

Construction of An Early Warning Model for Upper Gastrointestinal Bleeding in Patients with Cirrhotic Portal Hypertension Based on Serum miR-140 and miR-335-5p Combined with Clinical Indicators
-
摘要:
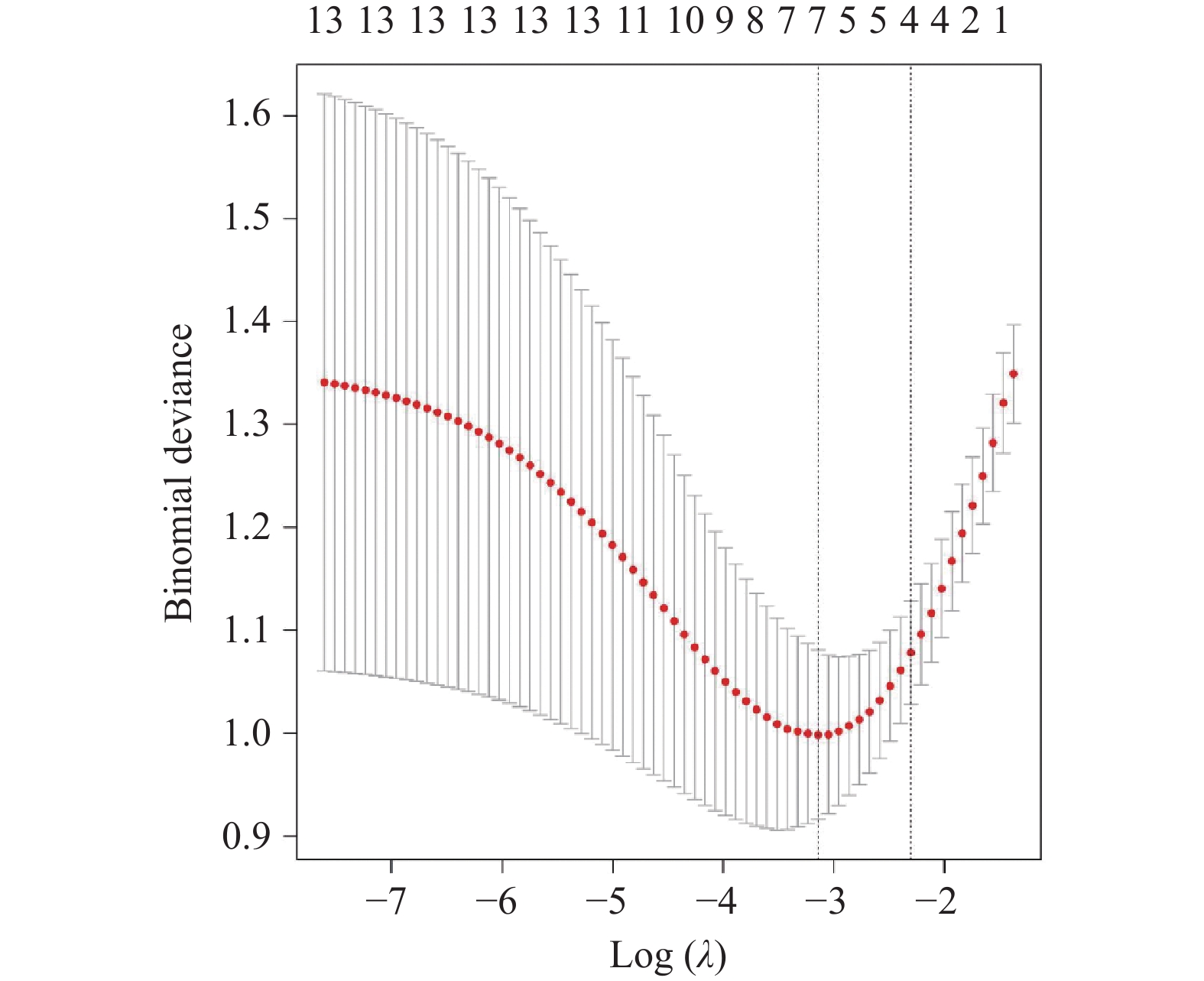
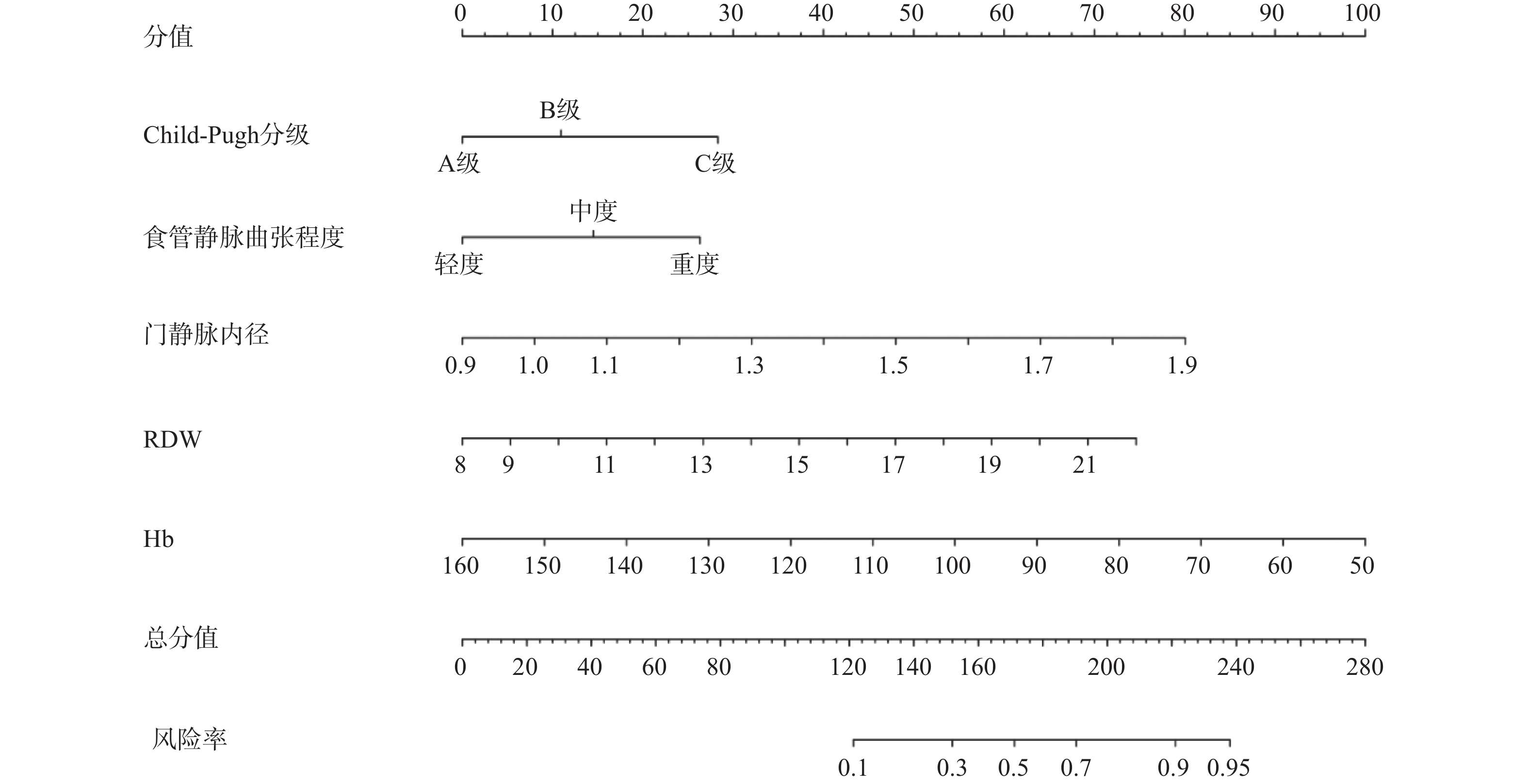
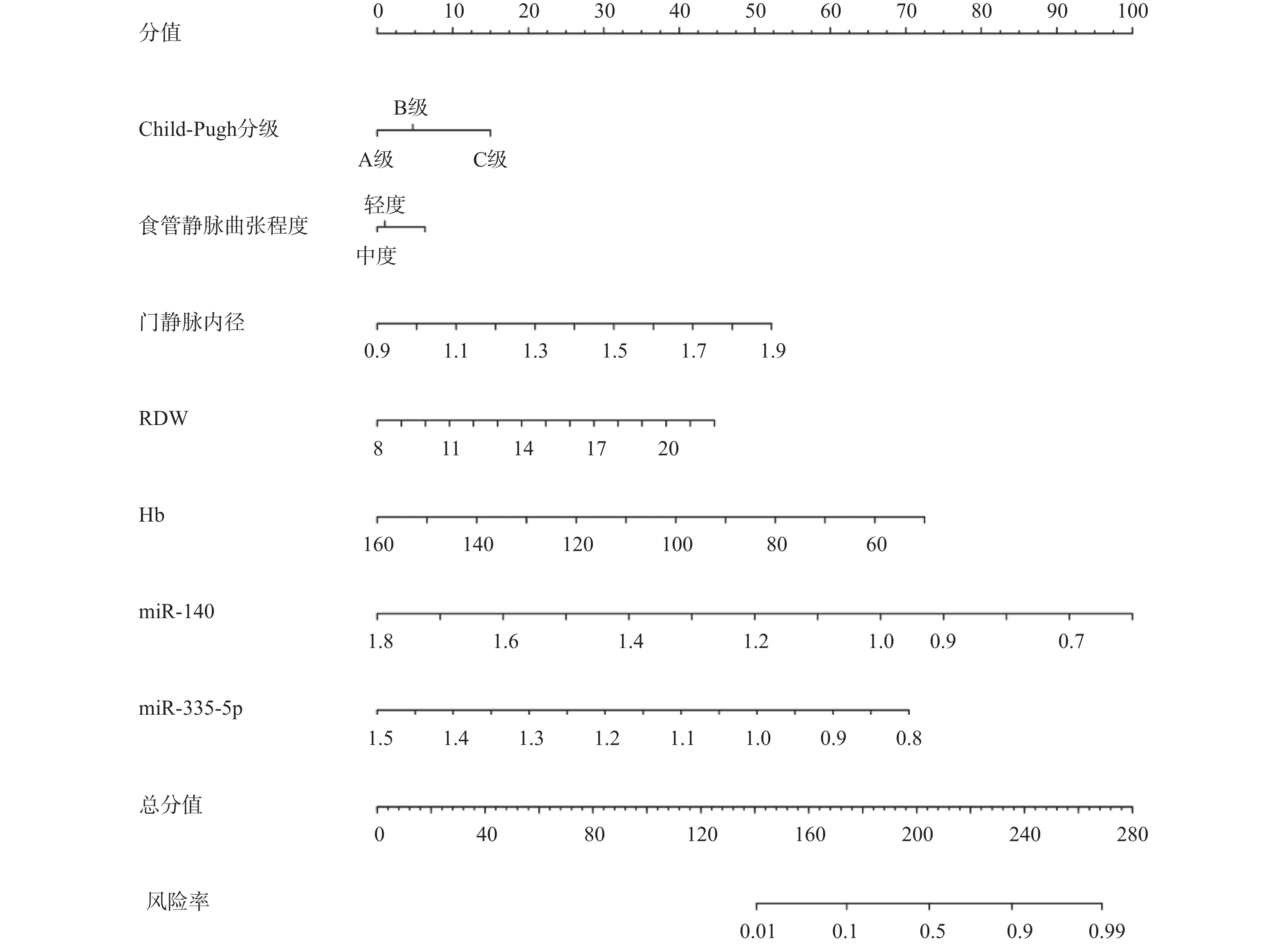
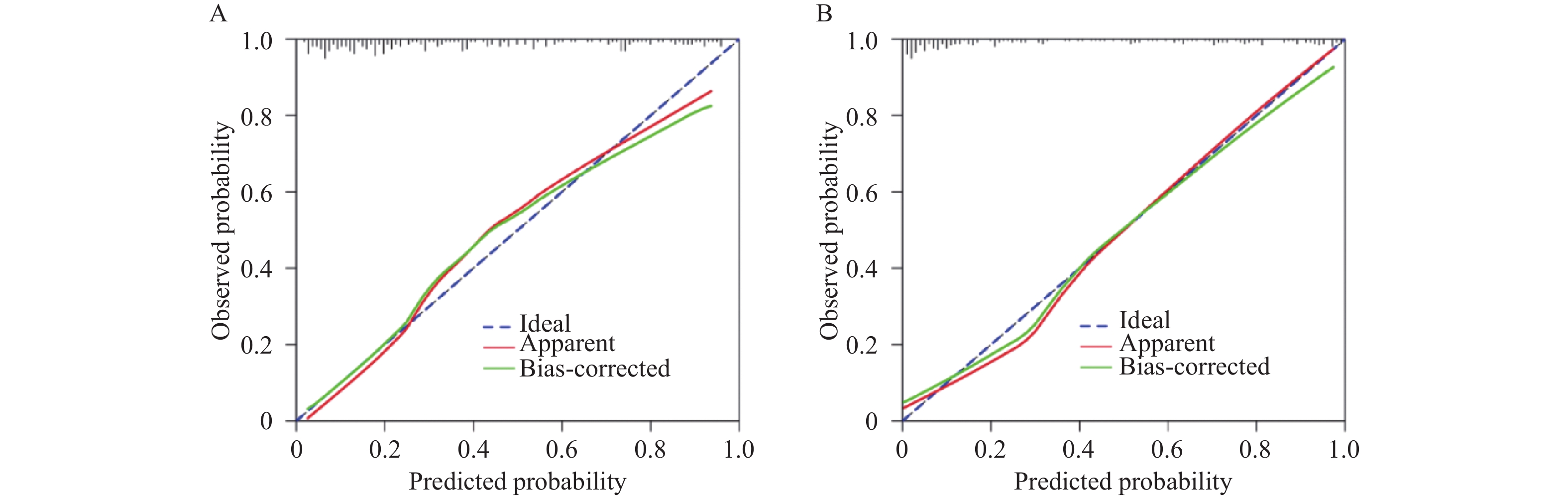
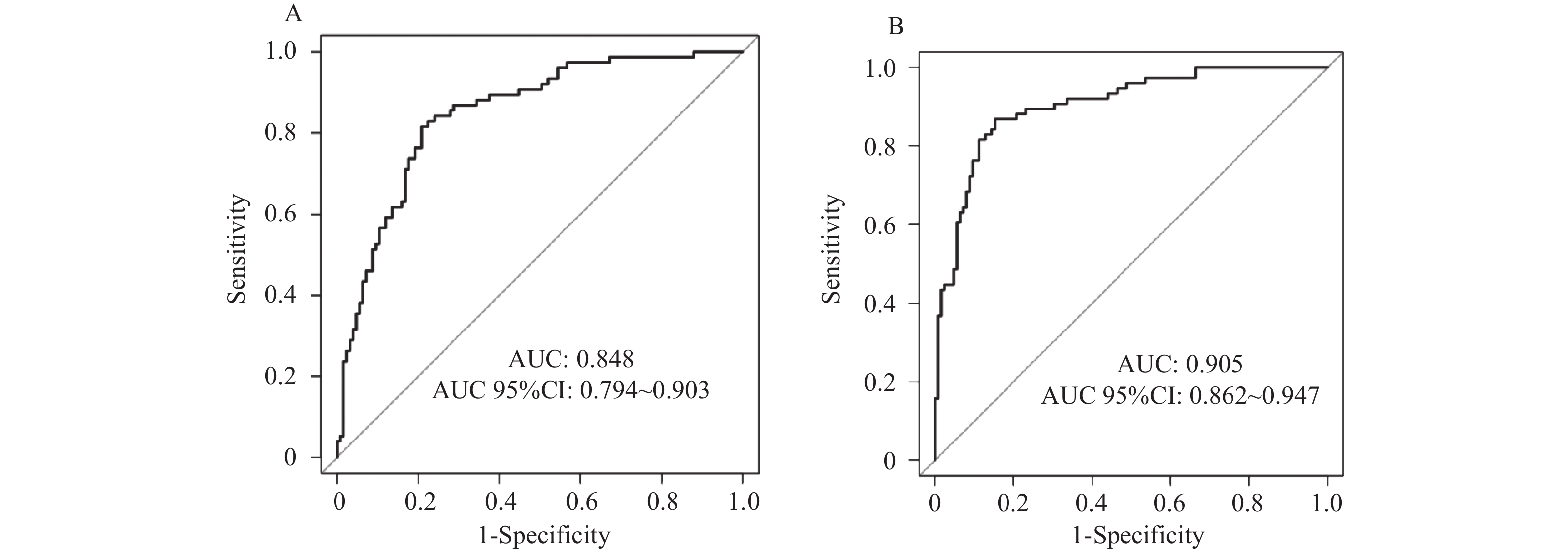
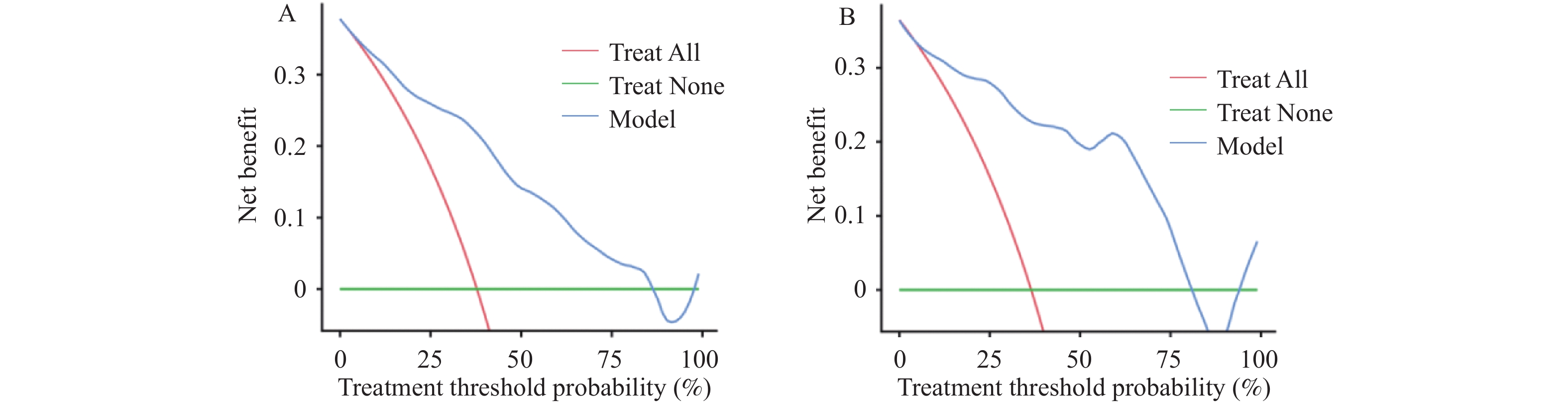
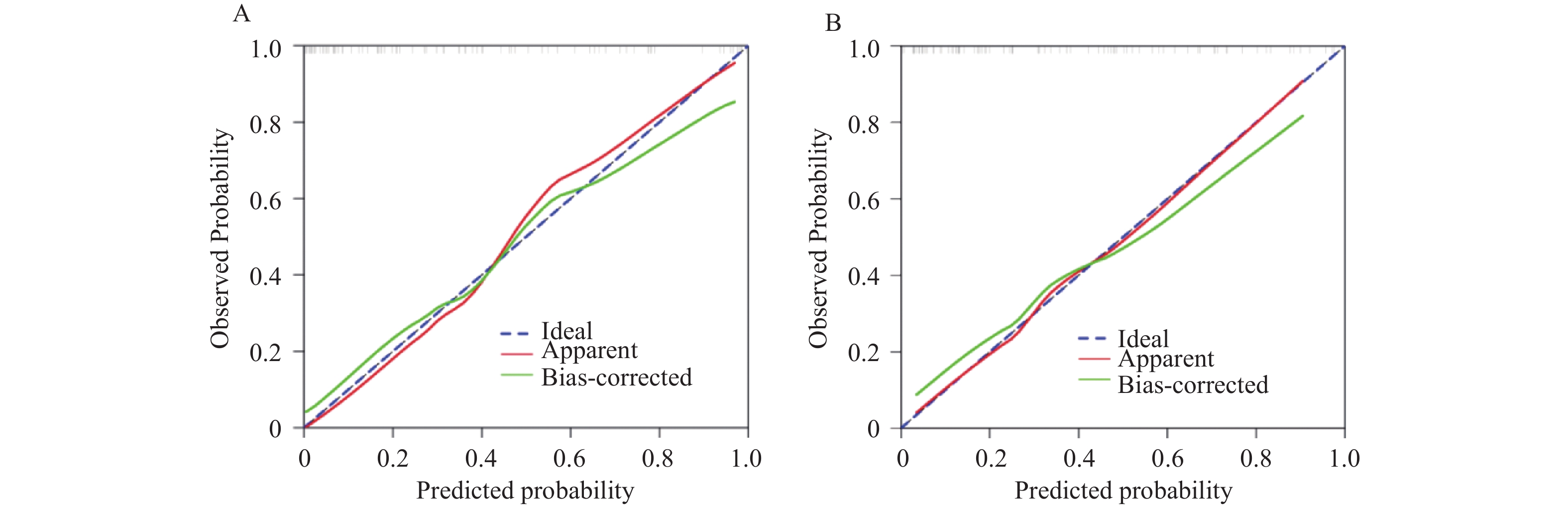
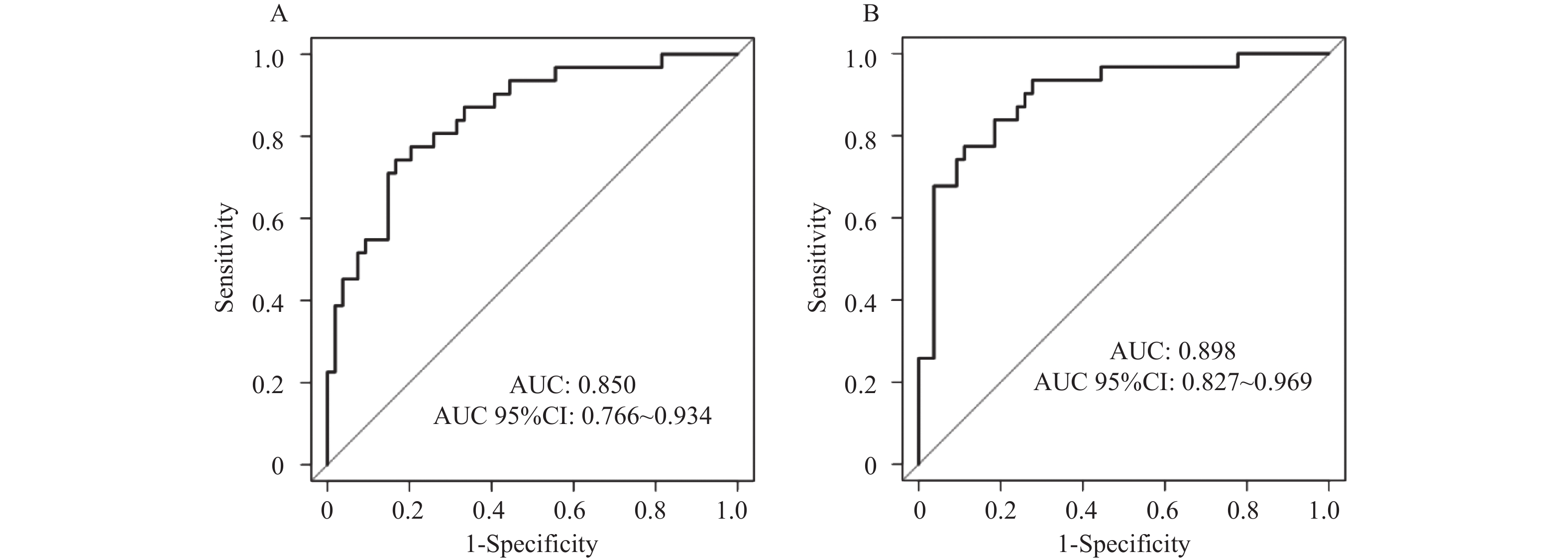
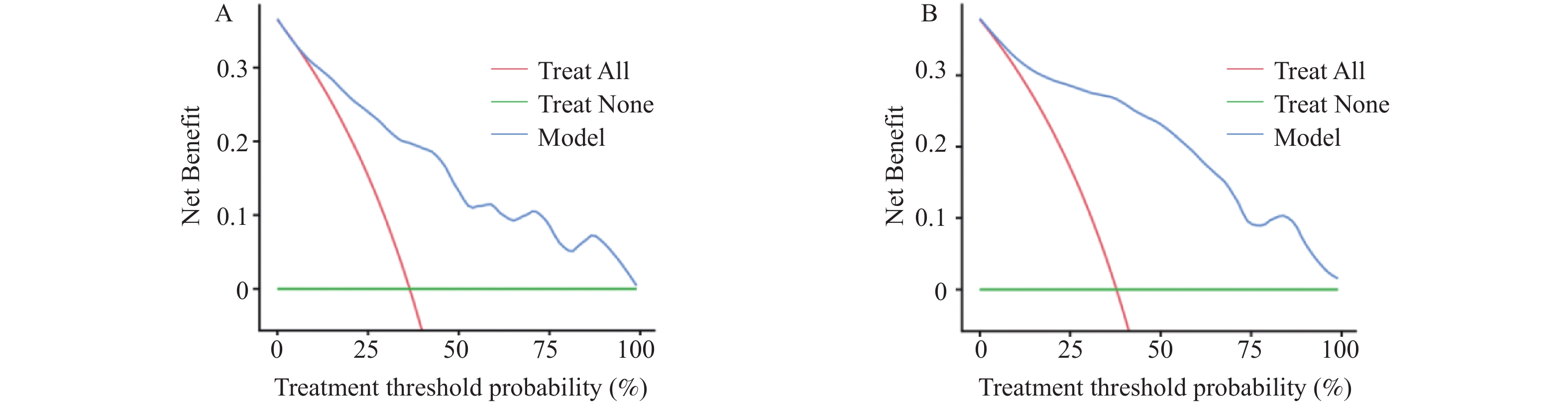
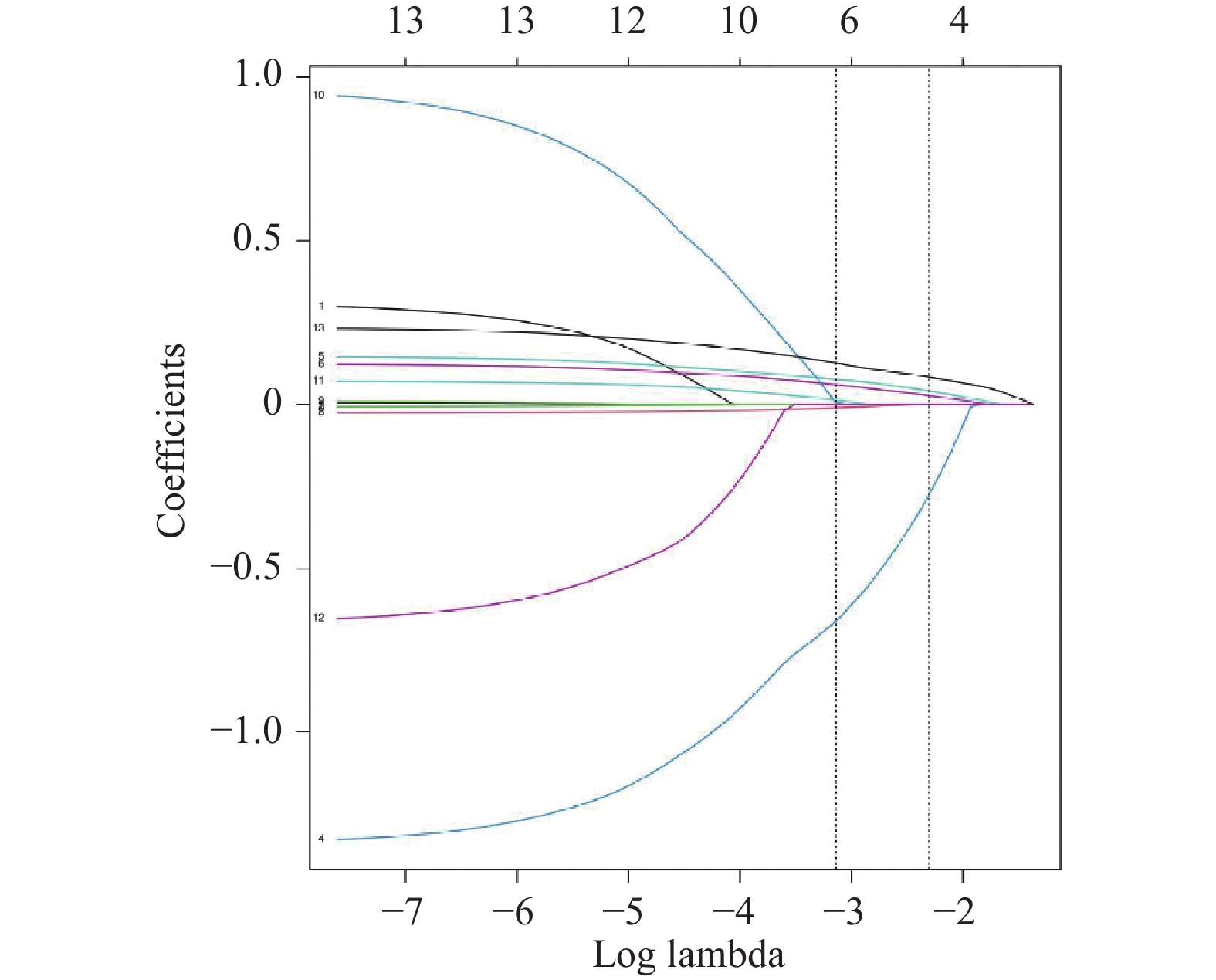
目的 基于血清微小核糖核酸-140(micro ribonucleic acid-140,miR-140)与微小核糖核酸-335-5p(micro ribonucleic acid-335-5p,miR-335-5p)联合临床指标构建肝硬化门静脉高压(cirrhosis with portal hypertension,CPH)患者上消化道出血(upper gastrointestinal bleeding,UGIB)的预警模型,并评估其预测效能。 方法 选取2021年3月至2024年8月太原市中心医院CPH患者作为研究对象,按照7∶3的比例分为训练集与验证集,随访1年,统计UGIB发生情况,收集临床资料,检测血清miR-140、miR-335-5p水平,采用Lasso-Logistic回归分析筛选CPH并发UGIB的独立预测因子,构建预警模型,采用校正曲线、受试者工作特征(receiver operating characteristic,ROC)曲线及临床决策曲线(decision curve analysis,DCA)评价和验证预警模型的价值。 结果 本研究最终选取289例CPH患者,按照7∶3的比例分为训练集(203例)与验证集(86例)。随访1年,训练集203例CPH患者中失访2例,未发生UGIB 125例,发生UGIB 76例。验证集86例CPH患者中失访1例,未发生UGIB 54例,发生UGIB 31例。Lasso-Logistic回归分析,Child-Pugh分级、食管静脉曲张程度、门静脉内径、红细胞分布宽度(red cell distribution width,RDW)、血红蛋白(hemoglobin,Hb)、miR-140、miR-335-5p是CPH并发UGIB的独立影响因素(P < 0.05);基于Child-Pugh分级、食管静脉曲张程度、门静脉内径、RDW、Hb等5项临床指标构建M1预警模型,在此基础上联合miR-140和miR-335-5p构建M2预警模型,两个预警模型均拟合良好(P > 0.05);在训练集和验证集中,校正曲线显示,M1预警模型的一致性指数为0.802、0.806,校准度为0.800、0.801,M2预警模型的一致性指数为0.867、0.871,校准度为0.859、0.862,提示M2预警模型具有优异的区分能力和较高的预测精度;ROC曲线分析,M2、M1预警模型在训练集和验证集中预测CPH并发UGIB的曲线下面积(area under the curve,AUC)为0.905(95%CI:0.862~0.947)、0.898(95%CI:0.827~0.969),敏感度为88.16%、83.87%,特异度为86.40%、81.48%,经Delong检验,M2预警模型的预测价值显著优于M1预警模型(Z = 2.192、1.986,P = 0.035、0.041);且M2预警模型的预测性能更优;DCA曲线显示,在训练集和验证集中M1、M2预警模型在10%~100%的广泛阈概率范围内,均展现出显著且稳定的临床正向净获益,且M2预警模型临床效用性更强。 结论 基于血清miR-140与miR-335-5p联合临床指标构建的预警模型是预测CPH患者发生UGIB风险的有效工具,可实现早期风险分层并优化临床决策。 -
关键词:
- 肝硬化门静脉高压 /
- 上消化道出血 /
- 微小核糖核酸-140 /
- 微小核糖核酸-335-5p /
- 临床指标 /
- 预警模型 /
- 预测效能
Abstract:Objective To construct an early warning model of upper gastrointestinal bleeding (UGIB) in patients with cirrhosis and portal hypertension (CPH) based on serum microRNA-140 (miR-140) and microRNA-335-5p (miR-335-5p) combined with clinical indicators, and to evaluate its predictive efficacy. Methods CPH patients in Taiyuan Central Hospital from March 2021 to August 2024 were selected as the research subjects and divided into training and validation sets in a 7:3 ratio. Patients were followed up for one year, with UGIB occurrence recorded. Clinical data were collected and serum levels of miR-140 and miR-335-5p were measured. Lasso-Logistic regression analysis was used to identify independent predictive factors for UGBI in CPH patients. An early warning model was constructed and validated using calibration curves, receiver operating characteristic (ROC) curves, and decision curve analysis (DCA). Results A total of 289 CPH patients were selected and divided into training set (203 cases) and validation set (86 cases) in a 7∶3 ratio. After one-year follow-up, in the training set, 2 patients were lost to follow-up, 125 did not develop UGIB, and 76 developed UGIB. In the validation set, 1 was lost to follow-up, 54 did not develop UGIB, and 31 developed UGIB. Lasso-Logistic regression analysis identified that Child-Pugh grade, esophageal varices severity, portal vein diameter, red cell distribution width (RDW), hemoglobin (Hb), miR-140 and miR-335-5p as independent factors for UGIB in CPH patients (P < 0.05). An M1 model was constructed based on five clinical indicators (Child-Pugh grade, esophageal varices severity, portal vein diameter, RDW, and Hb), while an M2 model incorporated miR-140 and miR-335-5p in addition to these indicators. Both models demonstrated good fit (P > 0.05). Calibration curves in both training and validation sets showed that the M1 model had concordance indices of 0.802 and 0.806 with calibration slopes of 0.800 and 0.801, while the M2 model had concordance indices of 0.867 and 0.871 with calibration slopes of 0.859 and 0.862, demonstrating superior discriminative ability and higher predictive accuracy for the M2 model. ROC curve analysis revealed that the areas under the curve (AUC) for M2 and M1 models in predicting UGIB in CPH were 0.905 (95%CI: 0.862-0.947) and 0.898 (95%CI: 0.827-0.969) in the training set, with sensitivities of 88.16% and 83.87%, and specificities of 86.40% and 81.48%, respectively. DeLong test demonstrated that the M2 model's predictive value was significantly superior to the M1 model (Z = 2.192, 1.986; P = 0.035, 0.041). DCA curves indicated that both M1 and M2 models demonstrated significant and stable positive net clinical benefit across a wide threshold probability range of 10%-100% in both datasets, with the M2 model exhibiting superior clinical utility. Conclusion The early warning model constructed based on serum miR-140 and miR-335-5p combined with clinical indicators is an effective tool for predicting UGIB in CPH patients, enabling early risk stratification and optimization of clinical decision-making. -
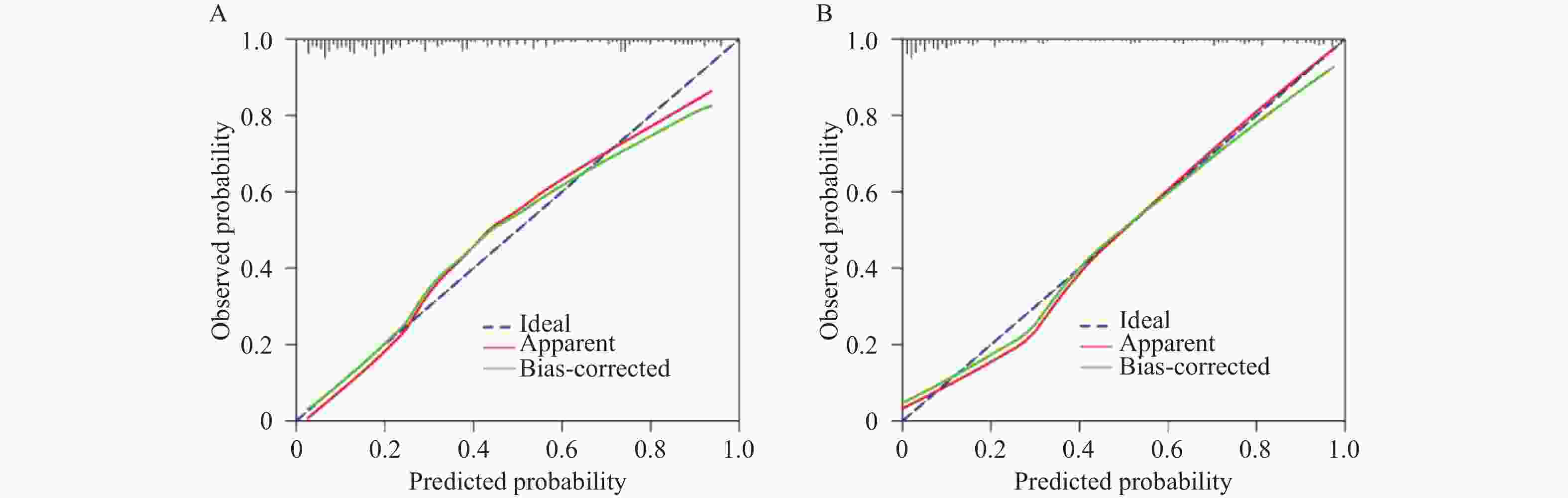
图 5 M1与M2预警模型在训练集中的校正曲线
A:M1预警模型的校正曲线;B:M2预警模型的校正曲线。
Figure 5. Calibration curves of M1 and M2 early warning models in the training set
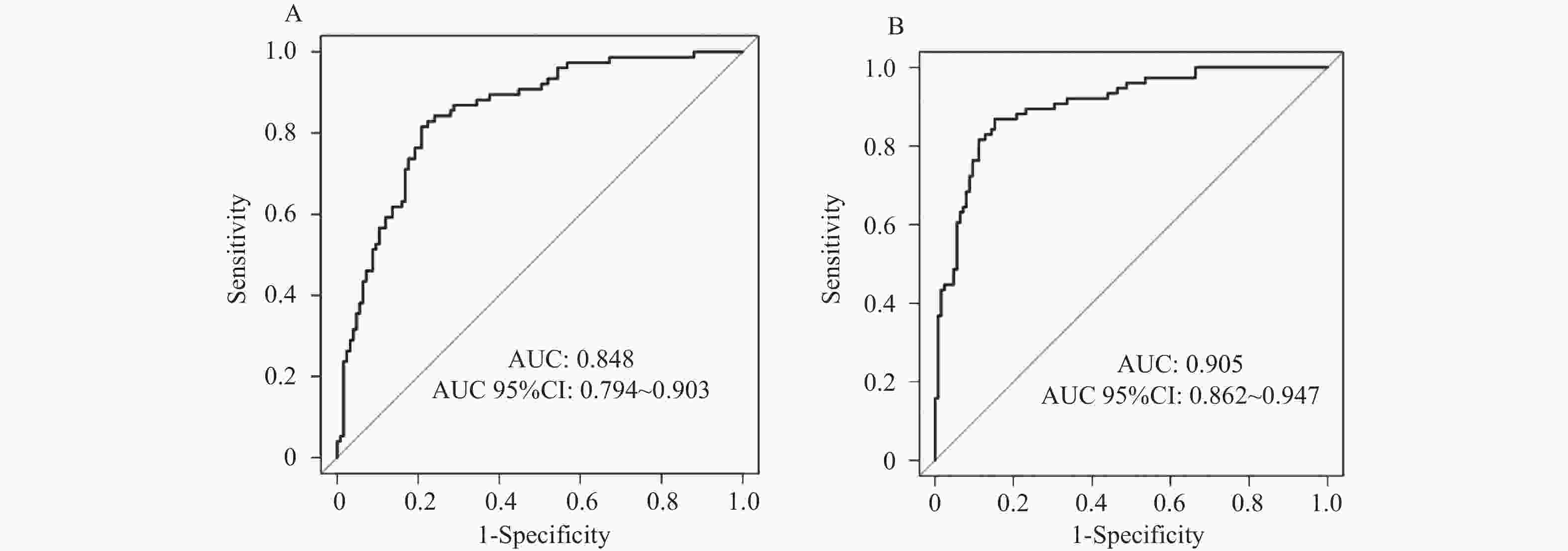
图 6 M1与M2预警模型在训练集中的ROC曲线
A:M1预警模型的ROC曲线;B:M2预警模型的ROC曲线。
Figure 6. ROC curves of M1 and M2 early warning models in the training set
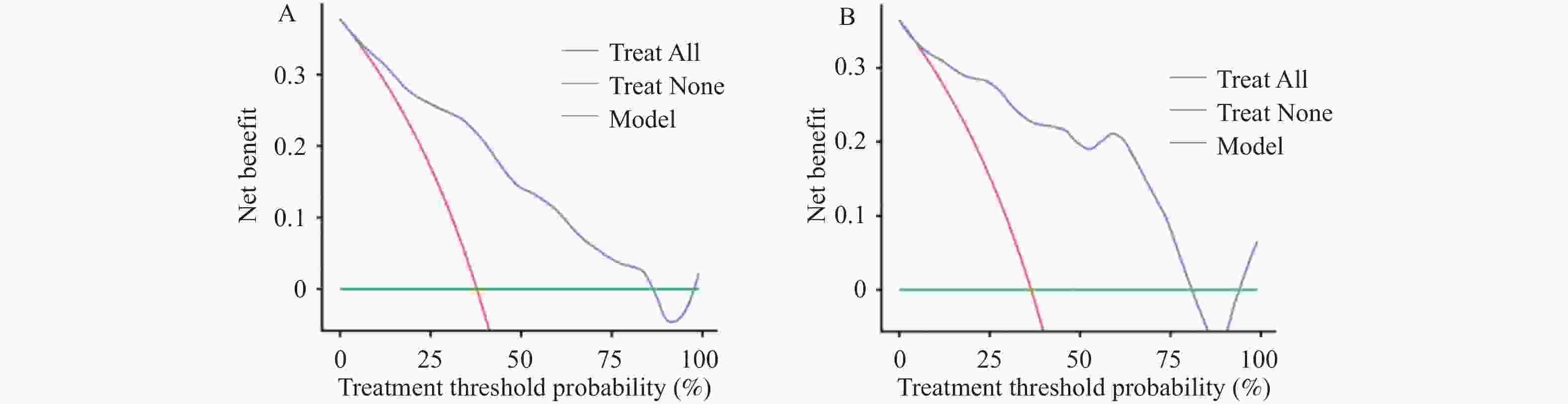
图 7 M1与M2预警模型在训练集中的DCA曲线
A:M1预警模型的DCA曲线;B:M2预警模型的DCA曲线。
Figure 7. DCA curves of M1 and M2 early warning models in the training set
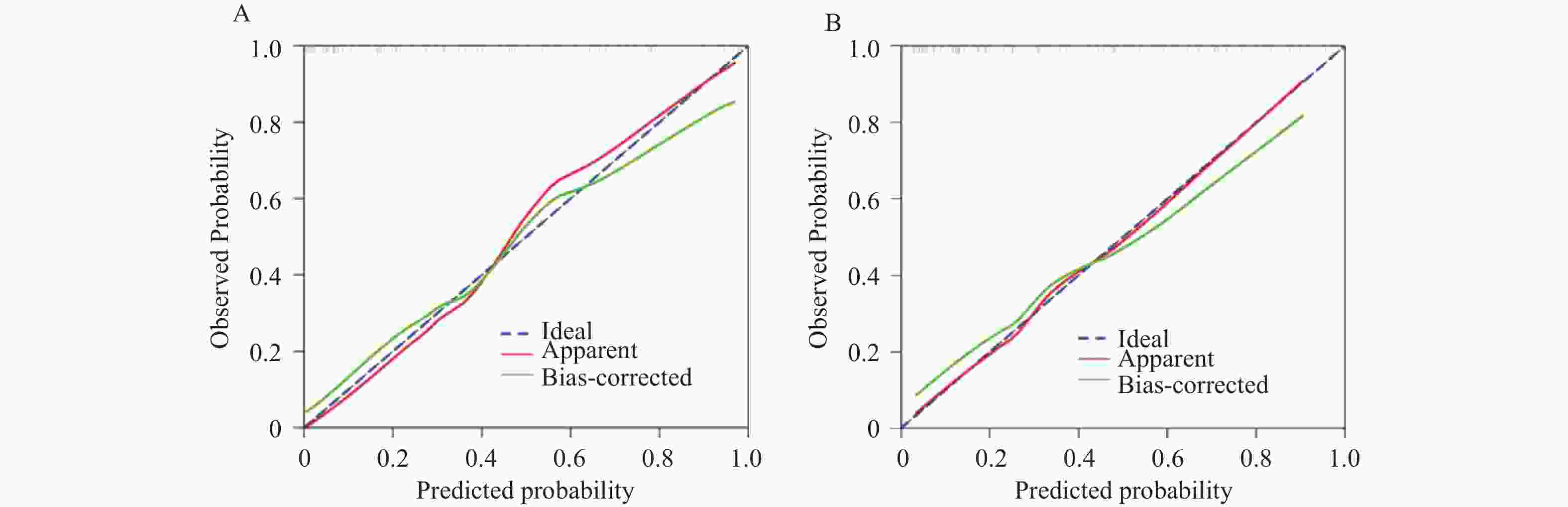
图 8 M1与M2预警模型在验证集中的校正曲线
A:M1预警模型的校正曲线;B:M2预警模型的校正曲线。
Figure 8. Adjustment curves of M1 and M2 early warning models in the validation set
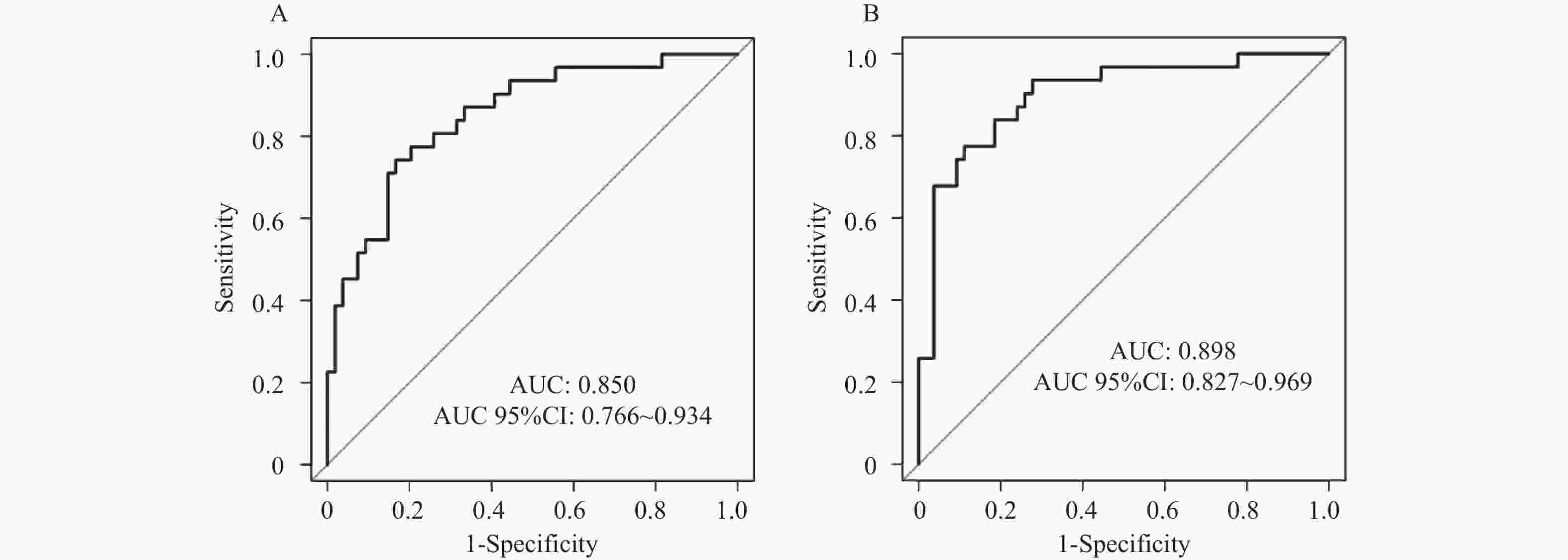
图 9 M1与M2预警模型在验证集中的ROC曲线
A:M1预警模型的ROC曲线;B:M2预警模型的ROC曲线。
Figure 9. ROC curves of M1 and M2 early warning models in the validation set
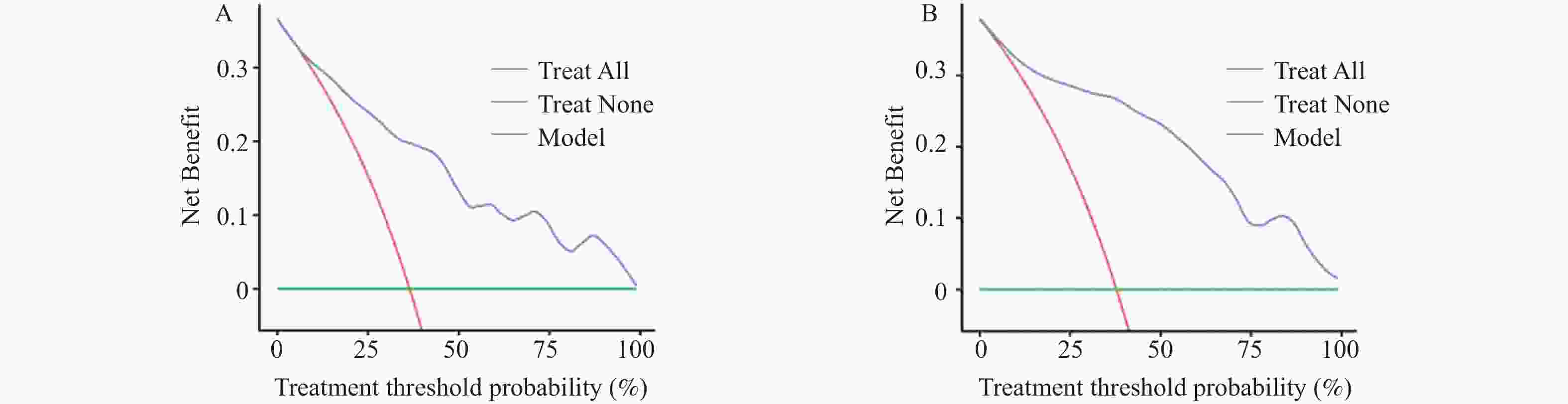
图 10 M1与M2预警模型在验证集中的DCA曲线
A:M1预警模型的DCA曲线;B:M2预警模型的DCA曲线。
Figure 10. DCA curves of M1 and M2 early warning models in the validation set
表 1 miR-140、miR-335-5p引物序列
Table 1. Primer sequences for miR-140 and miR-335-5p
指标 引物序列 miR-140 正向引物:5′-CCGCTAGTTGATGCAT-3′ 反向引物:5′-GCAGGGAGGTCTT-3′ miR-335-5p 正向引物:5′-AGCATGGACGTTCGTCTG-3′ 反向引物:5′-AACCACGGTTTGGTCCTTGG-3′ U6 正向引物:5′-CTCGCCTTAGTCGTCACCC-3′ 反向引物:5′-CGCCGAAGTTGCATTCCAG-3′  下载: 导出CSV
下载: 导出CSV
表 2 训练集与验证集的临床资料、血清miR-140、miR-335-5p比较[($ \bar x \pm s $)/n(%)]
Table 2. Comparison of clinical data,serum miR-140 and miR-335-5p between training set and validation set [($ \bar x \pm s $)/n(%)]
资料 训练集 验证集 UGIB组
(n = 76)非UGIB组
(n = 125)t/χ2/u P UGIB组
(n = 31)非UGIB组
(n = 54)t/χ2/u P 性别 0.095 0.758 0.041 0.841 男 47(61.84) 80(64.00) 20(64.52) 36(66.67) 女 29(38.16) 45(36.00) 11(35.48) 18(33.33) 年龄(岁) 52.61 ± 5.28 51.94 ± 5.47 0.853 0.395 51.62 ± 5.17 52.33 ± 5.50 0.585 0.560 BMI(kg/m2) 22.58 ± 1.42 22.39 ± 1.32 0.962 0.338 22.60 ± 1.29 22.35 ± 1.47 0.788 0.433 基础疾病 高血压 14(18.42) 20(16.00) 0.197 0.657 6(19.35) 9(16.67) 0.098 0.754 糖尿病 9(11.84) 14(11.20) 0.019 0.890 4(12.90) 5(9.26) 0.025 0.873 高脂血症 18(23.68) 32(25.60) 0.093 0.761 7(22.58) 10(18.52) 0.203 0.652 饮酒史 43(56.58) 38(30.40) 13.464 <0.001* 18(58.06) 16(29.63) 6.635 0.010* 肝硬化病程(年) 6.33 ± 1.57 6.06 ± 1.44 1.246 0.214 6.20 ± 1.63 6.17 ± 1.39 0.090 0.929 肝硬化病因 0.648 0.517 0.351 0.726 乙型肝炎肝硬化 42(55.26) 73(58.40) 18(58.06) 32(59.26) 酒精性肝硬化 21(27.63) 36(28.80) 9(29.03) 19(35.19) 丙型肝炎肝硬化 7(9.21) 11(8.80) 3(9.68) 2(3.70) 其他 6(7.89) 5(4.00) 1(3.23) 1(1.85) Child-Pugh分级 3.897 <0.001* 2.783 0.005* A级 13(17.11) 46(36.80) 4(12.90) 21(38.89) B级 25(32.89) 51(40.80) 12(38.71) 21(38.89) C级 38(50.00) 28(22.40) 15(48.39) 12(22.22) 食管静脉曲张程度 3.413 0.001* 2.548 0.011* 轻度 9(11.84) 39(31.20) 4(12.90) 19(35.19) 中度 24(31.58) 44(35.20) 11(35.48) 21(38.89) 重度 43(56.58) 42(33.60) 16(51.61) 14(25.93) 门静脉内径(cm) 1.51 ± 0.18 1.25 ± 0.12 12.281 <0.001* 1.50 ± 0.16 1.23 ± 0.11 9.195 <0.001* WBC(×109/L) 8.44 ± 0.85 8.50 ± 0.88 0.475 0.636 8.48 ± 0.91 8.53 ± 0.86 0.253 0.801 PLT(×109/L) 85.62 ± 12.74 87.49 ± 15.03 0.905 0.367 86.11 ± 13.16 89.02 ± 16.25 0.849 0.398 RDW(%) 15.82 ± 2.61 14.27 ± 1.35 5.538 <0.001* 15.91 ± 2.70 14.32 ± 1.56 3.448 0.001* Hb(g/L) 93.76 ± 15.23 108.85 ± 21.28 5.396 <0.001* 94.15 ± 17.14 109.20 ± 23.37 3.131 0.002* ALB(g/L) 29.15 ± 3.87 32.26 ± 3.31 6.054 <0.001* 29.27 ± 3.53 32.31 ± 3.30 3.986 <0.001* AST(U/L) 57.46 ± 10.02 51.92 ± 9.40 3.952 <0.001* 57.84 ± 10.28 52.08 ± 9.67 2.583 0.012* ALT(U/L) 45.38 ± 6.15 42.10 ± 5.73 3.827 <0.001* 45.42 ± 6.03 42.37 ± 5.59 2.353 0.021* GGT(U/L) 39.52 ± 8.27 33.08 ± 6.95 5.923 <0.001* 40.01 ± 8.84 33.46 ± 7.22 3.706 <0.001* TBiL(μmol/L) 26.65 ± 5.52 23.14 ± 4.17 5.108 <0.001* 26.80 ± 5.72 23.31 ± 4.25 3.205 0.002 miR-140 1.05 ± 0.12 1.16 ± 0.18 4.725 <0.001* 1.04 ± 0.11 1.14 ± 0.16 3.083 0.003* miR-335-5p 1.02 ± 0.10 1.13 ± 0.14 5.982 <0.001* 1.03 ± 0.10 1.12 ± 0.12 3.529 0.001* 用药史 非选择性β受体阻滞剂 45(59.21) 78(62.40) 0.203 0.653 19(61.29) 33(61.11) 0.000 0.987 质子泵抑制剂 58(76.32) 90(72.00) 0.453 0.501 24(77.42) 39(72.22) 0.277 0.599 他汀类药物 13(17.11) 22(17.60) 0.008 0.929 5(16.13) 9(16.67) 0.004 0.9749 *P < 0.05。
下载: 导出CSV
表 3 自变量赋值方法
Table 3. Independent variable assignment method
自变量 赋值方法 饮酒史 无=0,有=1 Child-Pugh分级 A级=1,B级=2,C级=3 食管静脉曲张程度 轻度=1,中度=2,重度=3 门静脉内径 连续变量,以实际值录入 RDW 连续变量,以实际值录入 AST 连续变量,以实际值录入 ALT 连续变量,以实际值录入 GGT 连续变量,以实际值录入 TBiL 连续变量,以实际值录入 Hb 连续变量,以实际值录入 ALB 连续变量,以实际值录入 miR-140 连续变量,以实际值录入 miR-335-5p 连续变量,以实际值录入
下载: 导出CSV
表 4 CPH并发UGIB的Logistic回归分析
Table 4. Logistic regression analysis of CPH complicated with UGIB
变量 β S.E. Waldχ2 P OR 95%CI Child-Pugh分级 A级 1.000 B级 1.201 0.350 11.732 0.001* 3.324 2.010~5.480 C级 1.370 0.320 18.289 <0.001* 3.935 2.458~6.301 食管静脉曲张程度 轻度 中度 1.033 0.281 13.415 <0.001* 2.810 1.726~4.582 重度 1.276 0.300 17.908 <0.001* 3.582 2.230~5.751 门静脉内径 0.462 0.120 14.610 <0.001* 1.587 1.270~1.960 RDW 0.434 0.111 15.524 <0.001* 1.544 1.259~1.890 Hb −0.859 0.180 22.784 <0.001* 0.424 0.318~0.565 miR-140 −0.978 0.192 26.012 <0.001* 0.376 0.280~0.505 miR-335-5p −0.927 0.185 25.016 <0.001* 0.396 0.298~0.526 常数项 −2.752 0.550 25.108 <0.001* − − *P < 0.05。
下载: 导出CSV
-
[1] Shung D L, Laine L. Review article: Upper gastrointestinal bleeding - review of current evidence and implications for management[J]. Aliment Pharmacol Ther, 2024, 59(9): 1062-1081. doi: 10.1111/apt.17949 [2] 谈理, 杨洪光, 郑波, 等. 肝硬化上消化道出血患者血清miR-130a表达情况及与病情严重程度和预后的相关性[J]. 临床误诊误治, 2021, 34(10): 88-93. doi: 10.3969/j.issn.1002-3429.2021.10.020 [3] Kumar M, Venishetty S, Jindal A, et al. Tranexamic acid in upper gastrointestinal bleed in patients with cirrhosis: A randomized controlled trial[J]. Hepatology, 2024, 80(2): 376-388. doi: 10.1097/HEP.0000000000000817 [4] Chen Y, Kong B B, Yin H, et al. Acute upper gastrointestinal bleeding due to portal hypertension in a patient with primary myelofibrosis: A case report[J]. World J Clin Cases, 2024, 12(15): 2621-2626. doi: 10.12998/wjcc.v12.i15.2621 [5] Cai L, Xu L, Shen K, et al. Sophorae tonkinensis Radix polysaccharide attenuates acetaminophen-induced liver injury by regulating the miR-140-5p-related antioxidant mechanism[J]. J Tradit Complement Med, 2024, 14(4): 467-476. doi: 10.1016/j.jtcme.2024.01.006 [6] Nie Y, Zhu X, Bu N, et al. Circ_0064288 acts as an oncogene of hepatocellular carcinoma cells by inhibiting miR-335-5p expression and promoting ROCK1 expression[J]. BMC Cancer, 2022, 22(1): 265. doi: 10.1186/s12885-022-09323-8 [7] 中华医学会肝病学分会. 肝硬化诊治指南[J]. 中华肝脏病杂志, 2019, 27(11): 846-865. doi: 10.3760/cma.j.cn501113-20250728-00298 [8] 北京医师协会门静脉高压专科医师分会, 中国研究型医院学会肝病专业委员会门静脉高压学组, 中国研究型医院学会肝病专业委员会. 肝硬化门静脉高压症多学科诊治(基于肝静脉压力梯度)专家共识[J]. 临床肝胆病杂志, 2021, 37(9): 2037-2044. doi: 10.3969/j.issn.1001-5256.2021.09.008 [9] 杨连粤, 白雪莉. 肝硬化门静脉高压症食管、胃底静脉曲张破裂出血诊治专家共识(2019版)[J]. 中国实用外科杂志, 2019, 39(12): 1241-1247. [10] Peng J, Jin H, Zhang N, et al. Development and evaluation of a predictive model of upper gastrointestinal bleeding in liver cirrhosis[J]. BMC Gastroenterol, 2025, 25(1): 142. doi: 10.1186/s12876-025-03677-6 [11] Oppong B, Amponsah G M, Gyabaah S, et al. Upper gastrointestinal endoscopic findings and their clinical correlates in patients with liver cirrhosis in northern Ghana[J]. Cureus, 2024, 16(8): e67725. doi: 10.7759/cureus.67725 [12] Wong R, Buckholz A, Hajifathalian K, et al. Liver severity score-based modeling to predict six-week mortality risk among hospitalized cirrhosis patients with upper gastrointestinal bleeding[J]. J Clin Exp Hepatol, 2024, 14(1): 101255. doi: 10.1016/j.jceh.2023.07.402 [13] 张春洋, 陈付群, 陈兆云. 老年肝硬化患者发生门脉高压性上消化道出血的危险因素分析及无创预测模型的建立[J]. 新疆医科大学学报, 2023, 46(12): 1623-1627, 1635. [14] Mousa N, Elbaz S, Elmetwalli A, et al. A risk stratification score for predicting first episode of upper gastrointestinal bleeding in patients with cirrhosis[J]. Arch Med Res, 2025, 56(7): 103253. doi: 10.1016/j.arcmed.2025.103253 [15] Prosty C, Noutsios D, Dubé L R, et al. Prophylactic antibiotics for upper gastrointestinal bleeding in patients with cirrhosis: A systematic review and Bayesian meta-analysis[J]. JAMA Intern Med, 2025, 185(10): e253832. doi: 10.1001/jamainternmed.2025.3832 [16] Metwally K, Essam T, Atwa A, et al. Helicobacter pylori versus platelet-to-spleen ratio as a risk factor for variceal bleeding in patients with liver-cirrhosis-related portal hypertension[J]. Am J Med Sci, 2022, 364(1): 23-28. doi: 10.1016/j.amjms.2021.10.018 [17] Yi M, Li Y, Wang D, et al. Correction to: KCNQ1OT1 exacerbates ischemia-reperfusion injury through targeted inhibition of miR-140-3P[J]. Inflammation, 2022, 45(2): 933-934. doi: 10.1007/s10753-022-01635-y [18] 何国富, 罗莉莉, 薛伟花. 乙型肝炎患者血清miR-129-5p、miR-335-5p水平变化及临床意义[J]. 转化医学杂志, 2024, 13(3): 417-420. doi: 10.3639/j.issn.2095-3097.2024.03.024 [19] Liu M, Liu X, Pan M, et al. Characterization and microRNA expression analysis of serum-derived extracellular vesicles in severe liver injury from chronic HBV infection[J]. Life, 2023, 13(2): 347. doi: 10.3390/life13020347 [20] Pan W, Wang Y, Zhao C. miR-140-5p attenuates hepatic fibrosis by directly targeting TGFβR1[J]. Scand J Gastroenterol, 2023, 58(11): 1335-1343. doi: 10.1080/00365521.2023.2223735 [21] López-Sánchez G N, Montalvo-Javé E, Domínguez-Perez M, et al. Hepatic mir-122-3p, mir-140-5p and mir-148b-5p expressions are correlated with cytokeratin-18 serum levels in MAFLD[J]. Ann Hepatol, 2022, 27(6): 100756. doi: 10.1016/j.aohep.2022.100756 [22] Yu Y Q, Li S Q, Weng J, et al. LncRNA H19 activates the RAS-MAPK signaling pathway via miR-140-5p/SOS1 axis in malignant liver tumors[J]. Curr Med Sci, 2024, 44(6): 1232-1240. doi: 10.1007/s11596-024-2949-0 [23] 张萍, 叶晓敏, 王云, 等. 肝硬化上消化道出血患者血清miR-210、miR-140水平与病情严重程度及预后的关系[J]. 临床检验杂志, 2023, 41(11): 844-849. [24] Liu Y, Kong X, Yu X, et al. Hepatitis B virus core/capsid protein induces hepatocellular carcinoma progression via long non-coding RNA KCNQ1OT1/miR-335-5p/CDC7 axis[J]. Transl Cancer Res, 2025, 14(6): 3319-3335. doi: 10.21037/tcr-2025-233 [25] 王玲, 曹信宇, 商伟芳, 等. 慢性乙型肝炎患者外泌体miR-335-5p与肝硬化严重程度的相关性[J]. 中国热带医学, 2024, 24(3): 326-332. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 197
- HTML全文浏览量: 109
- PDF下载量: 109
- 被引次数: 0
