RMSEA = 0.065~0.069). Clustering analysis identified three ability groups: high (33.33%), moderate (42.68%), and low (23.99%), with statistically significant differences across all dimensions (P < 0.01). After intervention with the case library, the improvement of core shortcoming dimensions in the intervention group was significantly higher than that in the control group (diagnostic relevance of high-ability group: F = 32.67; scheme decision-making ability of medium-ability group: F = 48.32; knowledge application ability of low-ability group: F = 41.56, all P < 0.01). Conclusion The three-dimensional structure and population characteristics of clinical thinking ability provide targeted guidance for precision training. The Python case library facilitates the transition of clinical thinking cultivation toward "data-driven" approaches. -
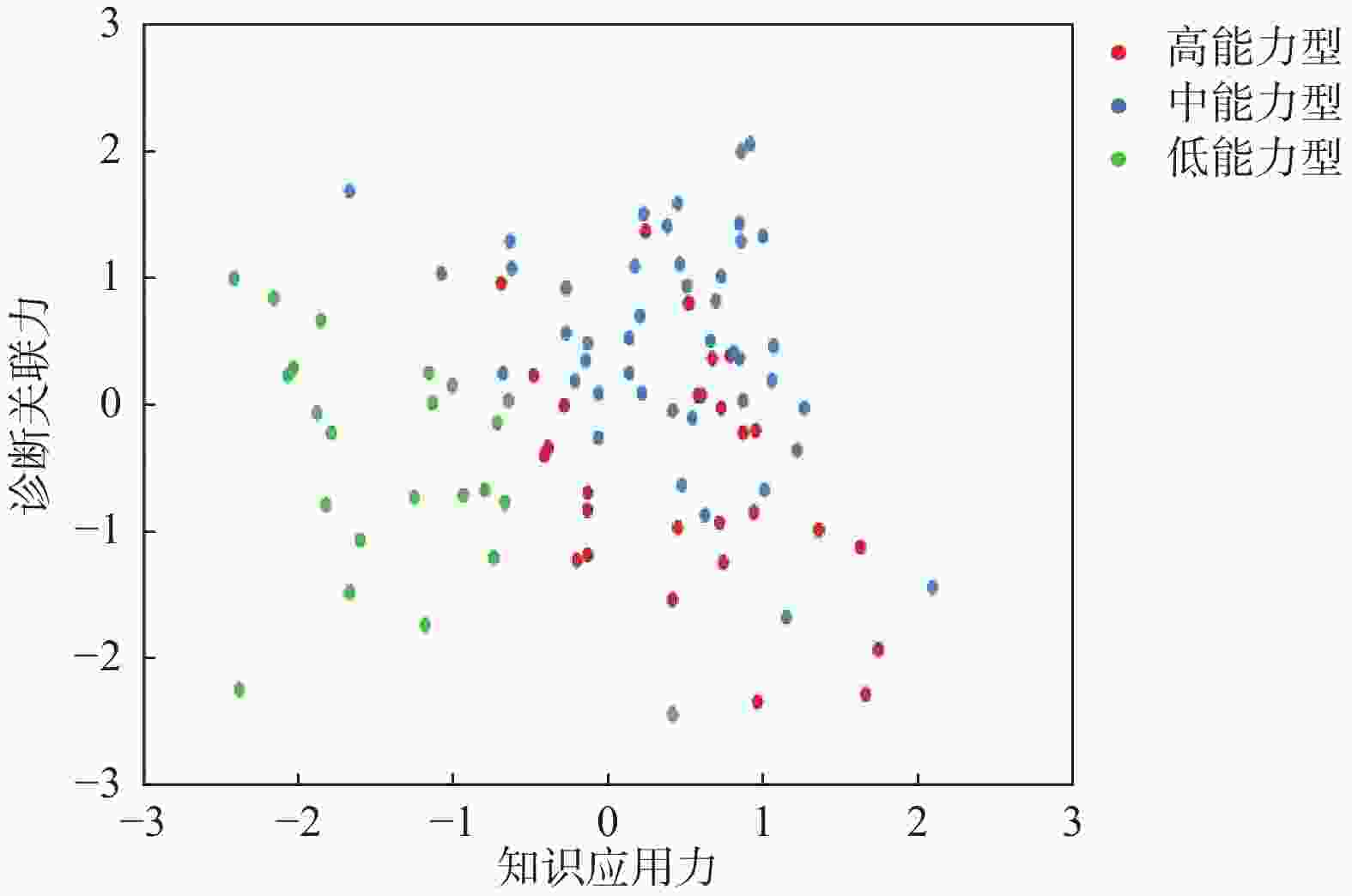
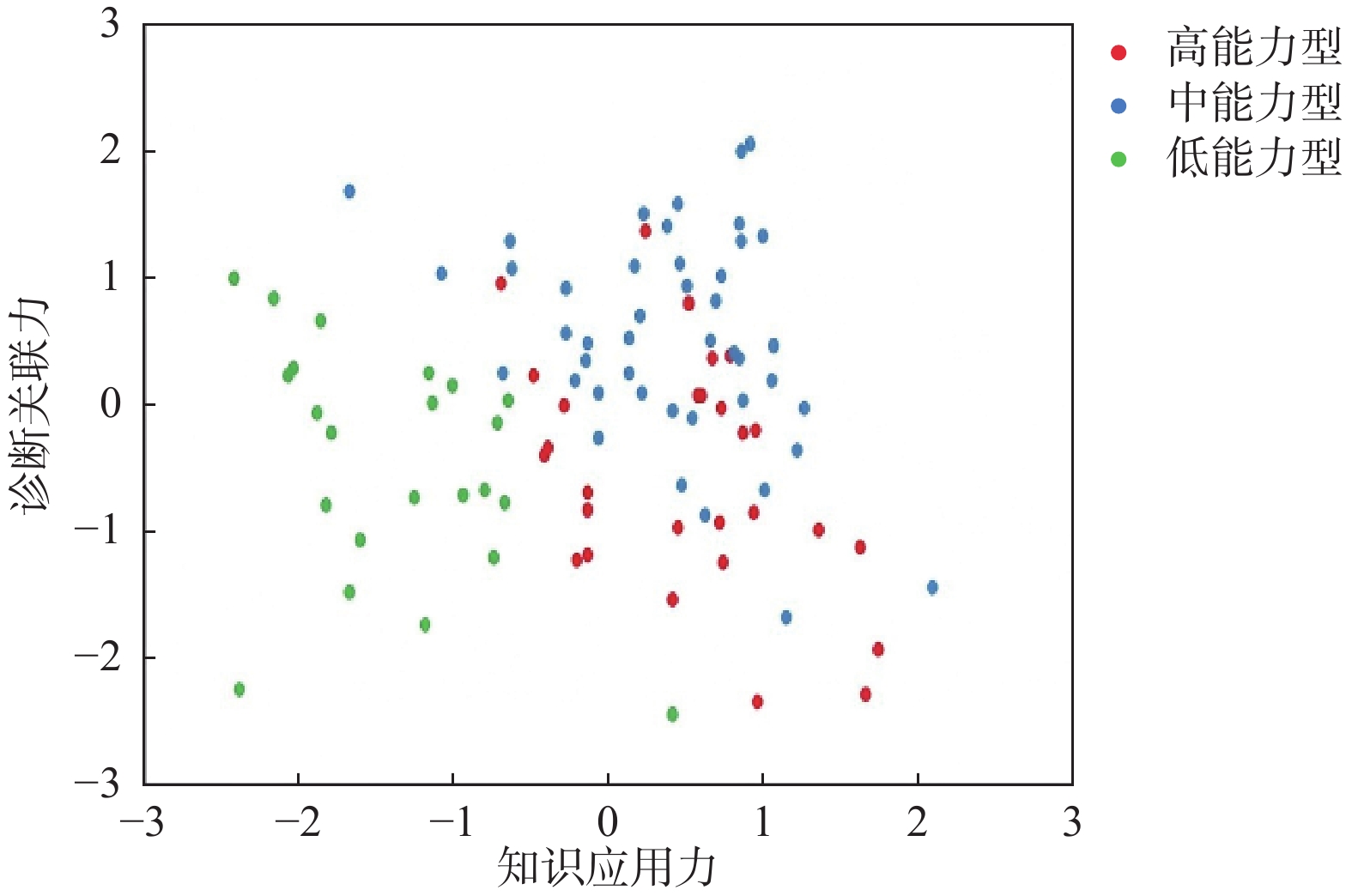
图 1 三类群体知识应用力-诊断关联力分布
Figure 1. Distribution of knowledge application ability-diagnostic relevance among three groups
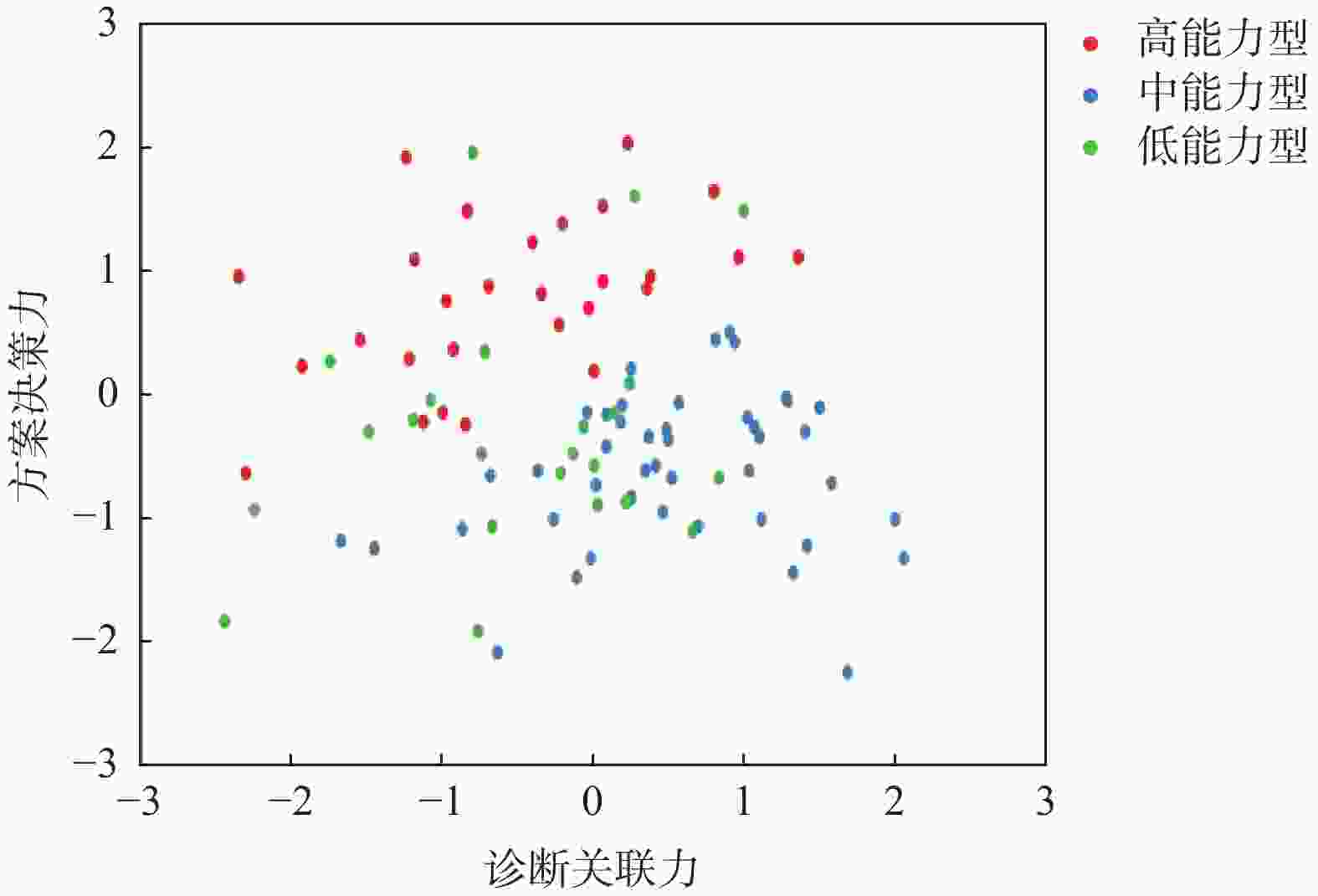
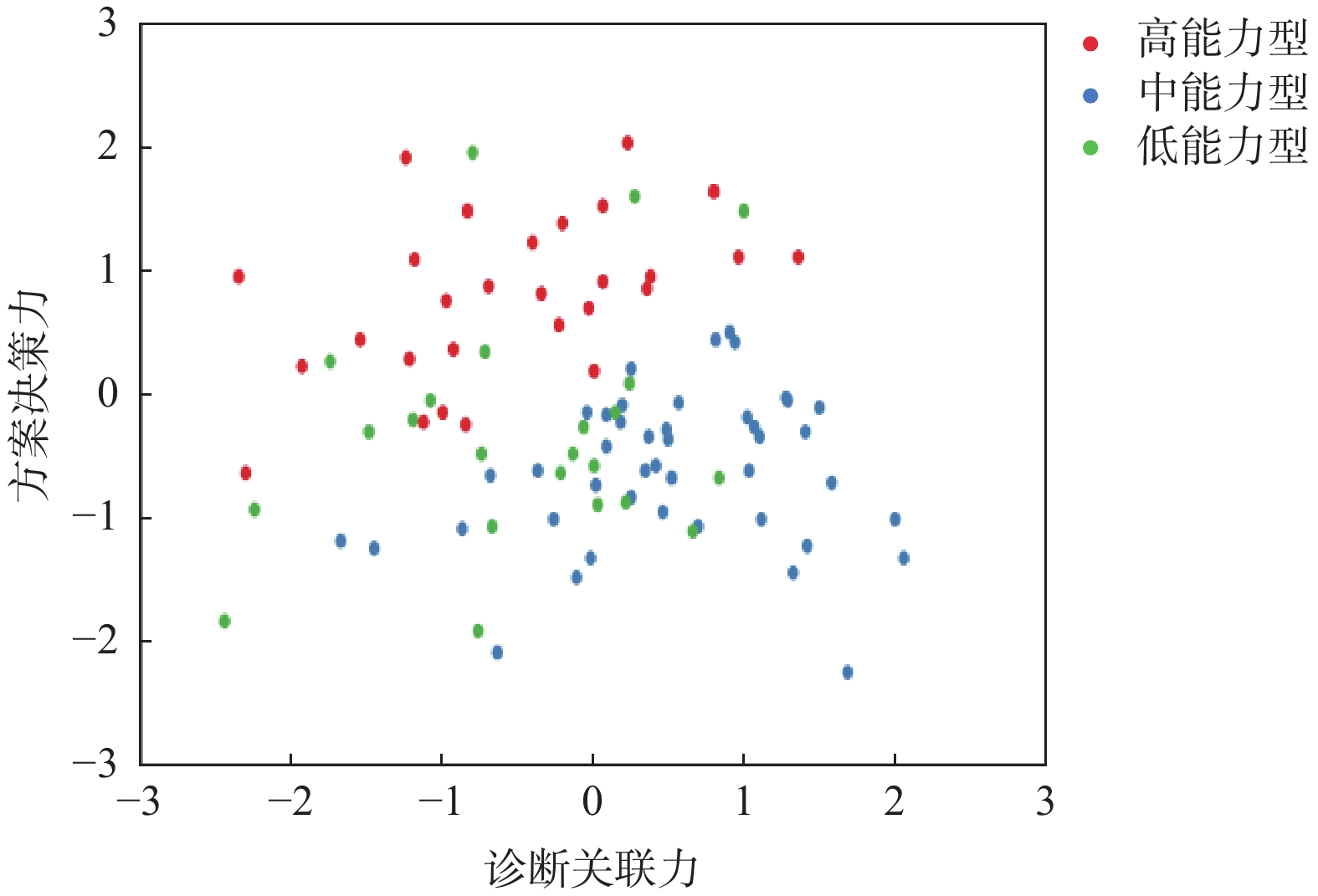
图 2 三类群体诊断关联力-方案决策力分布
Figure 2. Distribution of diagnostic relevance- scheme decision-making ability among three groups
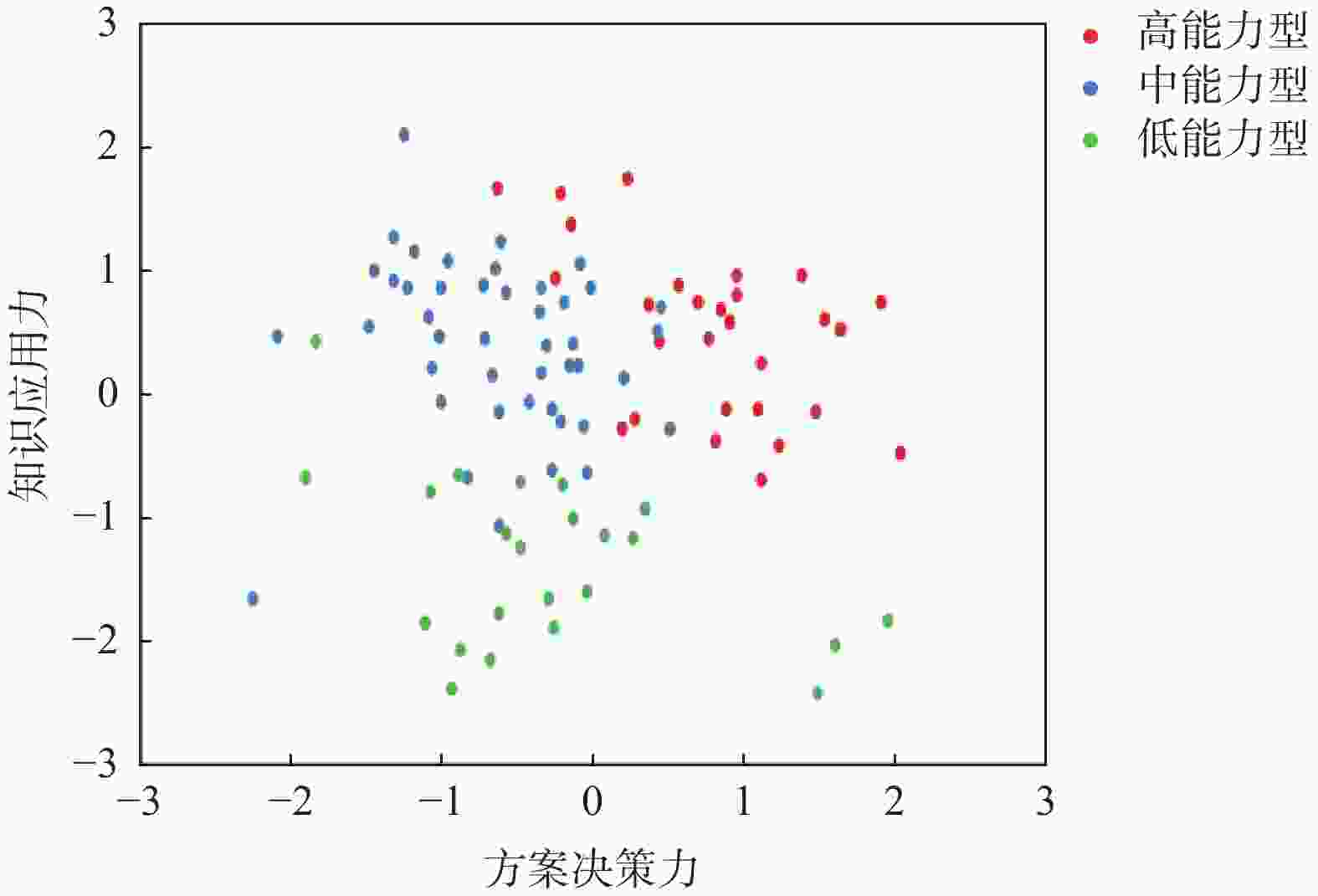
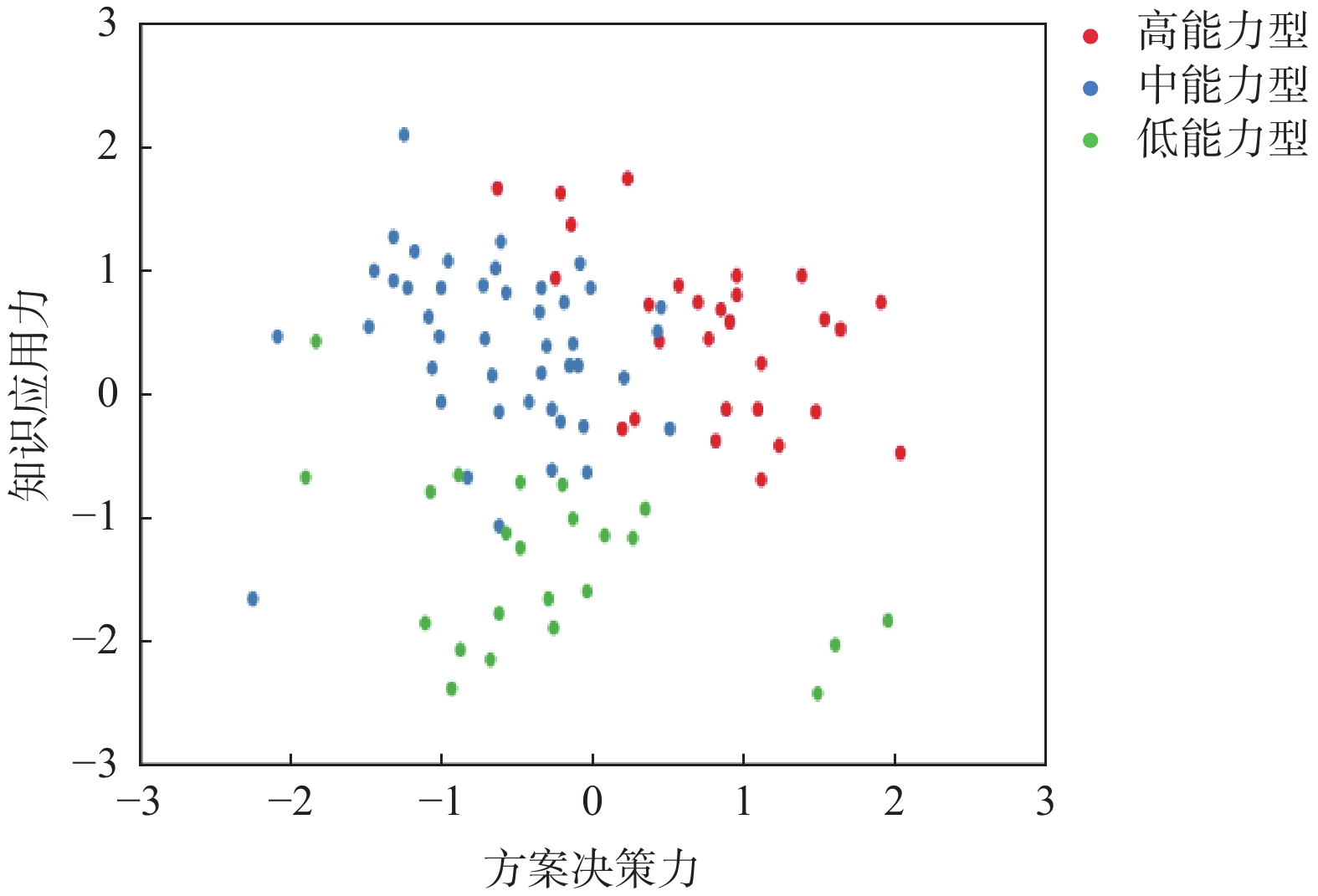
图 3 三类群体方案决策力-知识应用力分布
Figure 3. Distribution of scheme decision-making ability-knowledge application ability among three groups
表 1 诊断关联力维度各指标Pearson相关分析
Table 1. Pearson correlation analysis of each index in the dimension of diagnostic relevance
诊断关联力维度指标 平均值 标准差 归纳主诉信息 症状联系疾病 复杂病例鉴别 归纳主诉信息 3.88 0.95 1 症状联系疾病 3.51 0.89 0.702** 1 复杂病例鉴别 3.18 1.02 0.715** 0.764** 1 **P < 0.01。  下载: 导出CSV
下载: 导出CSV
表 3 知识应用力维度各指标Pearson相关分析
Table 3. Pearson correlation analysis of each index in the dimension of knowledge application ability
知识应用力维度指标 平均值 标准差 查阅文献咨询 分析检查结果 查阅文献咨询 4.08 1.05 1 分析检查结果 3.36 0.98 0.532** 1 **P < 0.01。
下载: 导出CSV
表 2 方案决策力维度各指标Pearson相关分析
Table 2. Pearson correlation analysis of each index in the dimension of scheme decision-making ability
方案决策力维度指标 平均值 标准差 制定治疗方案 逻辑推理自信 定位关键问题 制定治疗方案 3.20 1.02 1 逻辑推理自信 3.35 1.07 0.783** 1 定位关键问题 3.47 1.04 0.736** 0.771** 1 **P < 0.01。
下载: 导出CSV
表 4 临思维能力因子分析方差解释率(%)
Table 4. Factor analysis variance explanation rate of clinical thinking ability (%)
因子编号 特征根 旋转前方差解释率 旋转前累积 旋转前方差解释率 旋转前累积 1 5.52 69.01 69.01 37.89 37.89 2 0.72 9.03 78.04 28.92 66.81 3 0.51 6.04 84.44 17.40 84.21 4 0.40 5.02 89.46 − − 5 0.29 3.65 93.11 − − 6 0.23 2.91 96.02 − − 7 0.19 2.42 98.44 − − 8 0.13 1.56 100.00 − −
下载: 导出CSV
表 5 临床思维能力因子分析旋转后载荷系数
Table 5. Rotated loading coefficients of factor analysis for clinical thinking ability
名称 因子载荷系数 共同度(公因子方差) 因子1 因子2 因子3 归纳主诉信息 0.285 0.878 0.195 0.879 症状联系疾病 0.448 0.663 0.412 0.796 复杂病例鉴别 0.668 0.621 0.205 0.859 制定治疗方案 0.789 0.398 0.257 0.832 逻辑推理自信 0.791 0.478 0.105 0.852 定位关键问题 0.682 0.535 0.185 0.773 查阅文献咨询 0.218 0.248 0.918 0.943 分析检查结果 0.753 0.113 0.481 0.801 注:旋转方法:最大方差法Varimax。
下载: 导出CSV
表 6 三类能力群体各维度得分方差分析对比($ \bar x \pm s $,分)
Table 6. Comparison of variance analysis of dimension scores among three ability groups ($ \bar x \pm s $,Score)
能力维度指标 高能力型(n=107) 中能力型(n=137) 低能力型 (n=77) F P 知识应用力 0.49 ± 0.59 0.38 ± 0.68 −1.36 ± 0.66 215.68 0.000** 诊断关联力 −0.30 ± 0.96 0.54 ± 0.81 −0.51 ± 0.90 43.87 0.000** 方案决策力 0.97 ± 0.66 −0.59 ± 0.62 −0.26 ± 0.93 147.82 0.000** 分层分析(三级医院n = 232) 知识应用力 0.50 ± 0.58 0.39 ± 0.67 −1.35 ± 0.65 152.36 0.000** 诊断关联力 −0.29 ± 0.95 0.55 ± 0.80 −0.50 ± 0.89 30.62 0.000** 方案决策力 0.98 ± 0.65 −0.58 ± 0.61 −0.25 ± 0.92 104.57 0.000** 分层分析(二级医院n = 89) 知识应用力 0.46 ± 0.61 0.35 ± 0.70 −1.38 ± 0.68 63.29 0.000** 诊断关联力 −0.32 ± 0.98 0.52 ± 0.83 −0.53 ± 0.92 13.25 0.000** 方案决策力 0.94 ± 0.68 −0.61 ± 0.64 −0.28 ± 0.95 43.25 0.000** **P < 0.01。
下载: 导出CSV
表 7 三类能力群体8项指标得分差异比较($ \bar x \pm s $,分)
Table 7. Comparison of score differences of 8 indicators among three groups ($ \bar x \pm s $,scores)
指标 高能力型(n = 107) 中能力型(n = 137) 低能力型(n = 77) F P 归纳主诉信息 3.96 ± 0.91 4.22 ± 0.71 3.10 ± 0.99 42.05 0.000** 症状联系疾病 3.91 ± 0.88 3.67 ± 0.66 2.62 ± 0.70 69.83 0.000** 复杂病例鉴别 3.69 ± 1.06 3.19 ± 0.87 2.38 ± 0.75 44.78 0.000** 制定治疗方案 4.02 ± 0.78 2.98 ± 0.83 2.42 ± 0.86 90.87 0.000** 逻辑推理自信 4.05 ± 0.99 3.15 ± 0.80 2.70 ± 1.10 49.98 0.000** 定位关键问题 4.02 ± 1.03 3.45 ± 0.77 2.70 ± 1.06 43.46 0.000** 查阅文献咨询 4.66 ± 0.53 4.45 ± 0.68 2.54 ± 0.64 291.35 0.000** 分析检查结果 4.27 ± 0.68 3.13 ± 0.66 2.46 ± 0.81 154.02 0.000** **P < 0.01。
下载: 导出CSV
表 8 干预前两组临床思维能力基线比较($ \bar x \pm s $,分)
Table 8. Baseline comparison of clinical thinking ability between two groups before intervention ($ \bar x \pm s $,scores)
能力群体 组别 n 诊断关联力 方案决策力 知识应用力 问卷总分 案例考核得分 高能力型 干预组 30 3.95 ± 0.90 4.03 ± 0.77 4.65 ± 0.52 12.63 ± 1.85 82.42 ± 7.51 对照组 30 3.97 ± 0.92 4.01 ± 0.79 4.63 ± 0.54 12.61 ± 1.88 82.36 ± 7.55 t 0.08 0.09 0.15 0.04 0.03 P 0.936 0.928 0.881 0.968 0.976 中能力型 干预组 30 3.66 ± 0.65 2.97 ± 0.82 4.44 ± 0.67 11.07 ± 1.74 68.38 ± 8.15 对照组 30 3.68 ± 0.67 2.99 ± 0.84 4.46 ± 0.69 11.13 ± 1.76 68.45 ± 8.12 t 0.12 0.09 0.11 0.14 0.03 P 0.905 0.928 0.913 0.888 0.976 低能力型 干预组 30 2.61 ± 0.70 2.41 ± 0.85 2.53 ± 0.63 7.55 ± 1.88 52.62 ± 9.30 对照组 30 2.63 ± 0.72 2.43 ± 0.87 2.55 ± 0.65 7.61 ± 1.90 52.71 ± 9.33 t 0.10 0.08 0.12 0.13 0.04 P 0.920 0.936 0.905 0.896 0.968
下载: 导出CSV
表 9 干预前后两组临床思维能力变化比较($ \bar x \pm s $)
Table 9. Comparison of changes in clinical thinking ability between two groups before and after intervention ($ \bar x \pm s $)
能力群体 组别 时间点 诊断关联力 方案决策力 知识应用力 问卷总分 案例考核得分 高能力型 干预组 T0 3.95 ± 0.90 4.03 ± 0.77 4.65 ± 0.52 12.63 ± 1.85 82.42 ± 7.51 T1 4.52 ± 0.86** 4.28 ± 0.75 4.82 ± 0.50 13.62 ± 1.78** 89.65 ± 6.82** 对照组 T0 3.97 ± 0.92 4.01 ± 0.79 4.63 ± 0.54 12.61 ± 1.88 82.36 ± 7.55 T1 4.12 ± 0.91 4.15 ± 0.77 4.71 ± 0.52 12.98 ± 1.82 84.25 ± 7.48 组间T1差异(F/P) 32.67**/0.002 2.81/0.356 2.53/0.281 30.15**/0.003 45.82**/0.001 中能力型 干预组 T0 3.66 ± 0.65 2.97 ± 0.82 4.44 ± 0.67 11.07 ± 1.74 68.38 ± 8.15 T1 3.98 ± 0.63** 3.78 ± 0.76** 4.68 ± 0.65 12.56 ± 1.62** 76.82 ± 7.65** 对照组 T0 3.68 ± 0.67 2.99 ± 0.84 4.46 ± 0.69 11.13 ± 1.76 68.45 ± 8.12 T1 3.75 ± 0.66 3.22 ± 0.80 4.55 ± 0.67 11.52 ± 1.70 71.36 ± 7.88 组间T1差异(F/P) 8.64*/0.032 48.32**/0.001 2.47/0.295 42.76**/0.001 38.95**/0.002 低能力型 干预组 T0 2.61 ± 0.70 2.41 ± 0.85 2.53 ± 0.63 7.55 ± 1.88 52.62 ± 9.30 T1 3.25 ± 0.68** 2.98 ± 0.81** 3.38 ± 0.61** 8.61 ± 1.75** 63.45 ± 8.72** 对照组 T0 2.63 ± 0.72 2.43 ± 0.87 2.55 ± 0.65 7.61 ± 1.90 52.71 ± 9.33 T1 2.82 ± 0.71 2.65 ± 0.83 2.86 ± 0.64 8.33 ± 1.82 56.82 ± 9.05 组间T1差异(F/P) 35.29**/0.001 6.78*/0.028 41.56**/0.001 5.83*/0.035 49.21**/0.001 与同组T0比较,*P < 0.05;**P < 0.01;组间T1差异为方差分析结果;F值后标注*/**表示组间差异的统计学显著性,*P < 0.05;**P < 0.01;P为精确统计值。
下载: 导出CSV
-
[1] 金刚, 朴美花, 李治国, 等. 构建以病例为中心的临床思维培养路径探索和实践[J]. 高校医学教学研究(电子版), 2023, 13(3): 21-26. [2] 李新龙, 朱爽, 刘岩, 等. 中医临床思维研究热点和趋势可视化分析[J]. 中医教育, 2023, 30(1): 47-52. doi: 10.19879/j.cnki.1005-5304.202201389 [3] 张洁, 石秀娥, 付晓康, 等. EPC教学模式促进康复治疗专业学生临床实践教学效果[J]. 医学教育研究与实践, 2024, 32(1): 27-31. doi: 10.13555/j.cnki.c.m.e.2024.01.006 [4] 毕敬涛, 刘亚奇, 郑志学, 等. 结构化临床思维训练在外科医师培养中的应用研究[J]. 医学与哲学, 2025, 46(8): 61-64. doi: 10.12014/j.issn.1002-0772.2025.08.13 [5] Wong K, Faygnersh A, Traba C, et al. Using ChatGPT in the development of clinical reasoning cases: A qualitative study[J]. Cureus, 2024, 16(10): e11446. [6] Thomas MK, Meany B, Fenn J, et al. Development and assessment of simulation-based point-of-care ultrasound training for medical students[J]. Journal of Medical Education and Curricular Development, 2023, 10: 1-10. [7] Durning S J, Artino AR Jr, Schuwirth L, van der Vleuten C. Clarifying Assumptions to Enhance Our Understanding and Assessment of Clinical Reasoning[J]. Academic Medicine, 2013, 88(4): 442-448. [8] 宋一帆, 韩庆烽, 肖卫忠, 等. 基于德尔菲法的全科住院医师临床思维能力评价体系构建研究[J]. 中国全科医学, 2025, 28(1): 77-82. doi: 10.12114/j.issn.1007-9572.2023.0471 [9] 杨玲, 杜雪平. Murtagh安全诊断策略联合思维导图构建临床思维在全科教学门诊中的应用[J]. 中国全科医学, 2025, 28(6): 673-680. [10] Li Yiming, Yang Pinghua, Shi Qin, et al. Construction of an evaluation system for clinical thinking ability of general practitioners in treatment of multimorbidity based on Delphi method[J]. Chin J Gen Pract, 2024, 27(2): 140-145. [11] Durning S J, Jung E, Kim D H, et al. Teaching clinical reasoning: principles from the literature to help improve instruction from the classroom to the bedside[J]. Korean Journal of Medical Education, 2024, 36(3): 189-201. [12] Zhang Y, Li J, Wang H. Python-based intelligent case bank for clinical reasoning training: A pilot study[J]. BMC Med Educ, 2023, 23(1): 45-53. doi: 10.1186/s12909-023-04016-7 [13] Wang L, Zhao J, Huang Y. Validation of a three-dimensional clinical reasoning model: Recognition, decision-making, and application[J]. Acad Med, 2024, 99(2): 312-318. [14] 张云. 基于改进的K-means聚类算法的学生成绩分析[J]. 安徽开放大学学报, 2022, 30(3): 92-96. doi: 10.3969/j.issn.1008-6021.2022.03.018 [15] Gordon D, Rencic J, Lang V J, et al. Advancing the assessment of clinical reasoning across the health professions: Definitional and methodologic recommendations[J]. Med Educ, 2022, 56(1): 3-14. [16] 邹健, 李阳, 陈丽莉. 批判性思维在浙江大学临床医学教育中的应用探讨[J]. 全科医学临床与教育, 2023, 21(12): 1107-1110. doi: 10.13558/j.cnki.issn1672-3686.2023.012.015 [17] 邱艳, 叶康丽, 刘颖, 等. 分级分层培养在全科住院医师临床思维能力培养中的效果评价[J]. 医学教育研究与实践, 2022, 30(6): 691-694. doi: 10.13555/j.cnki.c.m.e.2022.06.004 [18] Humbert A J, Besinger B, Miech E J, et al. Assessing clinical reasoning skills in scenarios of uncertainty: Convergent validity for a script concordance test in an emergency medicine clerkship and residency[J]. Academic Emergency Medicine, 2011, 18(6): 627-634. doi: 10.1111/j.1553-2712.2011.01084.x [19] Wan M, Tor E, Hudson J N. Examining response process validity of script concordance testing: A think-aloud approach[J]. International Journal of Medical Education, 2020, 11: 127-135. doi: 10.5116/ijme.5eb6.7be2 [20] 沙宗硕, 渠瀚云, 张昕欣, 等. 人工智能赋能中医药课程思政案例库建设与实践路径研究[J]. 中国医药导报, 2025, 22(26): 1-6. doi: 10.20047/j.issn1673-7210.2025.26.01 [21] 赵世军, 孔亮, 赵伟娜, 等. “双碳”背景下“计算力学”教学改革-基于Python语言程序设计[J]. 教育教学论坛, 2024(50): 69-72. [22] 周丽涛, 谷振兴, 戴傲, 等. 大规模在线时间教学平台基于能力培养的创新应用于探索[J]. 计算机教育, 2024, (7): 20-25. [23] 田晨智, 宋敏, 田继伟, 等. 基于眼动追踪的指挥控制系统人机交互效能评估方法[J]. 航空兵器, 2023, 30(4): 57-66. doi: 10.12132/ISSN.1673-5048.2023.0008 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 634
- HTML全文浏览量: 347
- PDF下载量: 47
- 被引次数: 0
