

Correlation and Significance of FCN3,IGF-1 and Immune Function in Children with Recurrent Respiratory Tract Infection
-
摘要:
目的 探讨血清纤维胶凝蛋白3(Fibroin 3,FCN3)联合胰岛素样生长因子1(insulin-like growth factor 1,IGF-1)评估儿童反复呼吸道感染(recurrent respiratory tract infection,RRTIs)效能及与免疫功能相关性。 方法 选取2022年9月至2024年8月自贡市妇幼保健院收治的142例RRTIs患儿(RRTIs组)、142例急性偶发呼吸道感染患儿(感染组),另选同期50例健康儿童作为对照组。另选2024年9月至2025年1月50例儿童呼吸道感染患儿作为验证集进行前瞻性队列验证。比较3组基线资料及血清FCN3、IGF-1水平。分析FCN3、IGF-1对RRTIs发生风险的评估价值。比较3组免疫功能(CD3+ T淋巴细胞、CD4+ T淋巴细胞、CD4+/CD8+),并分析其与血清FCN3、IGF-1水平相关性。 结果 RRTIs组血清FCN3、IGF-1水平低于感染组、对照组(P < 0.05),且感染组血清FCN3水平低于对照组(P < 0.05),而感染组、对照组血清IGF-1水平对比,差异无统计学意义(P > 0.05);FCN3升高、IGF-1升高是RRTIs的独立相关保护因素(P < 0.05);血清FCN3、IGF-1联合评估RRTIs的AUC值大于血清FCN3、IGF-1(P < 0.05);RRTIs组CD3+ T淋巴细胞、CD4+ T淋巴细胞、CD4+/CD8+低于感染组、对照组,且感染组低于对照组(P < 0.05);血清FCN3、IGF-1水平与CD3+ T淋巴细胞、CD4+ T淋巴细胞、CD4+/CD8+呈正相关(P < 0.05);经Kappa值一致性分析显示,验证集中FCN3、IGF-1联合ROC结果与临床实际的符合率为90.00%,Kappa值为0.799(95%CI:0.524~0.912)(P < 0.001)。 结论 RRTIs患儿血清FCN3、IGF-1水平与免疫功能密切相关,联合检测其水平对RRTIs发生风险具有一定评估价值。 Abstract:Objective To investigate the efficacy of combining serum fibronectin 3 (FCN3) with insulin-like growth factor 1 (IGF-1) in evaluating recurrent respiratory tract infections (RRTIs) in children and its correlation with immune function. Methods A total of 142 children with RRTIs (RRTIs group) and 142 children with acute occasional respiratory tract infection (infection group) admitted to Zigong Maternal and Child Health Hospital from September 2022 to August 2024 were selected. Additionally, 50 healthy children during the same period were selected as the control group. Another 50 children with respiratory tract infection from September 2024 to January 2025 were selected as the validation set for prospective cohort validation. The baseline data and serum levels of FCN3 and IGF-1 were compared among the three groups. The evaluation value of FCN3 and IGF-1 for the risk of RRTIs was analyzed. The immune functions (CD3+ T lymphocytes, CD4+ T lymphocytes, CD4+/CD8+) were compared among the three groups, and their correlation with serum level of FCN3 and IGF-1 was analyzed. Results The levels of serum FCN3 and IGF-1 in the RRTIs group were lower than those in the infection group and the control group (P < 0.05), the level of serum FCN3 in the infection group was lower than that in the control group, However, there was no significant difference in the levels of serum IGF-1 between the infection group and the control group (P > 0.05). Elevated FCN3 and IGF-1 were independently associated protective factors for RRTIs (P < 0.05). The AUC value of the combined evaluation of RRTIs using serum FCN3 and IGF-1 is greater than that of serum FCN3 and IGF-1 (P < 0.05). The levels of CD3+ T lymphocytes, CD4+ T lymphocytes, and CD4+/CD8+ in the RRTIs group were lower than those in the infection group and the control group, with the infection group having lower levels than the control group (P < 0.05). The levels of serum FCN3 and IGF-1 were positively correlated with CD3+ T lymphocytes, CD4+ T lymphocytes, and CD4+/CD8+ (all P < 0.05). The Kappa value consistency analysis showed that the coincidence rate of the ROC results of FCN3 and IGF-1 combined with clinical practice in the validation set was 90.00 %, and the Kappa value was 0.799 (95%CI: 0.524~0.912) (P < 0.001). Conclusion The levels of serum FCN3 and IGF-1 in children with RRTIs are closely related to immune function, and the combined detection of their levels has certain evaluation value for the risk of RRTIs. -
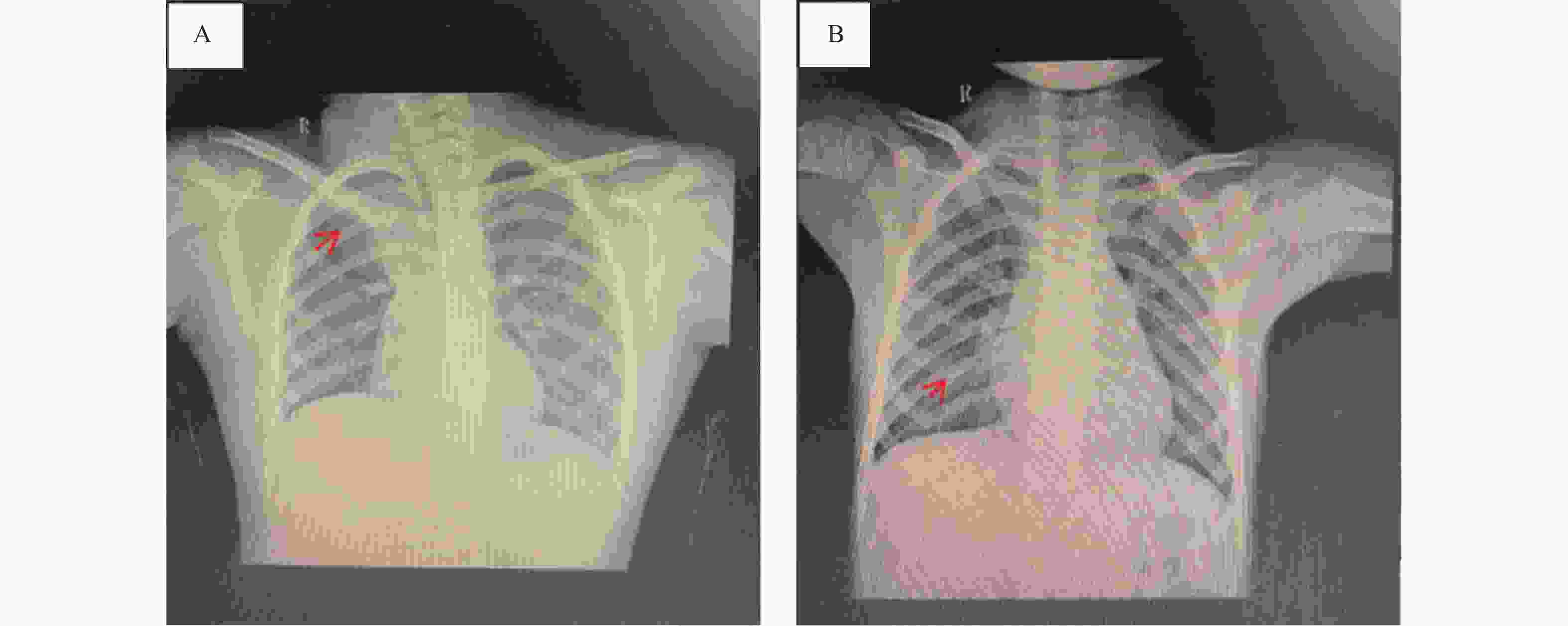
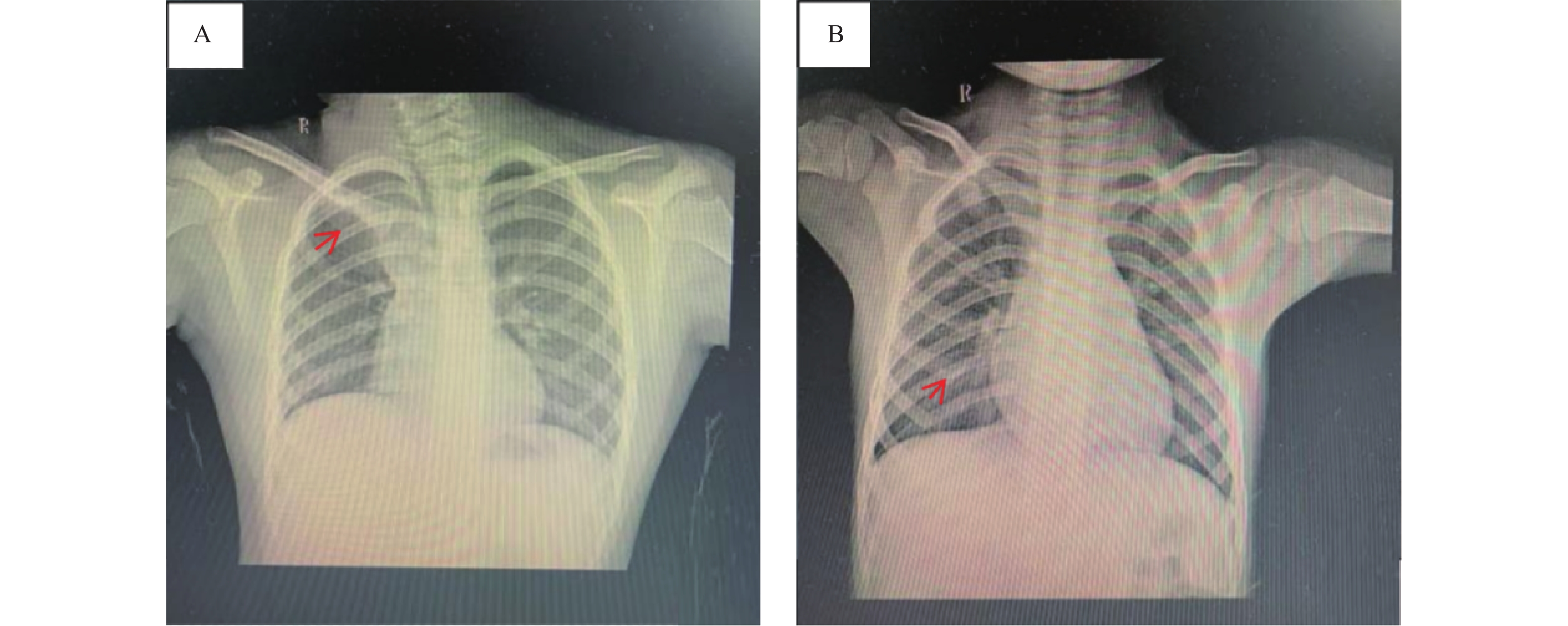
图 1 感染组部分患儿影像表现
A:右肺上叶各段见大片状肺组织实变影,可见少许含气支气管影,右肺上叶肺部体积缩小,右肺上叶各段支气管开口狭窄;左肺下叶外基底段微小结节影,边界模糊;纵膈内及双侧肺门未见增大淋巴结;心脏大小形态未见异常;胸廓对称,胸部骨质未见确切异常,下呼吸道(肺部)的炎症改变;B:胸廓对称,所见骨质结构完整,未见异常改变;双肺纹理增多、增粗,纹理间可见少许斑片状模糊影,双侧肺门结构未见异常,心外形未见异常,膈光滑,肋膈角锐利,下呼吸道(肺部)的炎症改变。
Figure 1. Imaging findings of some children in the infection group
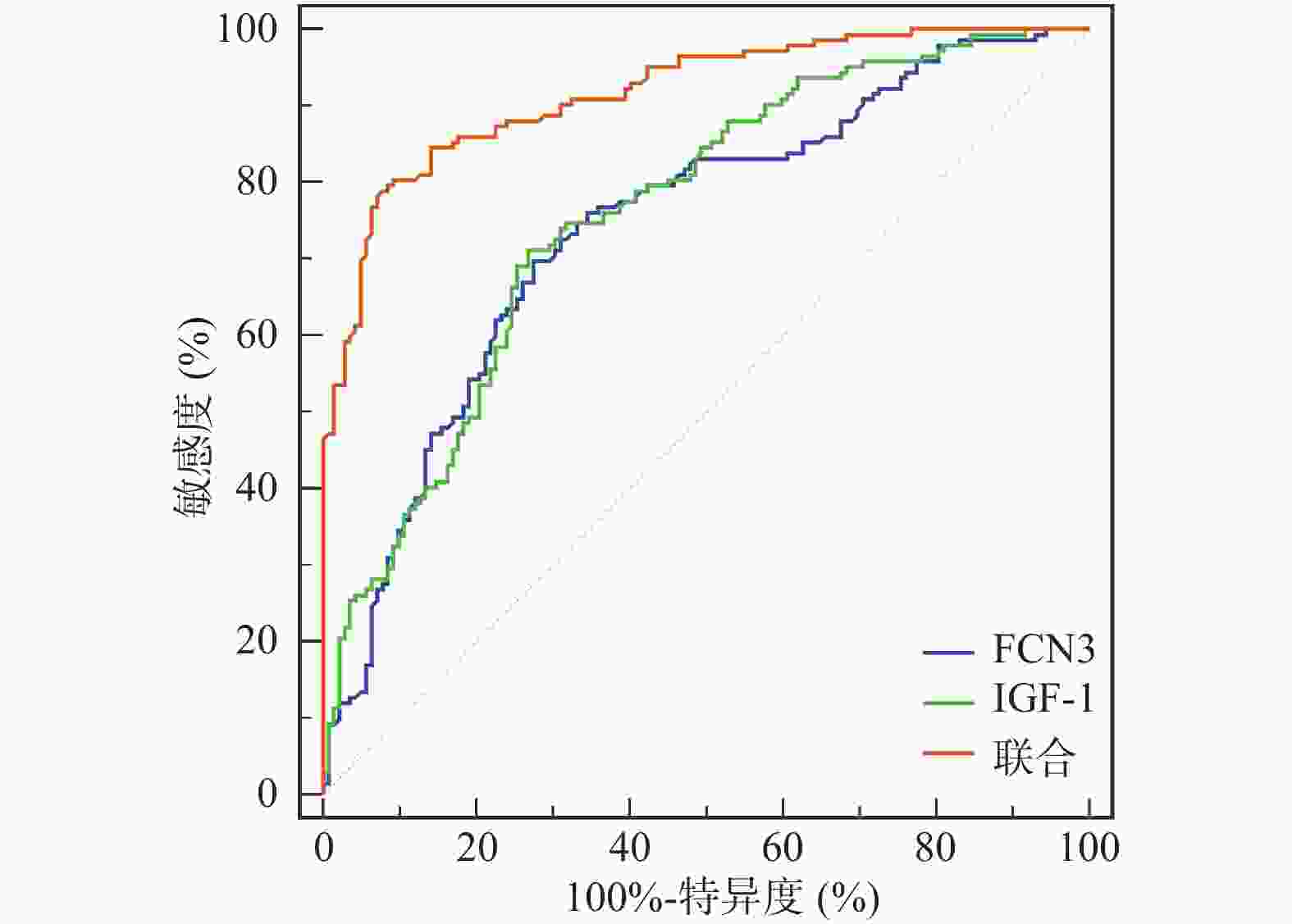
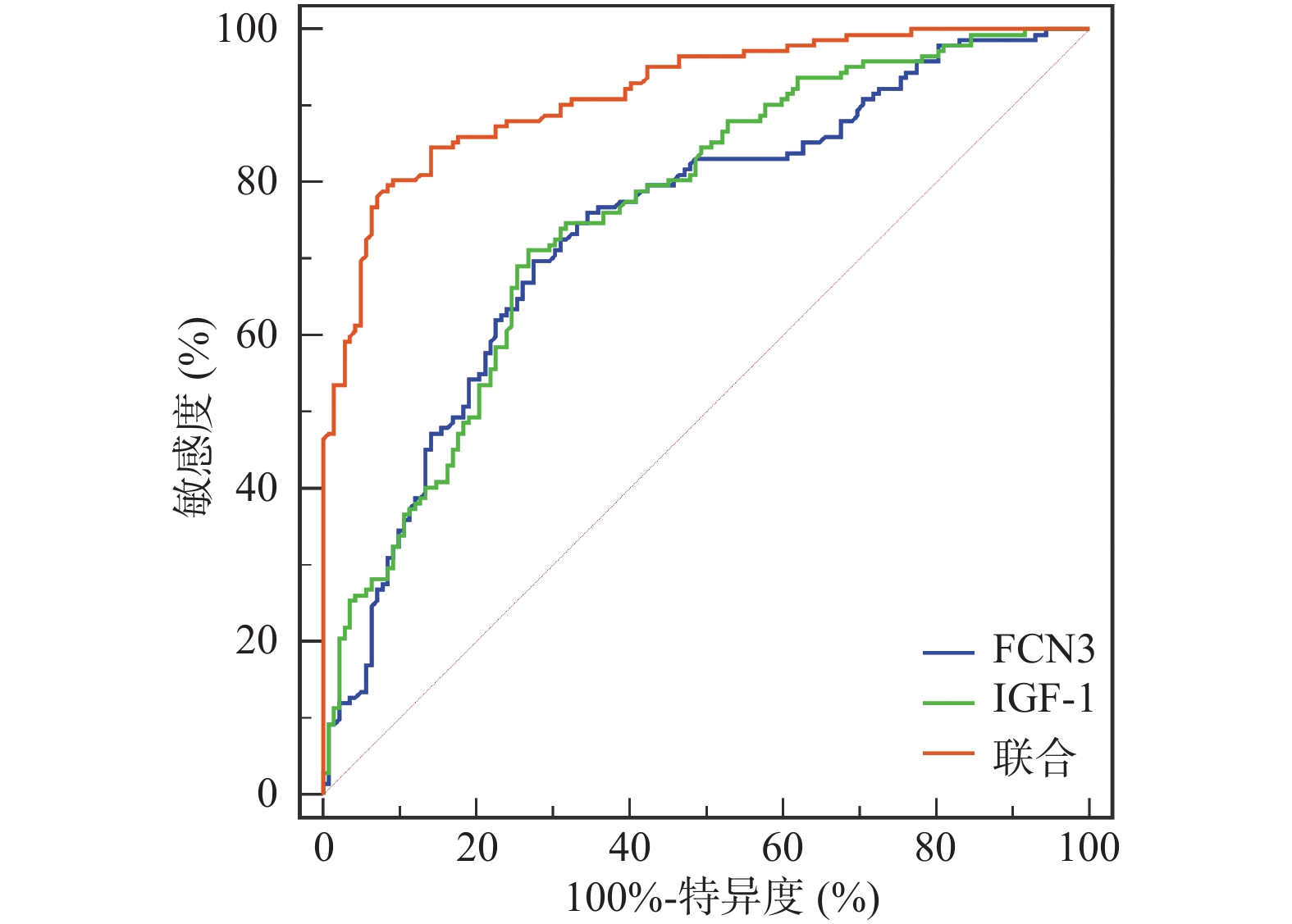
图 2 血清FCN3、IGF-1表达及联合评估RRTIs风险的ROC曲线
Figure 2. ROC curves for serum FCN3,IGF-1 expression and combined assessment of risk of RRTIs
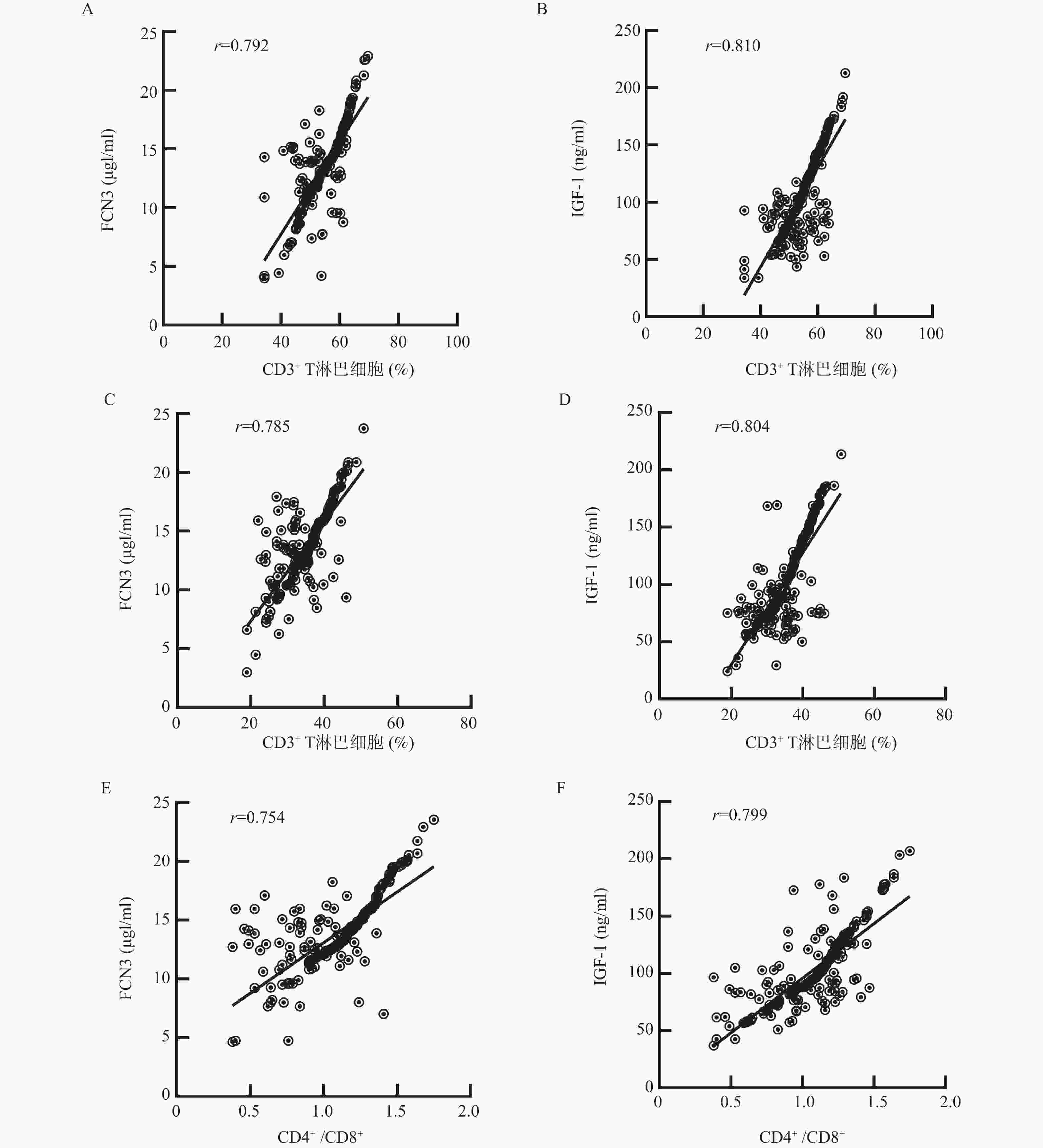
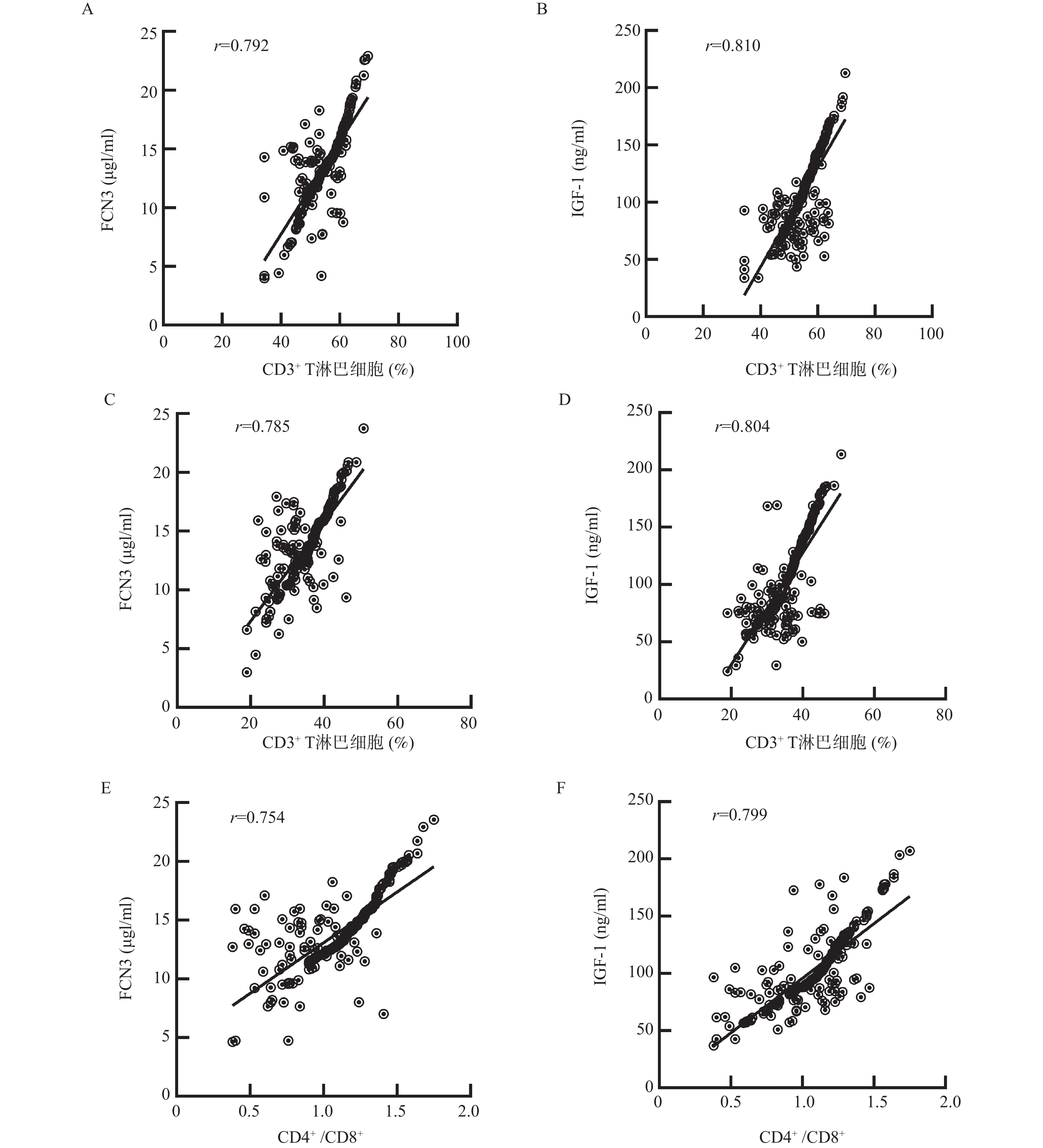
图 3 血清FCN3、IGF-1与免疫功能相关性($ \bar x \pm s $)
A:FCN3与CD3+ T淋巴细胞相关性;B:IGF-1与CD3+ T淋巴细胞相关性;C:FCN3与CD4+ T淋巴细胞相关性;D:IGF-1与CD4+ T淋巴细胞相关性;E:FCN3与CD4+/CD8+相关性;F:IGF-1与CD4+/CD8+相关性。
Figure 3. Correlation between serum FCN3,IGF-1 and immune function($ \bar x \pm s $)
表 1 3组基线资料比较[n (%)/($ \bar x \pm s $)]
Table 1. Comparison of baseline data among three groups[n (%)/($ \bar x \pm s $)]
资料 RRTIs组(n = 142) 感染组(n = 142) 对照组(n = 50) F/χ2/u P 年龄(岁) 2.16 ± 0.69 1.97 ± 0.62 2.08 ± 0.66 2.984 0.052 性别 0.128 0.938 男 67(47.18) 70(49.30) 24(48.00) 女 75(52.82) 72(50.70) 26(52.00) 体重(kg) 12.25 ± 2.51 12.50 ± 2.67 12.45 ± 2.79 0.340 0.712 身高(cm) 87.66 ± 3.40 88.03 ± 4.19 88.10 ± 4.26 0.414 0.662 民族 2.224 0.329 汉族 131(92.25) 134(94.37) 49(98.00) 少数民族 11(7.75) 8(5.63) 1(2.00) 常驻地 0.521 0.771 城市 104(73.24) 101(71.13) 34(68.00) 农村 38(26.76) 41(28.87) 16(32.00) 过敏性鼻炎 0.115 0.944 无 135(95.07) 136(95.77) 48(96.00) 有 7(4.93) 6(4.23) 2(4.00) 腺样体肥大 0.532 0.766 无 136(95.77) 137(96.48) 49(98.00) 有 6(4.23) 5(3.52) 1(2.00) 感染部位 0.580 0.446 上呼吸道感染 113(79.58) 118(83.10) − 下呼吸道感染 29(20.42) 24(16.90) − 喂养史 14.563 0.001* 母乳 70(49.30) 98(69.01) 36(72.00) 人工 72(50.70) 44(30.99) 14(28.00) RRTIs家族史 20(14.08) 5(3.52) 1(2.00) 13.777 0.001* 被动吸烟 34(23.94) 9(6.34) 2(4.00) 23.404 < 0.001* 流感疫苗接种 18(12.68) 33(23.24) 12(24.00) 6.191 0.045* 营养不良 2(1.41) 1(0.70) 0(0.00) 0.929 0.629 *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 3组血清FCN3、IGF-1表达比较($ \bar x \pm s $)
Table 2. Comparison of serum FCN3 and IGF-1 expression among three groups ($ \bar x \pm s $)
组别 n FCN3(μg/mL) IGF-1(ng/mL) RRTIs组 142 12.60 ± 2.79△# 78.63 ± 17.20△# 感染组 142 14.03 ± 3.55△ 129.79 ± 26.15 对照组 50 16.10 ± 4.84 133.89 ± 24.78 F 19.542 219.672 P < 0.001* < 0.001* *P < 0.05;与对照组比较,△P < 0.05;与感染组比较,#P < 0.05。
下载: 导出CSV
表 3 RRTIs的多因素分析
Table 3. Multivariate analysis of RRTIs
自变量 β SE Wald χ2 OR 95%CI P 下限 上限 FCN3 −1.529 0.366 17.461 0.217 0.106 0.444 < 0.001* IGF-1 −1.673 0.415 16.258 0.188 0.083 0.423 < 0.001* 常数项 0.240 0.062 14.938 − − − < 0.001* *P < 0.001。
下载: 导出CSV
表 4 血清FCN3、IGF-1表达及联合评估RRTIs风险的参数
Table 4. Serum FCN3,IGF-1 expression and parameters for combined assessment of risk of RRTIs
指标 AUC 95%CI 约登指数 cut-off 敏感度(%) 特异度(%) P FCN3 0.742 0.687~0.792 0.423 13.40 69.72 72.54 < 0.001* IGF-1 0.759 0.705~0.807 0.444 89.85 71.13 73.24 < 0.001* 联合 0.917 0.879~0.946 0.711 80.28 90.85 < 0.001* *P < 0.001。
下载: 导出CSV
表 5 3组免疫功能比较($ \bar x \pm s $)
Table 5. Comparison of immune function among three groups ($ \bar x \pm s $)
组别 n CD3+ T淋巴细胞(%) CD4+ T淋巴细胞(%) CD4+/CD8+ RRTIs组 142 51.20 ± 6.45△# 32.40 ± 5.11△# 0.93 ± 0.22△# 感染组 142 56.49 ± 5.22△ 37.89 ± 4.30△ 1.24 ± 0.20△ 对照组 50 65.00 ± 4.79 44.00 ± 3.87 1.69 ± 0.17 F 111.184 128.992 266.897 P < 0.001* < 0.001* < 0.001* *P < 0.001;与对照组比较,△P < 0.05;与感染组比较,#P < 0.05。
下载: 导出CSV
-
[1] Zhou B, Niu W, Liu F, et al. Risk factors for recurrent respiratory tract infection in preschool-aged children[J]. Pediatr Res, 2021, 90(1): 223-231. doi: 10.1038/s41390-020-01233-4 [2] 范芳, 汤丽萍, 牛焕红, 等. 儿童反复呼吸道感染影响因素分析[J]. 检验医学与临床, 2021, 18(4): 469-472. [3] Li Y, You E Q, Lin W H, et al. Association of ficolin-1 and ficolin-3 gene variation and pulmonary tuberculosis susceptibility in a Chinese population[J]. Clinical Laboratory Analysis, 2021, 35(4): e23732. doi: 10.1002/jcla.23732 [4] Dadfar E, Furuhjelm C, Nilsson J, et al. Fatal pneumococcus meningitis in a child with complement factor ficolin-3 deficiency[J]. J Allergy Clin Immunol Pract, 2020, 8(2): 778-779. doi: 10.1016/j.jaip.2019.07.039 [5] 齐姣, 靳丽丽, 杨月君, 等. 脑梗死病人血清SIL-2R、IGF-1、hs-CRP表达水平与继发肺部感染的关系[J]. 中西医结合心脑血管病杂志, 2024, 22(6): 1135-1138. doi: 10.12102/j.issn.1672-1349.2024.06.034 [6] 范芳, 汤丽萍, 牛焕红, 等. 儿童反复呼吸道感染影响因素分析[J]. 检验医学与临床, 2021, 18(4): 469-472. [7] 中华医学会儿科学分会呼吸学组, 《中华儿科杂志》编辑委员会. 反复呼吸道感染的临床概念和处理原则[J]. 中华儿科杂志, 2008, 46(2): 108-110. [8] 胡亚美. 诸福棠实用儿科学(第7版)[M]. 北京: 人民卫生出版社, 2005: 125-141. [9] 重庆市健康促进与健康教育学会儿科临床专委会, 程杰, 李洪东, 等. 儿童反复呼吸道感染防治重庆专家共识[J]. 中国药业, 2025, 34(22): 1-7. doi: 10.3969/j.issn.1006-4931.2025.22.001 [10] Wang X, Yin L, Bai X, et al. Pediatric Tuina for recurrent respiratory tract infection in children: A systematic review and meta-analysis[J]. Medicine, 2023, 102(51): e36655. doi: 10.1097/MD.0000000000036655 [11] Braido F, Melioli G, Nicocini G, et al. Prevention of recurrent respiratory tract infections: a literature review of the activity of the bacterial lysate Lantigen B[J]. Eur Rev Med Pharmacol Sci, 2023, 27(16): 7756-7767. [12] Blangy-Letheule A, Vergnaud A, Dupas T, et al. Value of a secretomic approach for distinguishing patients with COVID-19 viral pneumonia among patients with respiratory distress admitted to intensive care unit[J]. J Med Virol, 2024, 96(6): e29756. doi: 10.1002/jmv.29756 [13] Jang H, Jun Y, Kim S, et al. FCN3 functions as a tumor suppressor of lung adenocarcinoma through induction of endoplasmic reticulum stress[J]. Cell Death Dis, 2021, 12(4): 407. doi: 10.1038/s41419-021-03675-y [14] 艾忠华, 向学兰. 反复呼吸道感染患儿血清FCN3、25羟维生素D、IGF-1水平与孟鲁司特钠疗效的关系[J]. 中国医药指南, 2024, 22(27): 86-90. doi: 10.15912/j.issn.1671-8194.2024.27.025 [15] 孙立华, 董一慧, 孙莉莉. 血清纤维胶凝蛋白3、甲壳质酶蛋白-40对肺炎支原体肺炎患儿发生反复呼吸道感染的预测价值[J]. 检验医学与临床, 2025, 22(12): 1611-1616. doi: 10.3969/j.issn.1672-9455.2025.12.006 [16] Feizollahi P, Matin S, Roghani S A, et al. Evaluation serum levels of Insulin Growth Factor-1 (IGF-1) and its association with clinical parameters in severe COVID-19[J]. Inflammopharmacology, 2022, 30(1): 199-205. doi: 10.1007/s10787-021-00908-6 [17] Cui H, Zhang S, Wu Z, et al. Insulin-like growth factor-1 reduces hyperoxia-induced lung inflammation and oxidative stress and inhibits cell apoptosis through PERK/eIF2α/ATF4/CHOP signaling[J]. Exp Lung Res, 2022, 48(4-6): 187-197. doi: 10.1080/01902148.2022.2106388 [18] 尹杨艳, 陈丹丹, 桂冬梅. 反复呼吸道感染患儿血清维生素和IGF-1及T淋巴细胞亚群水平及临床意义[J]. 中华医院感染学杂志, 2021, 31(8): 1254-1257. doi: 10.11816/cn.ni.2021-202227 [19] Gul A, Khan S, Arshad M, et al. Peripheral blood T cells response in human parainfluenza virus-associated lower respiratory tract infection in children[J]. Saudi J Biol Sci, 2020, 27(10): 2847-2852. doi: 10.1016/j.sjbs.2020.07.005 [20] 卢红霞, 黄晗, 郭燕军, 等. 儿童难治性支原体肺炎白细胞介素-8、白细胞介素-17、CD4-CD8比值与病情及预后的相关性研究[J]. 安徽医药, 2021, 25(12): 2411-2415. doi: 10.3969/j.issn.1009-6469.2021.12.019 [21] Li H, Cui Q K, Li Z, et al. Clinical observation of the effect of modified Ginseng-Schisandra decoction (MGSD) on trace elements and immune function in children with spleen deficiency syndrome after recurrent respiratory tract infection (RRTI): A randomized controlled trial[J]. Transl Pediatr, 2021, 10(6): 1692-1700. doi: 10.21037/tp-21-243 [22] Verwey C, Nunes M C, Dangor Z, et al. Pulmonary function sequelae after respiratory syncytial virus lower respiratory tract infection in children: A systematic review[J]. Pediatr Pulmonol, 2020, 55(7): 1567-1583. doi: 10.1002/ppul.24804 [23] 贺媛媛, 贺陈龙, 李雅然, 等. 反复呼吸道感染患儿维生素A、D、E水平及免疫功能指标的相关性[J]. 贵州医科大学学报, 2020, 45(11): 1347-1350. doi: 10.19367/j.cnki.2096-8388.2020.11.021 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 317
- HTML全文浏览量: 188
- PDF下载量: 97
- 被引次数: 0
