

Serological Features of Neurological Involvement in ANCA-associated Vasculitis and Their Predictive Value for Prognosis
-
摘要:
目的 探讨抗中性粒细胞胞浆抗体(antineutrophil cytoplasmic antibody,ANCA)相关性血管炎患者神经系统受累情况与核周型抗中性粒细胞胞浆抗体(perinuclear anti-neutrophil cytoplasmic antibody,p-ANCA)、血沉(erythrocyte sedimentation rate,ESR)、髓过氧化物酶(myeloperoxidase,MPO)-免疫球蛋白G(immunoglobulin G,IgG)抗体及C反应蛋白(C-reactive protein,CRP)水平之间的差异及其对预后的预测价值。 方法 选取2020年1月至2024年11月于浙江大学医学院附属第一医院收治的106例ANCA相关性血管炎患者,根据预后分为预后良好组与不良组。采用倾向性评分匹配(propensity score matching,PSM)法减少基线差异。比较不同预后及神经系统是否受累患者的p-ANCA阳性率及ESR、MPO-IgG抗体、CRP水平差异;应用多因素Logistic回归分析上述指标与患者预后的关系,并利用ROC曲线分析各指标及联合检测对预后的预测效能。 结果 预后不良组患者的p-ANCA阳性率及ESR、MPO-IgG抗体、CRP水平均明显高于良好组(P < 0.05);神经系统受累患者的上述指标也明显高于未受累患者(P < 0.05)。多因素Logistic回归分析显示,p-ANCA阳性、ESR、MPO-IgG抗体和CRP均为影响患者预后的独立预测因素,尤其在神经系统受累患者中影响更显著(OR值更大,P < 0.05)。ROC曲线分析显示,各单项指标预测预后的AUC在0.675~0.780之间,联合预测的AUC高达0.922,明显优于单项指标的预测效果(P < 0.05)。联合的AUC值显著大于单独的p-ANCA、ESR、MPO-IgG、CRP(Z = 4.813、3.414、2.508、2.291,P < 0.001、P = 0.001、P = 0.012、P = 0.022)。 结论 p-ANCA阳性率和ESR、MPO-IgG抗体、CRP水平升高与ANCA相关性血管炎患者的神经系统损害及不良预后密切相关。 -
关键词:
- 抗中性粒细胞胞浆抗体相关性血管炎 /
- 神经系统受累 /
- 核周型抗中性粒细胞胞浆抗体 /
- 血沉 /
- 髓过氧化物酶IgG抗体 /
- C反应蛋白
Abstract:Objective To explore the relationship between neurological involvement in patients with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis and the difference of serum levels of perinuclear anti-neutrophil cytoplasmic antibody (p-ANCA), erythrocyte sedimentation rate (ESR), myeloperoxidase immunoglobulin G antibodies (MPO-IgG) and C-reactive protein (CRP), as well as their predictive value for the prognosis. Methods A total of 106 patients with ANCA-associated vasculitis admitted to the First Affiliated Hospital of Zhejiang University School of Medicine from January 2020 to November 2024 were selected and divided into good prognosis group and poor prognosis group according to the prognosis. Propensity score matching (PSM) was used to reduce baseline differences. The positive rate of p-ANCA and the levels of ESR, MPO-IgG antibody and CRP in patients with different prognosis and neurological involvement were compared. Multivariate Logistic regression was used to analyze the relationship between the above indicators and the prognosis of patients, and ROC curve was used to analyze the predictive efficacy of each indicator and combined detection on prognosis. Results The positive rate of p-ANCA and the levels of ESR, MPO-IgG antibody and CRP in the poor prognosis group were significantly higher than those in the good prognosis group (P < 0.05). The above indexes in patients with neurological involvement were also significantly higher than those in patients without involvement (P < 0.05). Multivariate logistic regression analysis showed that p-ANCA positive, ESR, MPO-IgG antibody and CRP were independent predictors of prognosis, especially in patients with neurological involvement (greater OR value, P < 0.05). ROC curve analysis showed that AUC of each single index in predicting prognosis was between 0.675 and 0.780, and AUC of combined prediction was as high as 0.922, which was significantly better than that of single index (P < 0.05). The combined AUC values were significantly greater than p-ANCA, ESR, MPO-IgG, and CRP alone (Z = 4.813, 3.414, 2.508, 2.291, P < 0.001, P = 0.001, P = 0.012, P = 0.022). Conclusion The positive rate of p-ANCA and the levels of ESR, MPO-IgG antibody and CRP are closely related to the neurological involvement and poor prognosis in patients with ANCA-associated vasculitis. -
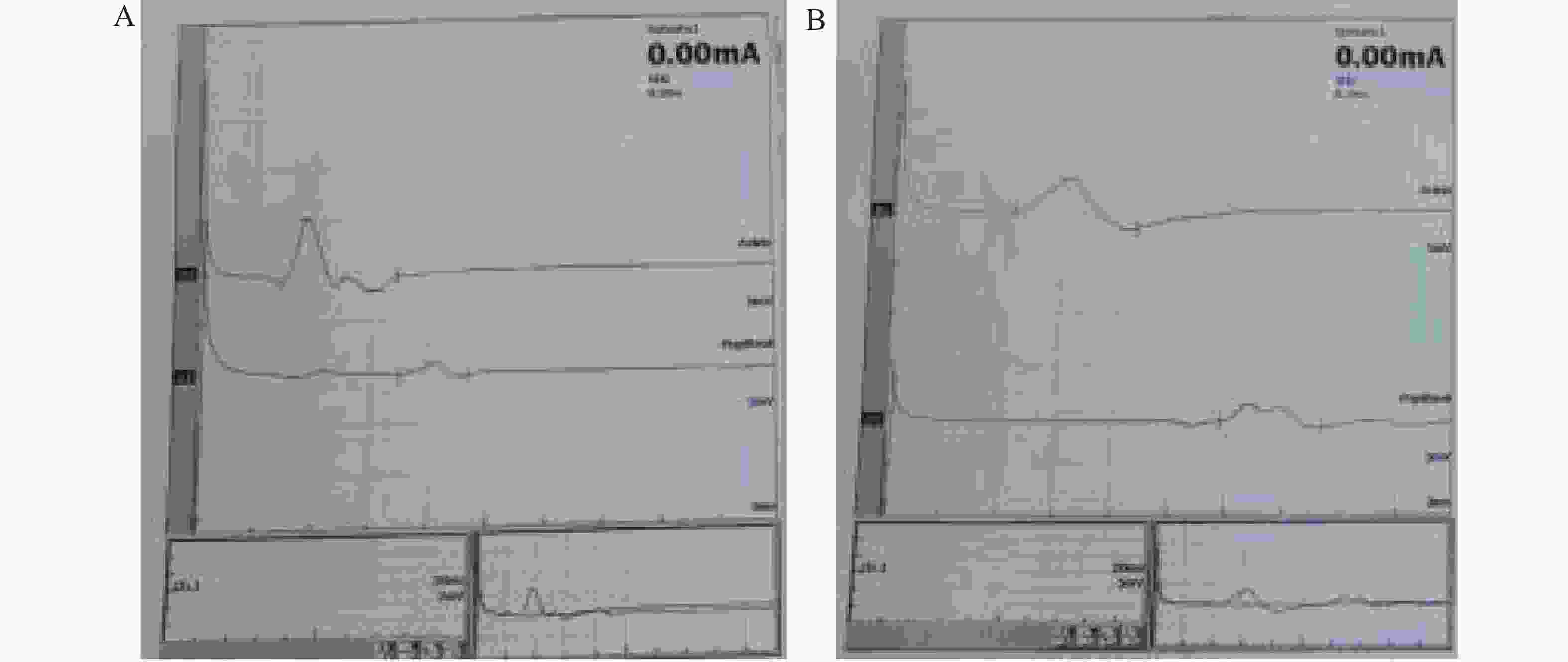
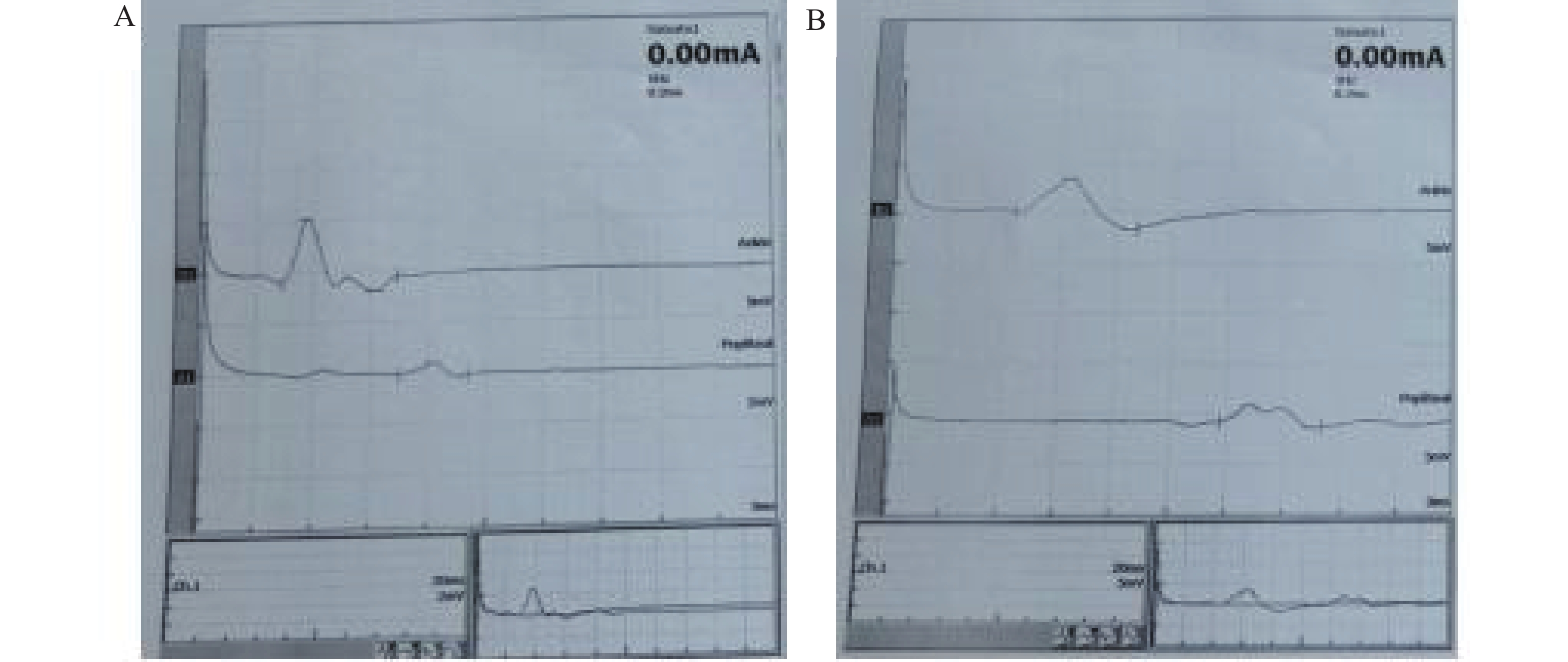
图 1 神经系统受累患者的表现
A:左侧胫神经;B:右侧胫神经,传导速度减慢,潜伏期延长,CMAP波幅低,F波潜伏期延长;(注:患者女,70岁,肌电图/诱发电位显示)。
Figure 1. Manifestations of patients with neurological involvement
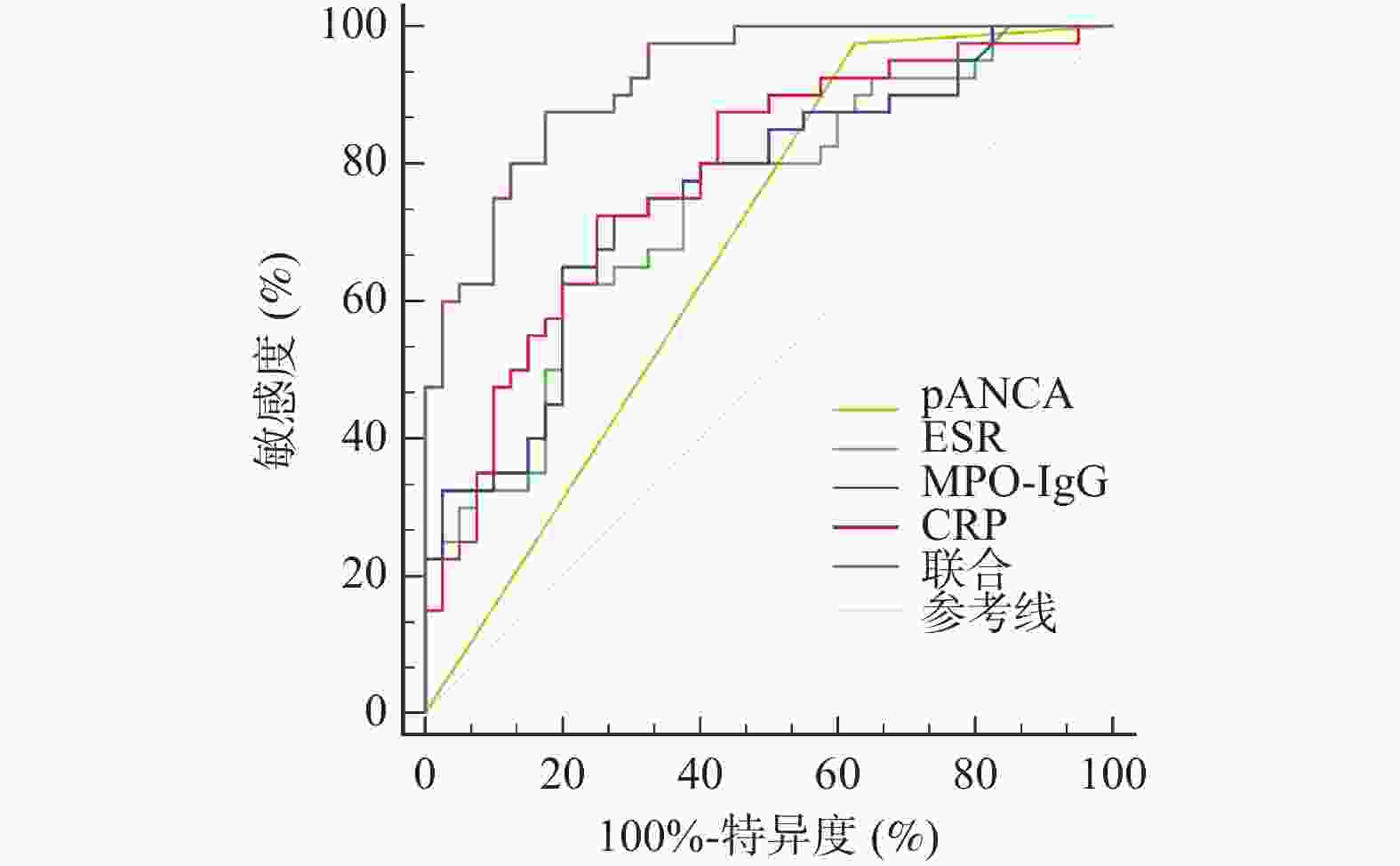
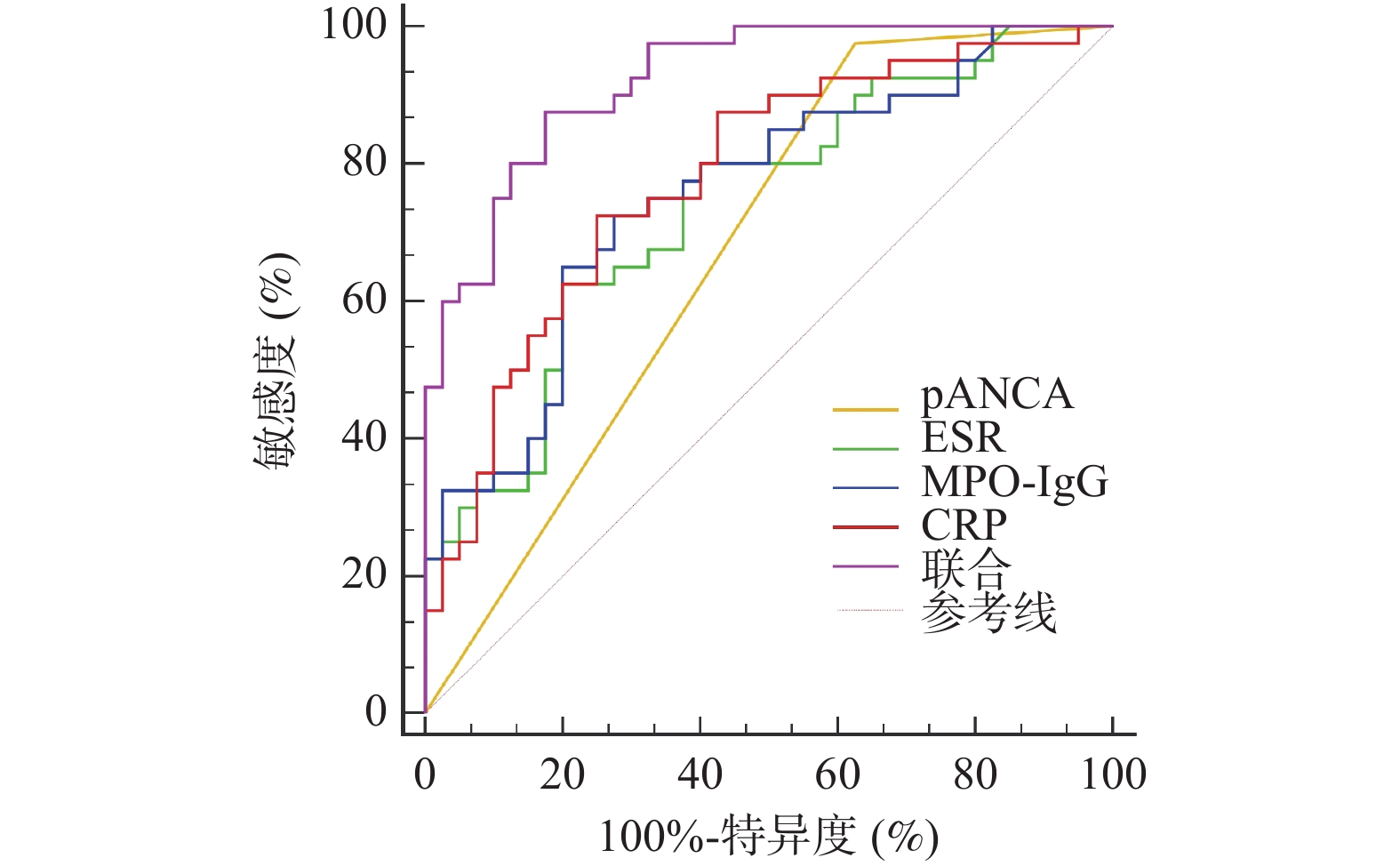
图 2 p-ANCA、ESR、MPO-IgG、CRP预测预后的价值
Figure 2. The value of p-ANCA,ESR,MPO-IgG and CRP in predicting prognosis
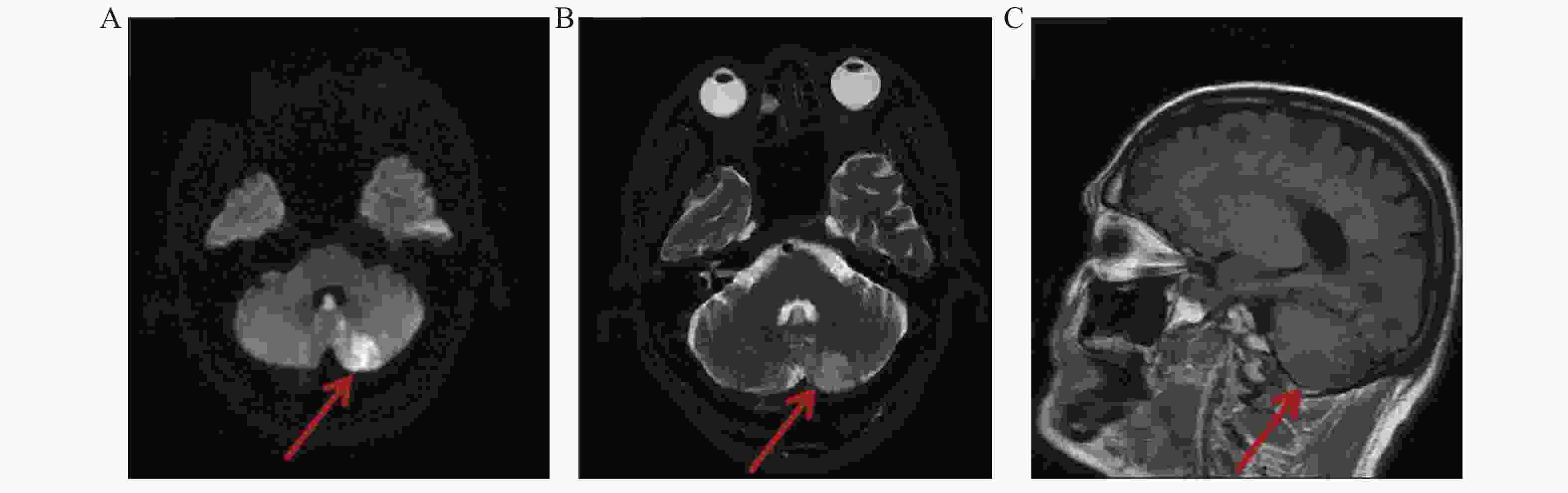
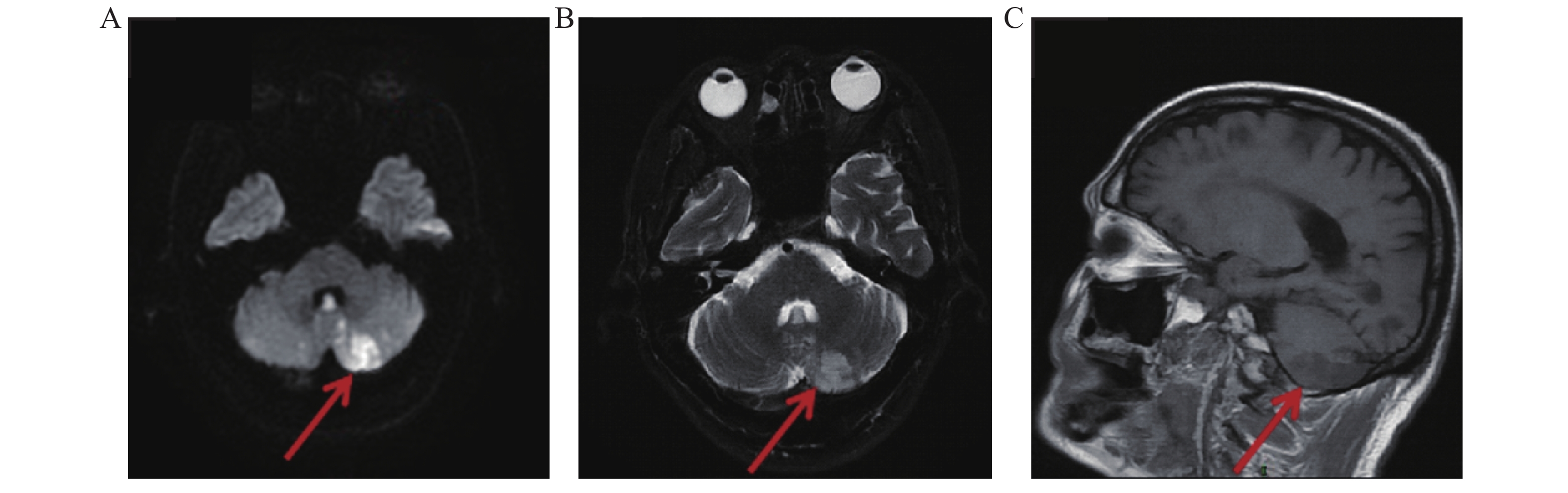
图 3 部分患者神经影像学的表现
A:左侧小脑半球DWI高信号影;B:T2压脂呈稍高信号影;C:矢状位T1FLAIR呈低信号影。
Figure 3. Neuroimaging manifestations of some patients
表 1 PSM前后两组患者基线资料比较[($ \bar x \pm s $)/n(%)]
Table 1. Comparison of baseline data between the two groups before and after PSM [($ \bar x \pm s $)/n(%)]
PSM前 组别 年龄(岁) 性别 BMI
(kg/m2)糖尿病 高血压 冠心病 高脂血症 肾受累 肺受累 ANCA滴度
(RU/mL)BVAS评分
(分)疾病分型 血红蛋白
(g/L)血小板
(×109/L)治疗 男 女 MPA GPA 利妥昔单抗 环磷酰胺 血浆置换 不良组
(n = 40)63.22±8.11 16
(40.00)24
(60.00)23.91±1.15 8
(20.00)11
(27.50)5
(12.50)14
(35.00)29
(72.50)21
(52.50)112.56±20.38 21.45±3.88 37
(92.50)3
(7.50)81.88±14.76 245.22±20.19 12
(30.00)31
(77.50)4
(10.00)良好组
(n = 66)61.90±9.45 22
(33.33)44
(66.67)24.02±0.87 9
(13.64)13
(19.70)4
(6.06)18
(27.27)26
(39.39)19
(28.79)109.74±22.75 17.94±5.13 60
(90.91)6
(9.09)84.59±16.43 242.96±23.15 16
(24.24)49
(74.24)2
(3.03)t/χ2 0.734 0.481 0.588 0.749 0.866 0.630 0.706 10.934 5.960 0.643 3.727 0.006 −0.855 0.511 0.425 0.143 1.148 P 0.464 0.488 0.578 0.387 0.352 0.428 0.401 0.001# 0.015# 0.522 <0.001* 0.941 0.395 0.611 0.515 0.706 0.284 SMD 0.150 0.139 0.109 0.170 0.183 0.219 0.167 0.691 0.494 0.129 0.772 0.058 0.173 0.103 0.130 0.076 0.278 PSM后 组别 年龄(岁) 性别 BMI
(kg/m2)糖尿病 高血压 冠心病 高脂血症 肾受累 肺受累 ANCA滴度
(RU/mL)BVAS评分
(分)疾病分型 血红蛋白
(g/L)血小板
(×109/L)治疗 男 女 MPA GPA 利妥昔单抗 环磷酰胺 血浆置换 不良组
(n = 40)63.22±8.11 16
(40.00)24
(60.00)23.91±1.15 8
(20.00)11
(27.50)5
(12.50)14
(35.00)29
(72.50)21
(52.50)112.56±20.38 21.45±3.88 37
(92.50)3
(7.50)81.88±14.76 245.22±20.19 12
(30.00)31
(77.50)4
(10.00)良好组
(n = 40)62.50±9.38 20
(50.00)20
(50.00)23.96±1.03 5
(12.50)9
(22.50)2
(5.00)17
(42.50)23
(57.50)15
(37.50)110.56±19.78 20.87±4.93 38
(95.00)2
(5.00)82.59±13.84 243.86±19.51 9
(22.50)28
(70.00)1
(2.50)t/χ2 0.367 0.808 −0.205 0.827 0.267 0.626 0.474 1.978 1.818 0.445 0.585 <0.001 −0.222 0.306 0.581 0.581 0.853 P 0.714 0.369 0.838 0.363 0.606 0.429 0.491 0.160 0.178 0.657 0.560 1.000 0.825 0.760 0.446 0.446 0.356 SMD 0.082 0.091 0.046 0.073 0.015 0.067 0.053 0.015 0.023 0.099 0.030 0.098 0.050 0.068 0.070 0.070 0.092 #P < 0.05,*P < 0.001。  下载: 导出CSV
下载: 导出CSV
表 2 两组患者治疗前p-ANCA、ESR、MPO-IgG、CRP比较[($ \bar x \pm s $)/n(%)]
Table 2. Comparison of p-ANCA,ESR,MPO-IgG and CRP between the two groups of patients before treatment [($ \bar x \pm s $)/n(%)]
组别 n pANCA阳性 ESR(mm/h) MPO-IgG(U/mL) CRP(mg/L) 不良组 40 39(97.50) 75.26 ± 24.88 94.00 ± 29.78 87.40 ± 28.40 良好组 40 25(62.50) 49.40 ± 16.29 71.65 ± 22.54 66.56 ± 20.19 t/χ2 15.313 5.500 3.785 3.783 P <0.001* <0.001* <0.001* <0.001* *P < 0.001。
下载: 导出CSV
表 3 两组患者治疗后p-ANCA、ESR、MPO-IgG、CRP比较[($ \bar x \pm s $)/n(%)]
Table 3. Comparison of p-ANCA,ESR,MPO-IgG and CRP between the two groups of patients after treatment [($ \bar x \pm s $)/n(%)]
组别 n pANCA阳性 ESR(mm/h) MPO-IgG(U/mL) CRP(mg/L) 不良组 40 36(90.00) 58.33 ± 19.15 85.10 ± 25.66 65.35 ± 21.17 良好组 40 18(45.00) 28.15 ± 9.22 45.20 ± 15.04 18.75 ± 6.23 t/χ2 18.462 8.981 8.484 13.355 P <0.001* <0.001* <0.001* <0.001* *P < 0.001。
下载: 导出CSV
表 4 神经系统受累与否患者治疗前p-ANCA、ESR、MPO-IgG、CRP水平差异性比较[($ \bar x \pm s $)/n(%)]
Table 4. Comparison of p-ANCA,ESR,MPO-IgG,CRP level differences in patients with or without neurological involvement before treatment [($ \bar x \pm s $)/n(%)]
组别 n p-ANCA阳性 ESR(mm/h) MPO-IgG(U/mL) CRP(mg/L) 受累 59 51(86.44) 70.95 ± 21.24 90.66 ± 21.53 83.44 ± 21.56 未受累 21 13(61.90) 38.11 ± 11.78 60.83 ± 19.96 58.83 ± 18.20 t/χ2 4.395 6.709 5.554 4.667 P 0.036* <0.001* <0.001* <0.001* *P < 0.001。
下载: 导出CSV
表 5 治疗前p-ANCA、ESR、MPO-IgG、CRP对预后的影响
Table 5. Effect of p-ANCA,ESR,MPO-IgG and CRP on prognosis before treatment
影响因素 β SE Wald χ2 OR 95%CI P 下限 上限 神经系统受累 pANCA阳性 1.383 0.315 19.263 3.985 3.115 5.098 <0.001* ESR 0.293 0.082 12.795 1.341 1.234 1.457 <0.001* MPO-IgG 0.325 0.095 11.712 1.384 1.196 1.602 <0.001* CRP 0.245 0.062 15.576 1.277 1.177 1.386 <0.001* 神经系统未受累 p-ANCA阳性 1.138 0.227 25.147 3.122 2.368 4.115 <0.001* ESR 0.187 0.059 10.068 1.206 1.086 1.339 <0.001* MPO-IgG 0.139 0.043 10.458 1.149 1.002 1.318 <0.001* CRP 0.096 0.026 13.661 1.101 1.015 1.194 <0.001* *P < 0.001。
下载: 导出CSV
表 6 p-ANCA、ESR、MPO-IgG、CRP预测预后的价值
Table 6. The value of p-ANCA,ESR,MPO-IgG and CRP in predicting prognosis
指标 AUC 95%CI cut-off值 敏感度(%) 特异度(%) P p-ANCA 0.675 0.561~0.776 阳性 97.50 37.50 <0.001* ESR 0.740 0.630~0.831 68.53 62.50 80.00 <0.001* MPO-IgG 0.756 0.647~0.845 85.45 65.00 80.00 <0.001* CRP 0.780 0.673~0.865 75.68 72.50 75.00 <0.001* 联合 0.922 0.840~0.970 − 87.50 82.50 <0.001* *P < 0.001。
下载: 导出CSV
-
[1] Kidney disease: Improving Global Outcomes (KDIGO) ANCA Vasculitis Work Group. KDIGO 2024 clinical practice guideline for the management of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis[J]. Kidney Int, 2024, 105(3S): S71-S116. [2] 徐莹, 韩飞. 2024年版KDIGO《ANCA相关性血管炎管理临床实践指南》更新重点内容解读[J]. 中国实用内科杂志, 2024, 44(9): 734-739. doi: 10.19538/j.nk2024090103 [3] Floege J, Jayne D R W, Sanders J F, et al. Executive summary of the KDIGO 2024 clinical practice guideline for the management of ANCA-associated vasculitis[J]. Kidney Int, 2024, 105(3): 447-449. [4] Gong Y, Shen C, Meng T, et al. Clinical features and prognosis of ANCA-associated vasculitis patients who were double-seropositive for myeloperoxidase-ANCA and proteinase 3-ANCA[J]. Clin Exp Med, 2024, 24(1): 66. doi: 10.1007/s10238-024-01318-y [5] Horai Y, Kurushima S, Kawakami A. Current diagnosis and treatment of anti-neutrophil cytoplasmic antibody-associated vasculitis: A review including a comparison of characteristics in Europe and Japan[J]. J Clin Med, 2025, 14(5): 1724. doi: 10.3390/jcm14051724 [6] Gisslander K, White A, Aslett L, et al. Data-driven subclassification of ANCA-associated vasculitis: model-based clustering of a federated international cohort[J]. Lancet Rheumatol, 2024, 6(11): e762-e770. doi: 10.1016/S2665-9913(24)00187-5 [7] Katsumata Y, Sada KE, Kameda T, et al. Comparison of different ANCA detection methods in a predominantly MPO-ANCA-associated vasculitis cohort[J]. Immunol Med, 2025, 48(1): 47-57. doi: 10.1080/25785826.2024.2408054 [8] Ötleş E, Serbest Ceylanoglu K, Demirci H. Bilateral choroidal detachments associated with perinuclear anti-neutrophil cytoplasmic antibodies (P-ANCA) - associated vasculitis[J]. Ocul Immunol Inflamm, 2024, 32(8): 1878-1881. [9] 田新平, 赵丽珂, 姜振宇, 等. 抗中性粒细胞胞质抗体相关血管炎诊疗规范[J]. 中华内科杂志, 2022, 61(10): 1128-1135. doi: 10.3760/cma.j.cn112138-20220318-00191 [10] Nimbvikar A A, Panchawagh S, Chavan A P, et al. Modified rankin scale is a reliable tool for the rapid assessment of stroke severity and predicting disability outcomes[J]. J Family Med Prim Care, 2024, 13(3): 1085-1090. doi: 10.4103/jfmpc.jfmpc_1431_23 [11] Mohammed BT, Uzodi N, Gotimukul A, et al. Case Report of MPO+ ANCA vasculitis with pauci-immune GN associated with Invasive ductal carcinoma of the Breast[J]. Curr Rheumatol Rev, 2024, 20(2): 213-218. doi: 10.2174/0115733971246438230924163114 [12] 张玉琴, 童海玲, 侯晨, 等. 以周围神经病为首发症状的抗中性粒细胞胞浆抗体相关性血管炎的临床特点[J]. 临床神经病学杂志, 2024, 37(3): 197-200. doi: 10.3969/j.issn.1004-1648.2024.03.012 [13] 张雨婷, 陈燕, 冯锦红. AAV中血清MPO、PR3阳性患者的抗体滴度与临床指标间的关系[J]. 国际泌尿系统杂志, 2025, 45(2): 115-119. doi: 10.3760/cma.j.cn431460-20240401-00077 [14] Schönermarck U, Hellmich B, Csernok E. Labordiagnostik bei Vaskulitiden jenseits von antineutrophilen zytoplasmatischen Autoantikörpern [Laboratory diagnostics for vasculitis beyond antineutrophil cytoplasmatic autoantibodies[J]. Z Rheumatol, 2024, 83(4): 283-296. [15] Xie LY, Qiu XY, Li YN, et al. Serum ferritin is a superior biomarker for evaluating disease activity and kidney injury compared with C-reactive protein in anti-neutrophil cytoplasmic antibody-associated vasculitis[J]. Clin Rheumatol, 2025, 44(5): 2009-2021. doi: 10.1007/s10067-025-07412-0 [16] Juto A, Martin M, Björk A, et al. Association of C4d with disease activity in anti-neutrophil cytoplasmic antibody-associated vasculitis: Evidence for classical/lectin complement pathway activation[J]. Arthritis Res Ther, 2025, 27(1): 49. doi: 10.1186/s13075-025-03503-0 [17] Locatelli L, Calatroni M, Reggiani F, et al. Long-term kidney outcome of patients with rheumatological diseases and antineutrophil cytoplasmic antibody-glomerulonephritis: comparison with a primitive ANCA-glomerulonephritis cohort[J]. Clin Exp Rheumatol, 2023, 41(4): 856-863. doi: 10.55563/clinexprheumatol/csk834 [18] 陈倩, 叶俊兵, 郝炎, 等. 103例抗中性粒细胞胞质抗体相关性血管炎的临床特征及预后分析[J]. 国际泌尿系统杂志, 2025, 45(2): 123-129. doi: 10.3760/cma.j.cn431460-20221229-00079 [19] Park P G, Song J J, Park Y B, et al. Clinical application of low erythrocyte sedimentation rate/high C-reactive protein to antineutrophil cytoplasmic antibody-associated vasculitis[J]. J Clin Lab Anal, 2022, 36(2): e24237. [20] Liu S, Guo L, Fan X, et al. Clinical features of central nervous system involvement in patients with eosinophilic granulomatosis with polyangiitis: a retrospective cohort study in China[J]. Orphanet J Rare Dis, 2021, 16(1): 152. doi: 10.1186/s13023-021-01780-x [21] Sherri A, Mortada M M, Makowska J, et al. Primary angiitis of the CNS and ANCA-associated vasculitis: from pathology to treatment[J]. Rheumatol Int, 2024, 44(2): 211-222. doi: 10.1007/s00296-023-05461-9 [22] Alharthi A M, Aljundi Z, Alharbi F A, et al. Prognostic factors and outcome measures after rituximab therapy in central nervous system vasculitis: A systematic review[J]. Cureus, 2024, 16(9): e69936. doi: 10.7759/cureus.69936 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 695
- HTML全文浏览量: 500
- PDF下载量: 134
- 被引次数: 0
