

Predictive Value of INETs combined with Neutrophil Indicators for Thromboembolic Complications in Patients under ECMO Assistance
-
摘要:
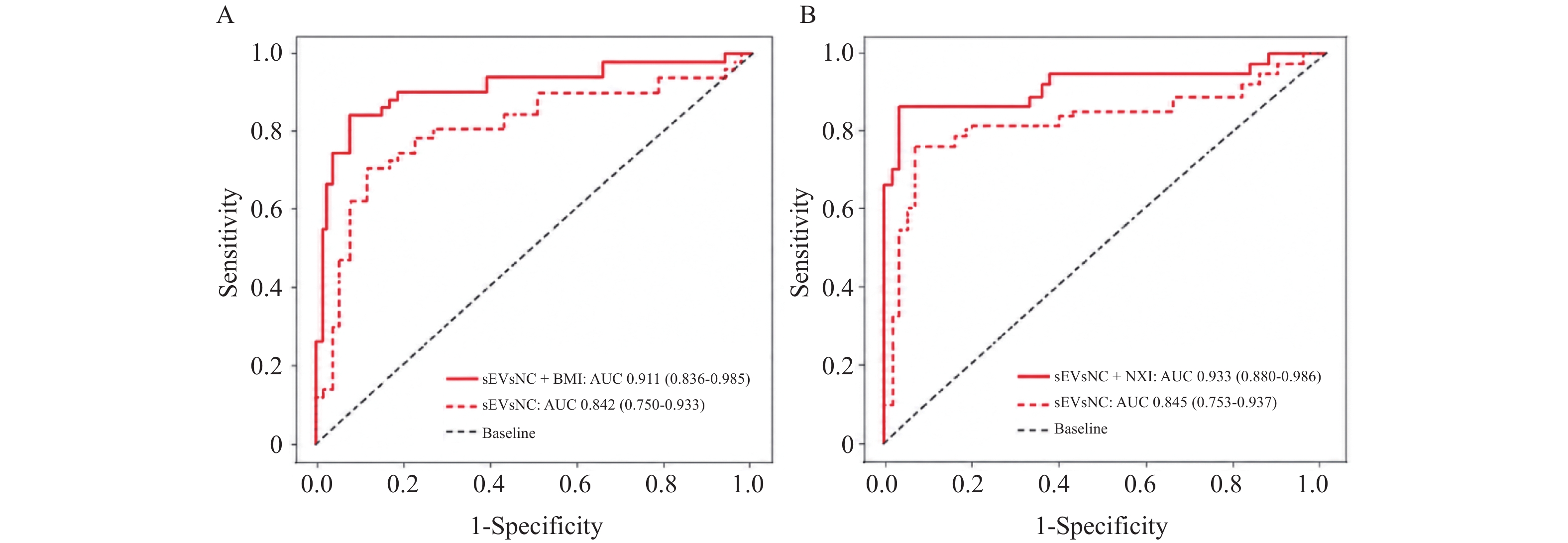
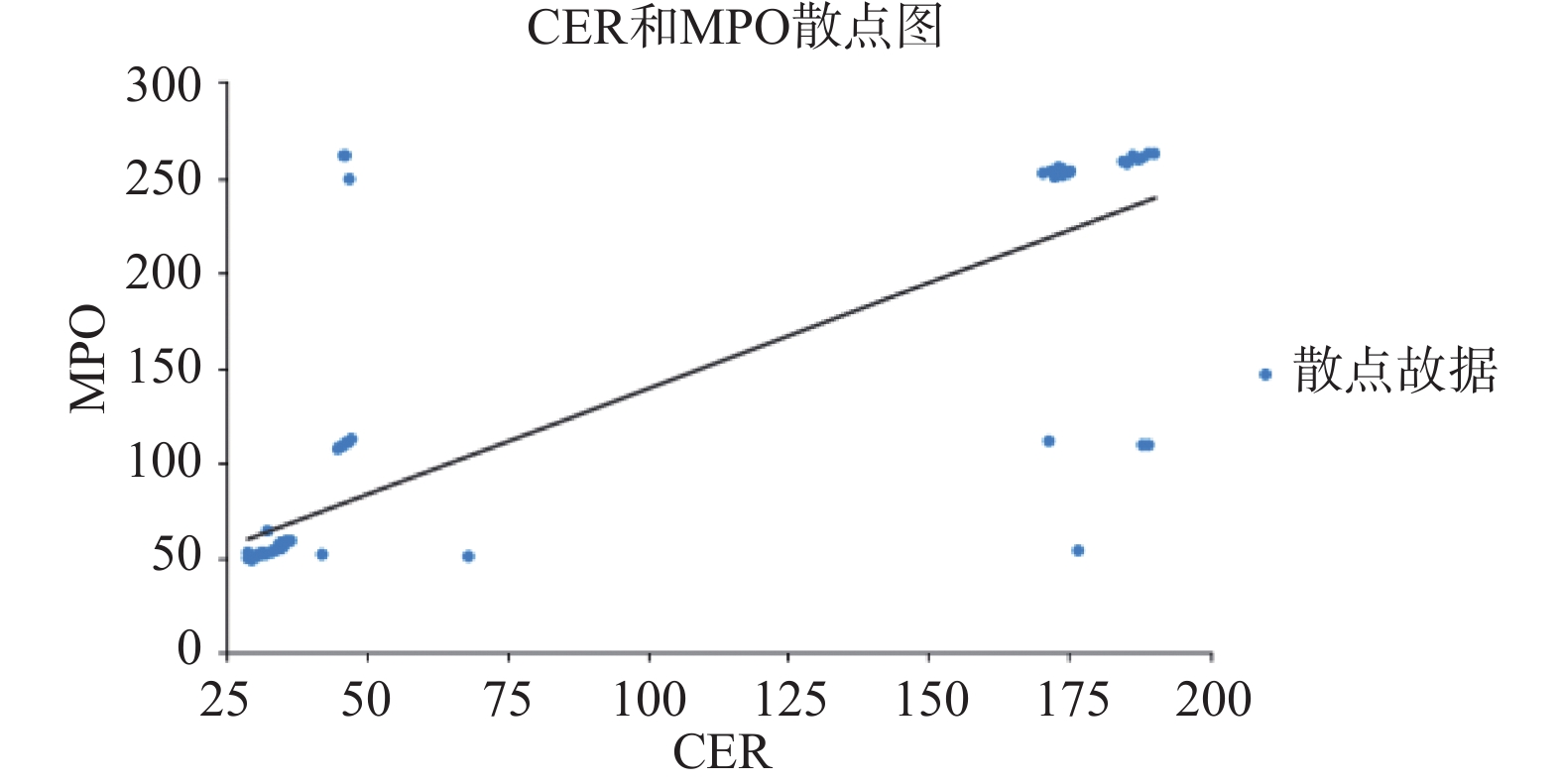
目的 探讨中性粒细胞胞外诱捕网(neutrophil extracellular traps,NETs)相关指标联合中性粒细胞功能指标对体外膜肺氧合(extracorporeal membrane oxygenation,ECMO)辅助患者血栓并发症的预警价值。 方法 本研究为单中心前瞻性队列研究,连续纳入 2023 年 1 月至 2024 年 12 月在内蒙古自治区人民医院接受 ECMO 辅助治疗的患者 100 例。根据有无血栓并发症分为非血栓并发症组和血栓并发症组。根据MACE发生的人数,将总研究人数分为MACE组和非MACE组。收集患者一般资料、病史及 ECMO 相关参数。检测血常规、凝血功能、NETs 标志物[髓过氧化物酶-DNA复合物(myeloperoxidase-DNA complexes,MPO-DNA)、瓜氨酸化组蛋白H3(citrullinated histone H3,CitH3)]及中性粒细胞功能指标[表面标志物〔分化簇11b(cluster of differentiation 11b,CD11b)、L-选择素(L-selectin,CD62L)〕及活性氧(reactive oxygen species,ROS)生成]。通过影像学检查及临床评估判定血栓并发症发生情况。采用 t 检验、卡方检验、相关性分析及受试者工作特征(receiver operating characteristic,ROC)曲线分析评价各指标的预测价值。 结果 100 例患者中,30 例(30.0%)发生血栓并发症。与非血栓组相比,血栓组 MPO 水平显著升高(P < 0.05)。随访期间共 23 例发生主要不良心血管事件(major adverse cardiovascular events,MACE),MACE 组 MPO 及血清铜蓝蛋白(ceruloplasmin,CER)水平均显著高于非 MACE 组(P < 0.05)。CER 与 MPO 水平具有相关性(r = 0.333,P < 0.001)。ROC 分析显示,MPO 预测 MACE 的效能高于 CER(AUC:0.867 vs 0.856,P < 0.05),而 CER 预测血栓并发症的效能高于 MPO(AUC:0.865 vs 0.825,P < 0.05)。 结论 NETs 相关指标联合中性粒细胞功能指标在 ECMO 辅助患者血栓并发症的预测中具有较好的预警价值,可为临床风险评估提供依据。 Abstract:Objective To evaluate the predictive value of neutrophil extracellular traps (NETs)–related indicators combined with neutrophil functional indices for thrombotic complications in patients receiving extracorporeal membrane oxygenation (ECMO) support. Methods The single-center prospective cohort study consecutively enrolled 100 patients receiving ECMO-assisted therapy at the Inner Mongolia Autonomous Region People's Hospital from January 2023 to December 2024. Patients were divided into non-thrombotic complication group and thrombotic complication group based on the presence or absence of thrombotic complications. The total study population was further divided into MACE group and non-MACE group according to the occurrence of MACE events. General patient data, medical history, and ECMO-related parameters were collected.Routine blood tests, coagulation function, NETs markers [myeloperoxidase-DNA complexes (MPO-DNA) and citrullinated histone H3 (CitH3)], and neutrophil functional indices [surface markers (CD11b, CD62L) and reactive oxygen species (ROS) production]were measured. Thrombotic complications were identified through imaging examinations and clinical evaluation. The predictive value of each indicator was assessed using t-test, chi-square test, correlation analysis, and receiver operating characteristic (ROC) curve analysis. Results Among the 100 patients, 30 (30.0%) developed thrombotic complications. MPO levels were significantly higher in the thrombosis group than in the non-thrombosis group (P < 0.05). During follow-up, 23 patients experienced MACE. Levels of MPO and ceruloplasmin (CER) were significantly higher in the MACE group (P < 0.05). CER levels were correlated with MPO levels (r = 0.333, P < 0.001). ROC analysis showed that MPO had better predictive performance for MACE than CER (AUC: 0.867 vs 0.856, P < 0.05), whereas CER demonstrated better performance in predicting thrombotic complications than MPO(AUC: 0.865 vs 0.825, P < 0.05). Conclusion NETs-related indicators combined with neutrophil functional indices have potential predictive value for thrombotic complications in ECMO-supported patients and may aid in clinical risk assessment. -
Key words:
- ECMO /
- Thromboembolic complications /
- Neutrophils /
- NETs
-
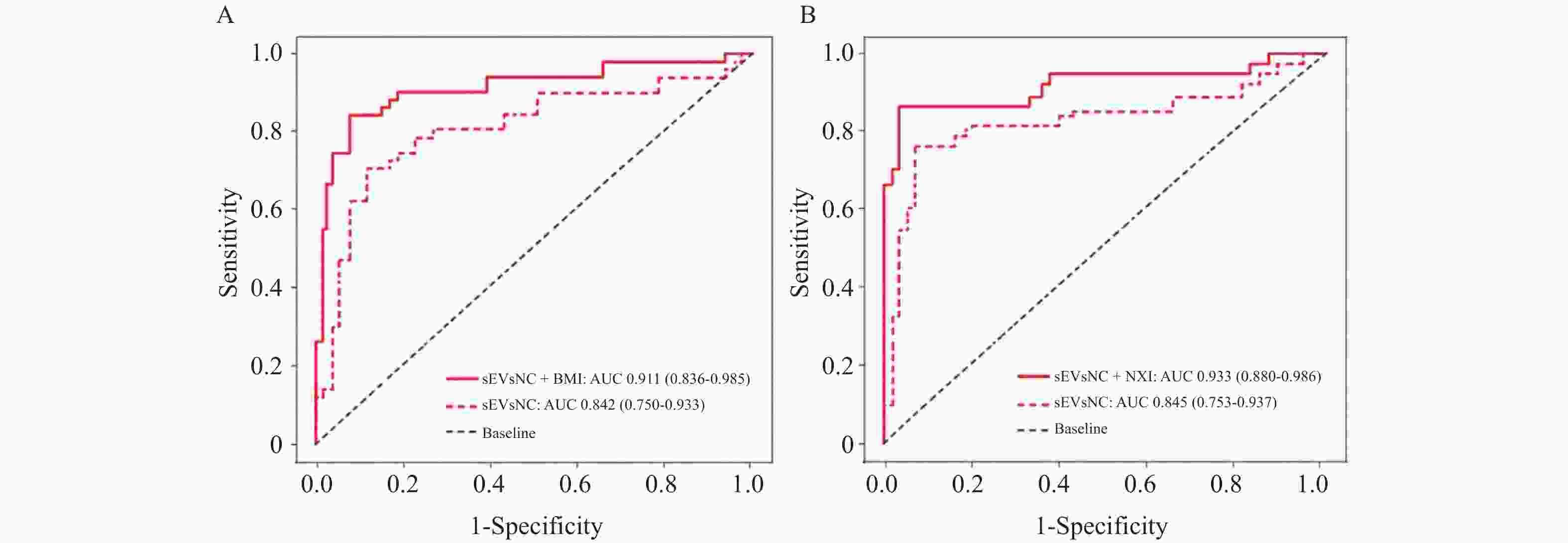
图 2 ROC曲线分析CER、MPO 水平预测接受 ECMO辅助治疗者血栓并发症及 MACE 事件
A:CER及MPO预测血栓并发症的ROC曲线;B:CER及MPO预测MACE事件的ROC曲线。
Figure 2. ROC curve analysis of CER and MPO levels in predicting thrombotic complications and MACE events in patients receiving ECMO-assisted therapy
表 1 ECMO 辅助治疗患者发生血栓并发症影响因素的单因素分析[$\bar x \pm s $/n(%)]
Table 1. Univariate analysis of influencing factors for thrombotic complications in patients receiving ECMO-assisted therapy[$\bar x \pm s $/ n(%)]
基线资料 非血栓并发症组(n = 70) 血栓并发症组(n = 30) t/χ2 P 年龄(岁) 55.32 ± 10.21 62.15 ± 11.33 4.235 0.001* BMI(kg/m2) 24.56 ± 3.21 25.87 ± 4.12 1.987 0.052 男性 56(70.0) 24(30.0) 0.000 1.000 收缩压(mmHg) 120.56 ± 15.32 125.67 ± 18.45 1.678 0.097 舒张压(mmHg) 75.23 ± 10.12 78.45 ± 11.23 1.732 0.086 高血压 42(67.7) 20(32.3) 0.571 0.450 吸烟 21(67.7) 10(32.3) 0.125 0.723 饮酒 12(70.6) 5(29.4) 0.003 0.955 TC(mmol/L) 4.89 ± 0.98 5.12 ± 1.05 1.324 0.188 HDL - c(mmol/L) 1.42 ± 0.35 1.36 ± 0.42 0.876 0.383 LDL - c(mmol/L) 2.78 ± 0.76 2.91 ± 0.82 1.057 0.293 TG(mmol/L) 1.55 ± 1.02 1.68 ± 1.15 0.674 0.502 血糖(mmol/L) 7.89 ± 2.01 8.23 ± 2.34 0.798 0.426 HbA1c(%) 6.54 ± 1.02 6.78 ± 1.13 1.125 0.263 eGFR[mL/(min·1.73m2)] 72.56 ± 16.33 68.78 ± 18.56 1.187 0.238 APTT(s) 52.34 ± 10.56 45.21 ± 9.87 3.126 0.002* INR 1.85 ± 0.42 1.61 ± 0.36 2.678 0.009* 肝素剂量[U/(kg·h)] 11.23 ± 2.34 9.87 ± 2.11 2.615 0.011* CitH3(ng/mL) 8.76 ± 2.31 15.42 ± 4.87 8.214 < 0.001* MPO-DNA(ng/mL) 42.35 ± 11.28 96.71 ± 28.56 11.032 < 0.001* MPO(U/L) 60.92 ± 17.97 194.58 ± 91.02 6.325 < 0.001* Nrf2(μg/L) 27.89 ± 6.32 30.12 ± 7.15 1.789 0.076 AGE(μg/L) 20.56 ± 6.23 22.33 ± 7.01 1.632 0.105 CAT(U/L) 33.21 ± 10.56 30.56 ± 11.23 1.345 0.182 GSH - Px(U/L) 140.56 ± 80.23 135.67 ± 75.33 0.456 0.649 SOD(U/L) 75.32 ± 19.87 70.56 ± 20.33 1.156 0.250 CER(μg/L) 38.61 ± 24.77 129.29 ± 68.32 8.765 < 0.001* CD11b阳性率(%) 78.56 ± 10.23 80.12 ± 11.45 0.654 0.515 CD62L阳性率(%) 65.34 ± 12.11 63.89 ± 13.02 0.543 0.588 *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 ECMO 辅助治疗患者发生 MACE 事件影响因素的单因素分析[$\bar x \pm s $/ n(%)]
Table 2. Univariate analysis of risk factors for MACE events in patients receiving ECMO support therapy[$\bar x \pm s $/ n(%)]
特征 非 MACE 组(n = 77) MACE 组(n = 23) t/χ2 P 年龄(岁) 56.12 ± 10.56 63.23 ± 12.45 2.345 0.021* BMI(kg/m2) 24.67 ± 3.12 25.33 ± 4.21 0.987 0.326 男性 68(80.0) 12(80.0) 0.000 1.000 收缩压(mmHg) 121.33 ± 15.21 124.56 ± 18.32 1.023 0.309 舒张压(mmHg) 75.67 ± 10.23 77.89 ± 11.34 1.234 0.220 高血压 50(64.9) 12(52.2) 2.897 0.089 吸烟 25(32.4) 6(26.1) 1.034 0.309 饮酒 14(18.2) 3(13.0) 0.235 0.628 DR 6.325 0.012* 非 DR 72(93.5) 8(34.8) 轻中度 NPDR 11(14.3) 4(17.4) 重度 NPDR/PDR 2(2.6) 3(13.0) TC(mmol/L) 4.92 ± 0.95 5.23 ± 1.06 1.532 0.129 HDL - c(mmol/L) 1.43 ± 0.36 1.35 ± 0.41 0.987 0.326 LDL - c(mmol/L) 2.79 ± 0.75 2.93 ± 0.81 1.057 0.293 TG(mmol/L) 1.56 ± 1.01 1.69 ± 1.14 0.674 0.502 血糖(mmol/L) 7.92 ± 2.03 8.33 ± 2.31 0.798 0.426 HbA1c(%) 6.56 ± 1.01 6.75 ± 1.12 1.125 0.263 eGFR[mL/(min·1.73m2)] 72.89 ± 16.23 69.33 ± 18.45 1.187 0.238 APTT(s) 51.89 ± 10.23 44.56 ± 9.45 3.245 0.002* INR 1.82 ± 0.41 1.58 ± 0.35 2.734 0.008* 肝素剂量[U/(kg·h)] 11.02 ± 2.28 9.56 ± 2.03 2.587 0.011* MPO(U/L) 71.15 ± 47.15 201.00 ± 88.67 5.325 < 0.001* Nrf2(μg/L) 27.98 ± 6.21 29.87 ± 7.02 1.345 0.182 AGE(μg/L) 20.67 ± 6.12 22.11 ± 6.89 1.324 0.188 CAT(U/L) 33.33 ± 10.67 30.22 ± 11.56 1.345 0.182 GSH - Px(U/L) 141.23 ± 80.33 130.56 ± 72.45 0.876 0.383 SOD(U/L) 75.67 ± 19.78 70.11 ± 20.23 1.324 0.188 CER(μg/L) 44.28 ± 36.39 137.90 ± 65.78 8.325 < 0.001* CitH3(ng/mL) 9.12 ± 2.56 16.35 ± 5.02 8.765 < 0.001* MPO-DNA(ng/mL) 45.78 ± 12.45 101.23 ± 30.67 10.214 < 0.001* *P < 0.05。
下载: 导出CSV
表 3 ECMO 辅助治疗患者发生 MACE 事件影响因素的多因素分析
Table 3. Multivariate analysis of influencing factors for MACE events in patients receiving ECMO-assisted therapy
变量 β SE Wald χ² OR 95%CI P 年龄(岁) 0.051 0.026 3.846 1.052 1.000–1.107 0.050 DR分级 1.153 0.501 5.294 3.168 1.186–8.462 0.021* MPO-DNA(ng/mL) 0.029 0.010 8.410 1.029 1.009–1.050 0.004* CER(μg/L) 0.011 0.004 7.563 1.011 1.003–1.020 0.006* APTT(s) −0.064 0.023 7.741 0.938 0.896–0.982 0.005* 肝素剂量[U/(kg·h)] −0.172 0.067 6.589 0.842 0.739–0.959 0.010* *P < 0.05。
下载: 导出CSV
-
[1] Nadkarni A S, Delany D R, Schramm J, et al. ECMO considerations in the pediatric cardiac population[J]. Curr Pediatr Rep, 2023, 11(3): 86-95. doi: 10.1007/s40124-023-00292-5 [2] Taccone F S, Nobile L, Annoni F. Thrombolysis for ECMO oxygenator thrombosis[J]. Crit Care, 2023, 27(1): 142. doi: 10.1186/s13054-023-04433-6 [3] Cohen W G, Rekhtman D, Iyengar A, et al. Extended support with the impella 5.5: Transplant, ECMO, and complications[J]. ASAIO J, 2023, 69(7): 642-648. doi: 10.1097/MAT.0000000000001931 [4] Thomas J, Kostousov V, Teruya J. Bleeding and thrombotic complications in the use of extracorporeal membrane oxygenation[J]. Semin Thromb Hemost, 2018, 44(1): 20-29. [5] Baran C, Ozcinar E, Kayan A, et al. Vascular complications in patients with ECMO support after cardiac surgery[J]. J Clin Med, 2024, 13(17): 5055. doi: 10.3390/jcm13175055 [6] Liu Y, Yan P, Bin Y, et al. Neutrophil extracellular traps and complications of liver transplantation[J]. Front Immunol, 2022, 13: 1054753. doi: 10.3389/fimmu.2022.1054753 [7] Pertiwi K, van der Wal A, Pabittei D, et al. Neutrophil extracellular traps participate in all different types of thrombotic and haemorrhagic complications of coronary atherosclerosis[J]. Thromb Haemost, 2018, 118(6): 1078-1087. doi: 10.1055/s-0038-1641749 [8] Li J, Xuan R, Wu W, et al. Geldanamycin ameliorates multiple organ dysfunction and microthrombosis in septic mice by inhibiting the formation of the neutrophil extracellular network by activating heat shock factor 1 HSF1[J]. Clin Exp Pharmacol Physiol, 2023, 50(8): 698-707. doi: 10.1111/1440-1681.13798 [9] Jabrah D, Rossi R, Molina S, et al. White blood cell subtypes and neutrophil extracellular traps content as biomarkers for stroke etiology in acute ischemic stroke clots retrieved by mechanical thrombectomy[J]. Thromb Res, 2024, 234: 1-8. doi: 10.1016/j.thromres.2023.12.005 [10] Ducroux C, Di Meglio L, Loyau S, et al. Thrombus neutrophil extracellular traps content impair tPA-induced thrombolysis in acute ischemic stroke[J]. Stroke, 2018, 49(3): 754-757. doi: 10.1161/STROKEAHA.117.019896 [11] Chen J, Liu T, He J, et al. Correspondence on ‘Critical role of neutrophil extracellular traps (NETs) in patients with Behcet’s disease‘[J]. Ann Rheum Dis, 2023, 82(2): e48. doi: 10.1136/annrheumdis-2020-219472 [12] Demkow U. Molecular mechanisms of neutrophil extracellular trap (NETs) degradation[J]. Int J Mol Sci, 2023, 24(5): 4896. doi: 10.3390/ijms24054896 [13] Zucoloto A Z, Jenne C N. Platelet-neutrophil interplay: Insights into neutrophil extracellular trap (NET)-driven coagulation in infection[J]. Front Cardiovasc Med, 2019, 6: 85. doi: 10.3389/fcvm.2019.00085 [14] Rodrigues L C, Kabeya L M, Azzolini A E C S, et al. Galectin-1 modulation of neutrophil reactive oxygen species production depends on the cell activation state[J]. Mol Immunol, 2019, 116: 80-89. doi: 10.1016/j.molimm.2019.10.001 [15] Lin W, Chen H, Chen X, et al. The roles of neutrophil-derived myeloperoxidase (MPO) in diseases: The new progress[J]. Antioxidants, 2024, 13(1): 132. doi: 10.3390/antiox13010132 [16] Perumal R, Konduru A, Rengasamy S. Serum ceruloplasmin-to-albumin ratio as a biochemical marker in pulmonary tuberculosis before and after treatment[J]. Cureus, 2024, 16(6): e62275. doi: 10.7759/cureus.62275 [17] Smyła-Gruca W, Szczurek-Wasilewicz W, Skrzypek M, et al. Ceruloplasmin and lipofuscin serum concentrations are associated with presence of hypertrophic cardiomyopathy[J]. Biomedicines, 2024, 12(8): 1767. doi: 10.3390/biomedicines12081767 [18] Wang T, Yan W, Zhang M, et al. Effects of extracorporeal membrane oxygenation on the coagulation system[J]. JoVE, 2024(204): e66433. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 6
- HTML全文浏览量: 3
- PDF下载量: 0
- 被引次数: 0
