

Clinical Value of AI-Assisted Transvaginal Color Ultrasound Combined with Serum Markers in Diagnosing Heterotopic Pregnancy after IVF-ET
-
摘要:
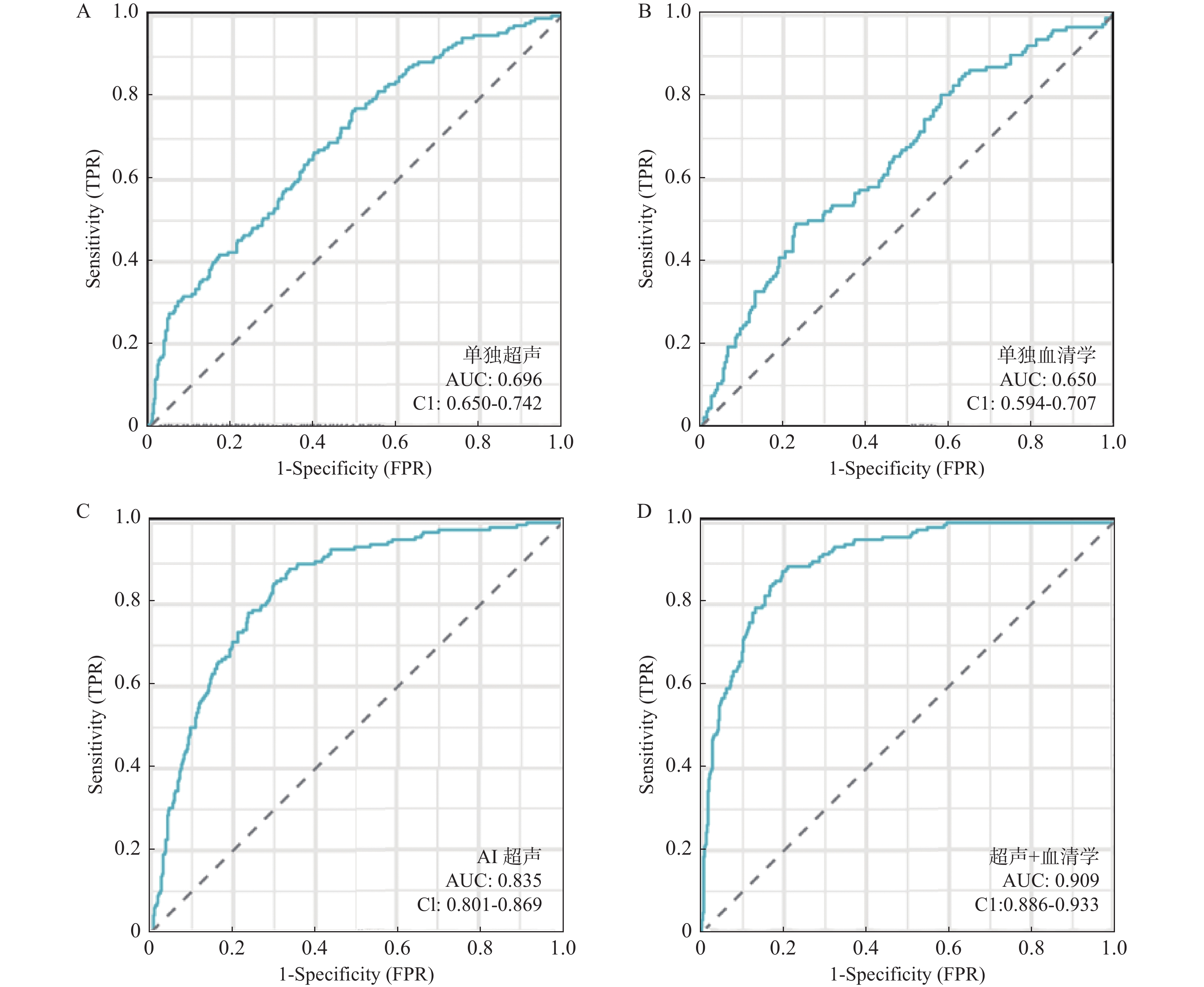
目的 探讨AI辅助阴道彩超联合血清标志物对IVF-ET后宫内外复合妊娠(HP)的早期诊断价值。 方法 本研究为回顾性病例对照研究,纳入2022年1月至2024年12月期间在河北省沧州中西医结合医院接受IVF-ET治疗后确诊为HP的86例患者。对照组包括同期86例正常宫内妊娠和86例单纯异位妊娠患者。所有患者均通过临床诊断、影像学检查及手术确认诊断。采用AI超声影像分析模型和血清学指标(hCG、PAPP~A、APA、孕酮、PlGF)联合评估HP的诊断效能。通过计算灵敏度、特异度、阳性预测值和阴性预测值,比较各组的诊断性能。 结果 AI超声影像分析模型的AUC值为0.835,显著优于传统超声(AUC=0.696,P < 0.01)。血清hCG和PAPP~A分别为( 36210 ±9820 ) IU/L和(0.81±0.25)μg/mL。联合诊断的AUC值为0.909,敏感性为94.2%,特异性为88.4%,阳性预测值为91.6%,阴性预测值为92.8%。结论 AI辅助超声联合血清学指标显著提高HP早期诊断准确性,优于单一方法,为临床提供了可靠工具。 Abstract:Objective To investigate the early diagnostic value of AI-assisted transvaginal ultrasound combined with serum biomarkers for intrauterine and ectopic combined pregnancy (heterotopic pregnancy, HP) after IVF-ET. Methods This retrospective case-control study included 86 patients diagnosed with HP after IVF-ET at Cangzhou Hospital of Integrated Traditional Chinese and Western Medicine between January 2022 and December 2024. Control groups consisted of 86 patients with normal intrauterine pregnancies and 86 patients with simple ectopic pregnancy. All patients were diagnosed through clinical diagnosis, imaging examinations, and surgical confirmation. An AI ultrasound image analysis model and serum markers (hCG, PAPP-A, APA, progesterone, PlGF) were used to jointly assess HP diagnostic efficiency. Diagnostic performance was compared by calculating sensitivity, specificity, positive predictive value, and negative predictive value. Results The AI ultrasound image analysis model's AUC was 0.835, significantly superior to traditional ultrasound (AUC=0.696). Serum hCG and PAPP-A levels were (36, 210±9, 820) IU/L and (0.81±0.25) μg/mL, respectively. The joint diagnostic AUC was 0.909, with a sensitivity of 94.2%, specificity of 88.4%, positive predictive value of 91.6%, and negative predictive value of 92.8%. Conclusion AI-assisted ultrasound combined with serological markers significantly improves the early diagnostic accuracy of HP, outperforming single methods and providing a reliable clinical tool. -
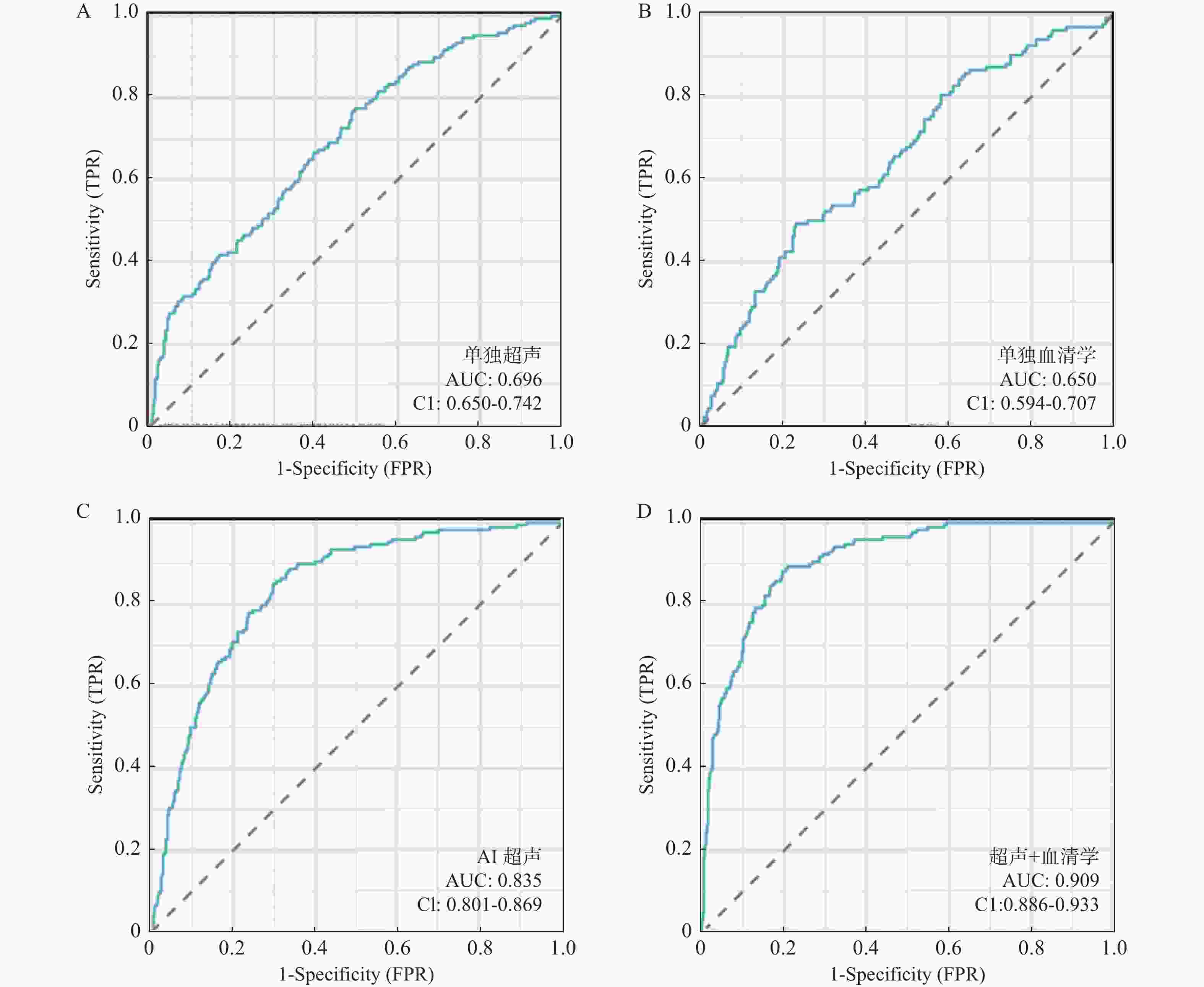
图 2 ROC曲线分析
A:单独超声的ROC曲线;B:单独血清学指标的ROC曲线;C:AI超声的ROC曲线;D:联合诊断的ROC曲线。
Figure 2. ROC curve analysis
表 1 患者基本特征[($\bar x \pm s $)/n (%)]
Table 1. Basic characteristics of patients[($\bar x \pm s $)/n (%)]
指标 HP组
(n=86)正常宫内
妊娠组(n=86)单纯异位
妊娠组(n=86)F/χ2 P 平均年龄(岁) 33.2 ± 4.1 32.8 ± 3.9 32.5 ± 4.0 0.75 0.474 平均孕周(周) 6.8 ± 1.2 6.9 ± 1.1 7.0 ± 1.0 0.5 0.607 阴道出血 71 (82.6) 13 (15.1) 53 (61.6) 95.2 <0.001* 下腹痛 56 (65.1) 16 (18.6) 63 (73.3) 65.8 <0.001* *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 阴道彩色多普勒超声检查特征[($\bar x \pm s $)/n (%)]
Table 2. Features of transvaginal color doppler ultrasound examination[($\bar x \pm s $)/n (%)]
超声特征 数值结果 标准差 (SD) 95%置信区间 (CI) 宫内妊娠孕囊平均直径 (mm) 18.6 ± 4.2 4.2 17.2 ~ 19.9 胎心搏动检出率(%) 76(88.4) - - 输卵管妊娠发生率(%) 64(74.4) - - 异位妊娠平均包块直径 (mm) 24.3 ± 6.1 6.1 22.2 ~ 26.4 “火环征”阳性率(%) 55(64.0) - - 高流量血流信号出现率(%) 50(58.1) - - 输卵管妊娠包块位于输卵管中段 44(52.3) - - 异位妊娠出现血管影像征 36(41.8) - -
下载: 导出CSV
表 3 人工智能影像分析模型评估指标
Table 3. Evaluation metrics of artificial intelligence imaging analysis model
评估指标 评估指标数值 95% 置信区间 (CI) 准确率 (%) 92.4 90.1 ~94.7 敏感性(%) 94.2 92.5 ~ 95.9 特异性 (%) 88.4 85.6 ~ 91.2 F1-score 93.2 91.5 ~ 94.9 AUC 0.835 0.801 ~ 0.869
下载: 导出CSV
表 4 血清hCG与PAPP-A检测结果[($\bar x \pm s $)/n (%)]
Table 4. Serum hCG and PAPP-A test results[($\bar x \pm s $)/n (%)]
指标 测量值 95% 置信区间 (CI) P 血清hCG (IU/L) 36210 ± 9820 28000 ~45000 0.001** 血清PAPP-A(μg/mL) 0.81 ± 0.25 0.68 ~ 0.94 0.003** 血清APA阳性率 (%) 45(52.3) 41.5 ~ 63.1 0.021* 血清孕酮 (ng/mL) 12.5 ± 4.2 10.1 ~ 14.9 0.008** 血清 PlGF (pg/mL) 22.6 ± 8.1 18.4 ~ 26.8 0.004** *P < 0.05;**P < 0.01。
下载: 导出CSV
表 5 不同诊断方法的敏感性与特异性
Table 5. Sensitivity and specificity of different diagnostic methods
诊断方法 敏感性 (%) 特异性 (%) 阳性预测值 (%) 阴性预测值 (%) 传统超声单独诊断 81.4 73.2 79.4 74.2 AI超声单独诊断 84.5 76.7 84.3 80.1 血清学指标联合诊断 78.2 72.1 81.5 75.9 联合诊断(超声 + 血清学指标) 94.2 88.4 91.6 92.8
下载: 导出CSV
-
[1] Han Q S, Zhou Y, Xu Y, et al. Optimal timing of GnRH antagonist initiation in IVF-ET: A retrospective cohort study on advanced maternal age women[J]. Front Endocrinol (Lausanne), 2024, 15: 1340230. doi: 10.3389/fendo.2024.1340230 [2] Wang R, Pan W, Yu L, et al. AI-based optimal treatment strategy selection for female infertility for first and subsequent IVF-ET cycles[J]. J Med Syst, 2023, 47(1): 87. doi: 10.1007/s10916-023-01967-8 [3] Zhu S, Fan Y, Lan L, et al. Heterotopic pregnancy secondary to in vitro fertilization-embryo transfer: Risk factors and pregnancy outcomes[J]. Front Med (Lausanne), 2022, 9: 864560. doi: 10.3389/fmed.2022.864560 [4] Mao Y, Peng Y, Zheng M, et al. First-trimester ultrasound diagnosis and risk factor analysis of cesarean scar pregnancy after in vitro fertilization-embryo transfer[J]. Quant Imaging Med Surg, 2024, 14(7): 5028-5039. doi: 10.21037/qims-23-1239 [5] Li X, Cai P, Ouyang Y, et al. Heterotopic interstitial pregnancy: Early ultrasound diagnosis of 179 cases after in vitro fertilization-embryo transfer[J]. J Ultrasound Med, 2023, 42(4): 915-922. doi: 10.1002/jum.16103 [6] 邵慧娟, 郑晓凤, 李琪, 等. 胚胎移植宫内外复合妊娠合并输卵管及黄体破裂休克1例并文献复习[J]. 生殖医学杂志, 2023, 32(4): 610-612. doi: 10.3969/j.issn.1004-3845.2023.04.021 [7] Chen X, Chen F, Zhu W, et al. Treatment effects of laparoscopy versus laparotomy on heterotopic pregnancy after in vitro fertilization and embryo transfer[J]. Int J Gynaecol Obstet, 2023, 163(2): 689-696. doi: 10.1002/ijgo.14919 [8] 尚琴琴, 刘何利. 经阴道彩色多普勒超声诊断IVF-ET术后宫内外复合妊娠效果及腹腔镜手术后妊娠结局[J]. 中国计划生育学杂志, 2024, 32(5): 1117-1120. doi: 10.3969/j.issn.1004-8189.2024.05.027 [9] Maleki A, Khalid N, Rajesh Patel C, et al. The rising incidence of heterotopic pregnancy: Current perspectives and associations with in-vitro fertilization[J]. Eur J Obstet Gynecol Reprod Biol, 2021, 266: 138-144. doi: 10.1016/j.ejogrb.2021.09.031 [10] Orsi M, Motta F, Fedele F, et al. Heterotopic cervical and isthmic pregnancy[J]. Ultrasound Obstet Gynecol, 2024, 63(6): 841-842. doi: 10.1002/uog.27603 [11] Heremans R, Valentin L, Sladkevicius P, et al. Imaging in gynecological disease (24): Clinical and ultrasound characteristics of ovarian mature cystic teratomas[J]. Ultrasound Obstet Gynecol, 2022, 60(4): 549-558. doi: 10.1002/uog.24904 [12] Bartusevicius A, Bartuseviciene E, Maseviciene M, et al. Heterotopic tubal choriocarcinoma coexistent with a viable intrauterine pregnancy: A case report[J]. Medicina (Kaunas), 2024, 60(8): 1226. [13] Conover C A, Oxvig C. The pregnancy-associated plasma protein-A (PAPP-A) story[J]. Endocr Rev, 2023, 44(6): 1012-1028. doi: 10.1210/endrev/bnad017 [14] Pasinska M, Balcerek E, Repczynska A, et al. The levels of pregnancy-associated plasma protein (PAPP-A) and chorionic gonadotropin (β-hCG) in the blood serum of women with hypothyroidism in the 1st trimester of pregnancy[J]. Int J Womens Health, 2023, 15: 167-176. doi: 10.2147/IJWH.S386414 [15] van Dijk C E, van Gils A L, van Zijl M D, et al. Cervical pessary versus vaginal progesterone in women with a singleton pregnancy, a short cervix, and no history of spontaneous preterm birth at less than 34 weeks' gestation: Open label, multicentre, randomised, controlled trial[J]. BMJ, 2024, 384: e077033. [16] Gladstone R A, Ahmed S, Huszti E, et al. Midpregnancy placental growth factor screening and early preterm birth[J]. JAMA Netw Open, 2024, 7(11): e2444454. doi: 10.1001/jamanetworkopen.2024.44454 [17] Branch D W, Lim M Y. How I diagnose and treat antiphospholipid syndrome in pregnancy[J]. Blood, 2024, 143(9): 757-768. doi: 10.1182/blood.2023020727 [18] Zhang Y Z, Zhou L, Tian L. A mid-pregnancy risk prediction model for gestational diabetes mellitus based on the maternal status in combination with ultrasound and serological findings[J]. Exp Ther Med, 2020, 20(1): 293-300. doi: 10.3892/etm.2020.8690 [19] 张芸, 丁霞, 李刚, 等. 人工智能技术评估早孕期胎盘体积应用价值分析[J]. 中国初级卫生保健, 2024, 38(3): 56-59. doi: 10.3969/j.issn.1001-568X.2024.03.0015 [20] 陈菲, 李茂林, 蒋玉婷, 等. 深度卷积网络模型可自动识别与分割胰腺及其肿瘤: 基于3D V-Net[J]. 分子影像学杂志, 2024, 47(11): 1170-1175. [21] Huang Y, Yao Z, Li L, et al. Deep learning radiopathomics based on preoperative US images and biopsy whole slide images can distinguish between luminal and non-luminal tumors in early-stage breast cancers[J]. EBiomedicine, 2023, 94: 104706. doi: 10.1016/j.ebiom.2023.104706 [22] Elsayed S, Farah N, Anglim M. Heterotopic pregnancy: Case series and review of diagnosis and management[J]. Case Rep Obstet Gynecol, 2023, 2023: 2124191. [23] 温召迎. 经腹部超声联合经阴道超声在宫外孕诊断中的应用价值[J]. 临床医学研究与实践, 2022, 7(32): 110-113. [24] Vaidakis D, Papapanou M, Siristatidis C S. Autologous platelet-rich plasma for assisted reproduction[J]. Cochrane Database Syst Rev, 2024, 4(4): CD013875. [25] Craciunas L, Tsampras N, Raine-Fenning N, et al. Intrauterine administration of human chorionic gonadotropin (hCG) for subfertile women undergoing assisted reproduction[J]. Cochrane Database Syst Rev, 2018, 10(10): CD011537. [26] Houser M, Kandalaft N, Khati N J. Ectopic pregnancy: A resident's guide to imaging findings and diagnostic pitfalls[J]. Emerg Radiol, 2022, 29(1): 161-172. doi: 10.1007/s10140-021-01974-7 [27] 宋淑花. 经阴道彩色多普勒超声在宫外孕破裂与卵巢黄体破裂鉴别诊断中的临床价值[J]. 基层医学论坛, 2024, 28(33): 76-79. [28] Harzif A K, Hyaswicaksono P, Kurniawan R H, et al. Heterotopic pregnancy: Diagnosis and pitfall in ultrasonography[J]. Gynecol Minim Invasive Ther, 2021, 10(1): 53-56. doi: 10.4103/GMIT.GMIT_92_19 [29] Zhou H, Chen W, Chen C, et al. Predictive value of ultrasonic artificial intelligence in placental characteristics of early pregnancy for gestational diabetes mellitus[J]. Front Endocrinol (Lausanne), 2024, 15: 1344666. doi: 10.3389/fendo.2024.1344666 [30] Li W B, Du Z C, Liu Y J, et al. Prediction of axillary lymph node metastasis in early breast cancer patients with ultrasonic videos based deep learning[J]. Front Oncol, 2023, 13: 1219838. doi: 10.3389/fonc.2023.1219838 -

 点击查看大图
点击查看大图

计量
- 文章访问数: 122
- HTML全文浏览量: 92
- PDF下载量: 7
- 被引次数: 0
