

Clinical Efficacy of V-Shaped Double-channel Spinal Endoscopic Technique (VBE) in Patients with LDH and Lumbar Instability
-
摘要:
目的 以常规经椎间孔椎间融合术(TLIF)为对照,分析V形双通道脊柱内镜技术(VBE)治疗腰椎间盘突出症(LDH)伴腰椎不稳的效果。 方法 选取2021年1月至2023年3月昆明市官渡区人民医院和上海市第十人民医院收治的102例LDH伴腰椎不稳患者,以随机分组软件分为TLIF组(予以TLIF术,n = 51)、VBE组(予以VBE手术,n = 51)。比较2组手术一般情况、围手术期疼痛程度(VAS评分)、手术前后腰痛与下肢痛程度(VAS评分)、腰椎稳定性(椎间隙高度、腰椎前凸角)、减压效果(硬膜囊横断面积、椎间孔面积)、功能预后及并发症情况。 结果 VBE组术中出血量少于TLIF组,切口长度、卧床时间、住院时间短于TLIF组(P < 0.05);VBE组术后6 h、术后12 h、术后24 h、术后48 h、术后72 h的VAS评分低于TLIF组(P < 0.05);术后3、6个月腰痛、下肢痛VAS评分及术后6个月椎间隙高度、腰椎前凸角、硬膜囊横断面积、椎间孔面积高于术前,但组间比较差异无统计学意义(P > 0.05);2组功能预后优良率(98.04%、94.12%)比较,差异无统计学意义(P > 0.05);VBE组无并发症发生,TLIF组1例出现切口渗出。 结论 VBE与TLIF治疗LDH伴腰椎不稳患者,可增强腰椎稳定性,改善患者腰椎功能,确保安全性,而VBE切口小,可减少术中出血,降低术后早期疼痛,加快早期病情恢复。 Abstract:Objective To compare the effectiveness of V-shaped double-channel spine endoscope technology (VBE) in treating lumbar disc herniation (LDH) with lumbar instability with traditional transforaminal lumbar interbody fusion (TLIF). Methods From January 2021 to March 2023, 102 patients with LDH and lumbar instability admitted to the People's Hospital of Guandu District, Kunming City, and the Tenth People's Hospital of Shanghai were selected. They were randomly divided into two groups using random grouping software: the TLIF group (undergoing TLIF surgery, n = 51) and the VBE group (undergoing VBE surgery, n = 51). The two groups were compared in terms of general surgical conditions, perioperative pain levels (VAS scores), pre- and postoperative levels of back and leg pain (VAS scores), lumbar spine stability (intervertebral height, lumbar lordosis angle), decompression effect (cross-sectional area of the dural sac, intervertebral foramina area), functional prognosis, and complication status. Results In the VBE group, the amount of bleeding during the surgery was less than in the TLIF group, with shorter incision length, bed rest time, and hospital stay compared to the TLIF group (P < 0.05). VAS scores at 6 hours, 12 hours, 24 hours, 48 hours, and 72 hours post-operation were lower in the VBE group compared to the TLIF group (P < 0.05). VAS scores for lower back pain and leg pain at 3 and 6 months post-operation, as well as intervertebral height, lumbar lordosis angle, dural sac cross-sectional area, and intervertebral foramen area at 6 months post-operation were higher than pre-operation levels in both groups, but the inter-group differences were not statistically significant (P > 0.05). Comparison of the excellent-to-good functional prognosis rates between the two groups (98.04%, 94.12%) showed no statistically significant difference (P > 0.05). no complications occurred in the VBE group, while one case of incision exudation occurred in the TLIF group. Conclusion VBE and TLIF treatment for LDH with lumbar instability patients can enhance lumbar stability, improve patients' lumbar function, ensure safety, while VBE with a small incision can reduce intraoperative bleeding, decrease early postoperative pain, and speed up early recovery. -

图 1 VBE手术前后影像图片
A:术前俯卧位X线正位片;B:腰椎横截面CT影像片;C:术后俯卧位X线正位片。
Figure 1. Images before and after VBE surgery
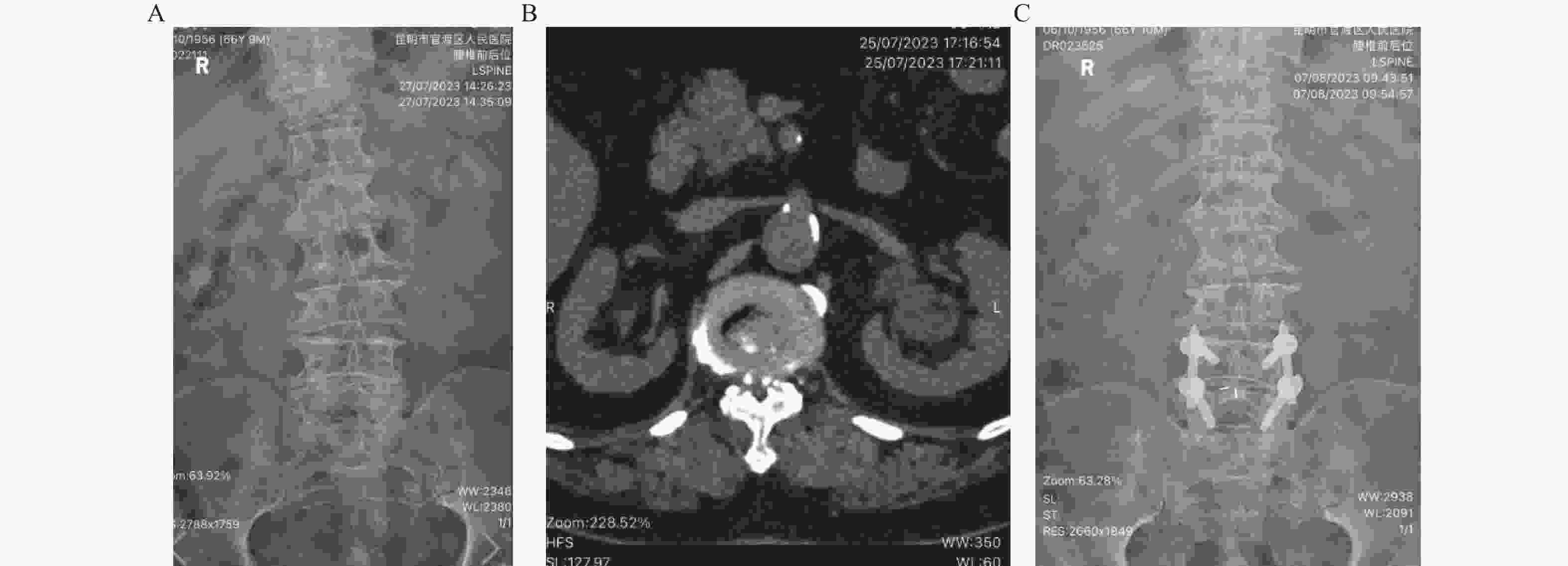
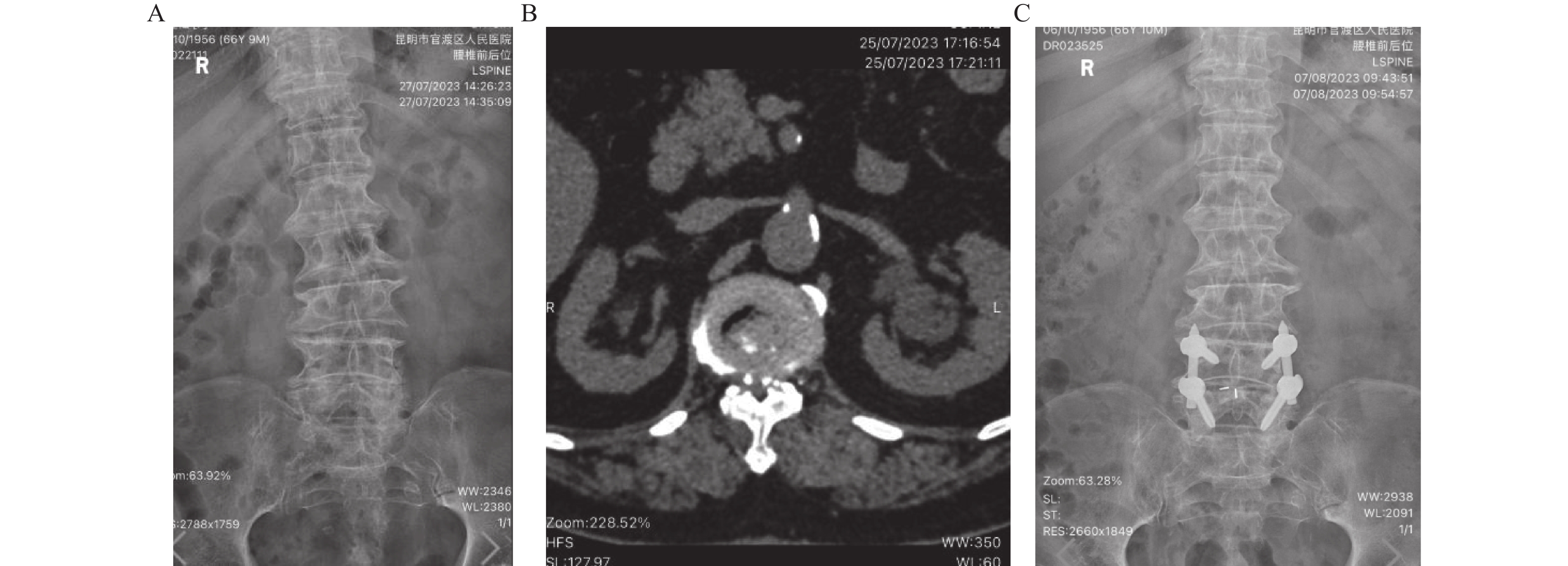
图 2 TLIF手术前后影像图片
A:术前俯卧位X线正位片;B:腰椎横截面CT影像片;C:术后俯卧位X线正位片。
Figure 2. Images of TLIF before and after surgery
表 1 2组基线资料比较[($\bar x \pm s $)/n(%)]
Table 1. Comparison of baseline information between the two groups [($\bar x \pm s $)/n (%)]
基线资料 VBE组(n=51) TLIF组(n=51) χ2/t P 年龄(岁) 65.14±3.42 64.97±3.48 0.359b 0.720 性别 0.630a 0.428 男 29(56.86) 25(49.02) 女 22(43.14) 26(50.98) BMI(kg/m2) 22.98±1.61 23.22±1.58 1.099b 0.273 病程(a) 3.79±1.28 3.92±1.31 0.731b 0.465 病变椎体 0.531 0.767 L3/4 10(19.61) 8(15.69) L4/5 27(52.94) 26(50.98) L5/S1 14(27.45) 17(33.33) 病变类型 0.371a 0.831 侧型 23(45.10) 20(39.22) 中央型 15(29.41) 17(33.33) 中央旁型 13(25.49) 14(27.45) 髓核突出程度 1.131a 0.568 隆起型 25(49.02) 22(43.14) 破裂型 14(27.45) 19(37.25) 游离型 12(27.45) 10(19.61) 合并症 高血压 21(41.18) 18(35.29) 0.374a 0.541 糖尿病 5(9.80) 8(15.69) 0.793a 0.373 高脂血症 7(13.73) 9(17.65) 0.297a 0.586 a表示χ2检验;b表示t检验。  下载: 导出CSV
下载: 导出CSV
表 2 2组手术一般情况比较[$ \bar x \pm s $/M(P25,P75)]
Table 2. Comparison of general surgical conditions in the two groups [($\bar x \pm s $)/M(P25,P75)]
组别 n 切口长度(cm) 手术时间(min) 术中出血量(mL) X线透视次数(次) 卧床时间(d) 住院时间(d) VBE组 51 1.01±0.23 101.67±14.39 41.70±13.52 6(3,9) 2.24±0.57 7.00±2.12 TLIF组 51 2.45±0.76 99.50±12.44 80.44±21.68 7(4,10) 4.00±0.81 10.52±3.11 t/Mann-Whitney U 17.830 1.187 15.241 0.954 17.968 9.441 P <0.001* 0.236 <0.001* 0.231 <0.001* <0.001* *P < 0.05。
下载: 导出CSV
表 3 2组围手术期VAS评分比较($\bar x \pm s $,分)
Table 3. Comparison of perioperative VAS scores in the two groups ($\bar x \pm s $,scores)
组别 n 术前 术后6 h 术后12 h 术后24 h 术后48 h 术后72 h VBE组 51 7.02±2.29 2.25±0.70 1.77±0.46 1.21±0.33 0.81±0.25 0.64±0.23 TLIF组 51 6.95±2.30 3.40±0.68 2.89±0.55 2.40±0.59 1.56±0.40 1.19±0.32 t 0.222 12.179 15.945 17.609 15.984 14.128 P 0.824 <0.001* <0.001* <0.001* <0.001* <0.001* *P < 0.05。
下载: 导出CSV
表 4 2组腰痛与下肢痛VAS评分比较($\bar x \pm s $,分)
Table 4. Comparison of VAS scores for low back pain and lower extremity pain in the two groups ($\bar x \pm s $,scores)
指标 组别 n 术前 术后3个月 术后6个月 腰痛VAS评分(分) VBE组 51 7.02±2.29 1.18±0.39 0.55±0.17 TLIF组 51 6.95±2.30 1.26±0.35 0.59±0.18 t 0.154 −1.090 −1.154 P 0.878 0.278 0.251 下肢痛VAS评分(分) VBE组 51 6.12±2.00 1.44±0.32 1.09±0.25 TLIF组 51 5.90±1.87 1.51±0.30 1.14±0.21 t 0.574 −1.140 −1.094 P 0.567 0.257 0.277
下载: 导出CSV
表 5 2组腰椎稳定性比较($\bar x \pm s $)
Table 5. Comparison of lumbar spine stability between the two groups ($\bar x \pm s $)
组别 n 椎间隙高度(mm) t P 腰椎前凸角(°) t P 术前 术后6个月 术前 术后6个月 VBE组 51 6.52±1.36 11.52±1.44 25.953 <0.001* 45.83±9.11 55.10±8.64 7.642 <0.001* TLIF组 51 6.60±1.28 11.40±1.59 23.952 <0.001* 46.78±7.52 54.28±10.01 6.078 <0.001* t 0.444 0.574 0.839 0.634 P 0.658 0.568 0.402 0.527 *P < 0.05。
下载: 导出CSV
表 6 2组减压效果比较[($\bar x \pm s $),mm2]
Table 6. Comparison of the effect of decompression in the two groups [($\bar x \pm s $),mm2]
组别 n 椎间孔面积 t P 硬膜囊横断面积 t P 术前 术后6个月 术前 术后6个月 VBE组 51 136.58±22.73 160.33±29.84 6.429 <0.001* 79.13±24.56 113.67±19.53 11.515 <0.001* TLIF组 51 138.00±24.15 158.95±26.00 6.064 <0.001* 81.27±27.40 111.06±22.77 8.724 <0.001* t 0.440 0.363 0.596 0.889 P 0.660 0.717 0.552 0.374 *P < 0.05。
下载: 导出CSV
表 7 2组功能预后比较[n(%)]
Table 7. Comparison of functional prognosis between the two groups [n (%)]
组别 n 优 良 一般 差 优良率 VBE组 51 39(76.47) 11(21.57) 1(1.96) 0(0.00) 50(98.04) TLIF组 51 32(62.75) 16(31.37) 3(5.88) 0(0.00) 48(94.12) χ2 0.260 P 0.610
下载: 导出CSV
-
[1] Siccoli A,Staartjes V E,De Wispelaere M P,et al. Tandem disc herniation of the lumbar and cervical spine: Case series and review of the epidemiological,pathophysiological and genetic literature[J]. Cureus,2019,11(2):e4081. [2] Shiga Y. The essence of clinical practice guidelines for lumbar disc herniation,2021: 1. Epidemiology and natural course[J]. Spine Surg Relat Res,2022,6(4):319-321. doi: 10.22603/ssrr.2022-0042 [3] 林少豪,何嘉辉,方志超,等. 腰椎内镜单纯减压治疗腰椎间盘突出症合并腰椎不稳的疗效分析[J]. 中国中医骨伤科杂志,2023,31(5):76-80. [4] Anderson A B,Braswell M J,Pisano A J,et al. Factors associated with progression to surgical intervention for lumbar disc herniation in the military health system[J]. Spine (Phila Pa 1976),2021,46(6): E392-E397. [5] Hornung A L,Barajas J N,Rudisill S S,et al. Prediction of lumbar disc herniation resorption in symptomatic patients: A prospective,multi-imaging and clinical phenotype study[J]. Spine J,2023,23(2):247-260. doi: 10.1016/j.spinee.2022.10.003 [6] Gupta A,Chhabra H S,Nagarjuna D,et al. Comparison of functional outcomes between lumbar interbody fusion surgery and discectomy in massive lumbar disc herniation: A retrospective analysis[J]. Global Spine J,2021,11(5):690-696. doi: 10.1177/2192568220921829 [7] Heemskerk J L,Oluwadara Akinduro O,Clifton W,et al. Long-term clinical outcome of minimally invasive versus open single-level transforaminal lumbar interbody fusion for degenerative lumbar diseases: A meta-analysis[J]. Spine J,2021,21(12):2049-2065. doi: 10.1016/j.spinee.2021.07.006 [8] Gong H Y,Fan Y S,Zhao Y C,et al. Minimally invasive transforaminal lumbar interbody fusion by a novel two-medium compatible bichannel endoscopy system,technique note and preliminary clinical results[J]. Eur Spine J,2023,32(8):2845-2852. doi: 10.1007/s00586-023-07746-w [9] Dal-Ré R. Waivers of informed consent in research with competent participants and the Declaration of Helsinki[J]. Eur J Clin Pharmacol,2023,79(4):575-578. doi: 10.1007/s00228-023-03472-w [10] 中华医学会骨科学分会脊柱外科学组,中华医学会骨科学分会骨科康复学组. 腰椎间盘突出症诊疗指南[J]. 中华骨科杂志,2020,40(8):477-487. [11] 中华中医药学会脊柱微创专家委员会,中国康复医学会骨伤康复专业委员会,中国医师协会骨科医师定期考核专业委员会脊柱外科专家组,等. 单孔分体内镜技术治疗腰椎管狭窄症专家共识[J]. 实用骨科杂志,2024,30(3):193-198. [12] Shafshak T S,Elnemr R. The visual analogue scale versus numerical rating scale in measuring pain severity and predicting disability in low back pain[J]. J Clin Rheumatol,2021,27(7):282-285. doi: 10.1097/RHU.0000000000001320 [13] Haro H,Ebata S,Inoue G,et al. Japanese Orthopaedic Association (JOA) clinical practice guidelines on the management of lumbar disc herniation,third edition - secondary publication[J]. J Orthop Sci,2022,27(1):31-78. doi: 10.1016/j.jos.2021.07.028 [14] Deng C,Feng H Y,Ma X,et al. Comparing oblique lumbar interbody fusion with lateral screw fixation and percutaneous endoscopic transforaminal discectomy (OLIF-PETD) and minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) for the treatment of lumbar disc herniation complicated with lumbar instability[J]. BMC Musculoskelet Disord,2022,23(1):1104. doi: 10.1186/s12891-022-06075-1 [15] 中国康复医学会脊柱脊髓专业委员会基础研究与转化学组. 腰椎间盘突出症诊治与康复管理指南[J]. 中华外科杂志,2022,60(5):401-408. [16] Kandregula S,Guthikonda B. Minimally invasive TLIF[J]. Neurol India,2021,69(5):1141. [17] Mikula A L,Lakomkin N,Elder B D,et al. Transforaminal lumbar interbody fusion with double cages: 2-dimensional operative video[J]. Oper Neurosurg (Hagerstown),2022,22(1):e52. doi: 10.1227/ONS.0000000000000025 [18] Lightsey H M 4th,Pisano A J,Striano B M,et al. ALIF versus TLIF for L5-S1 isthmic spondylolisthesis: ALIF demonstrates superior segmental and regional radiographic outcomes and clinical improvements across more patient-reported outcome measures domains[J]. Spine (Phila Pa 1976),2022,47(11): 808-816. [19] 贺石生. V形双通道脊柱内镜技术[M]. 北京: 科学出版社,2021: 17-22. [20] Verret M,Lauzier F,Zarychanski R,et al. Perioperative use of gabapentinoids for the management of postoperative acute pain: A systematic review and meta-analysis[J]. Anesthesiology,2020,133(2):265-279. doi: 10.1097/ALN.0000000000003428 [21] St-Georges M,Teles A R,Rabau O,et al. Adolescent idiopathic scoliosis: Evaluating perioperative back pain through a simultaneous morphological and biomechanical approach[J]. BMC Musculoskelet Disord,2020,21(1):466. doi: 10.1186/s12891-020-03462-4 [22] 陈帅,李志伟. 腰椎融合术围手术期疼痛管理的研究进展[J]. 现代临床医学,2023,49(1):64-67,71. [23] 孙凤龙,梁庆晨,王宏庆,等. 脊柱内镜下经椎间孔腰椎椎间融合术治疗腰椎间盘突出症伴腰椎不稳的早期临床研究[J]. 中华骨与关节外科杂志,2019,12(10):754-760. [24] Udby P M,Andersen M Ø,Ohrt-Nissen S. Improvement in physical function and reduced pain after instrumented lumbar interbody fusion[J]. Dan Med J,2023,70(9):A08220508. [25] Liu G,Liu W X,Jin D J,et al. Clinical outcomes of unilateral biportal endoscopic lumbar interbody fusion (ULIF) compared with conventional posterior lumbar interbody fusion (PLIF)[J]. Spine J,2023,23(2):271-280. doi: 10.1016/j.spinee.2022.10.001 [26] 李振宙,侯树勋. 经单侧椎板间隙入路双通道全内镜辅助下腰椎椎体间融合术[J]. 中国骨与关节杂志,2020,9(1):22-26. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 270
- HTML全文浏览量: 540
- PDF下载量: 8
- 被引次数: 0
