

Evaluation and Clinical Analysis of Extubation Related Indicators in Patients with Brain Injury Undergoing Tracheotomy
-
摘要:
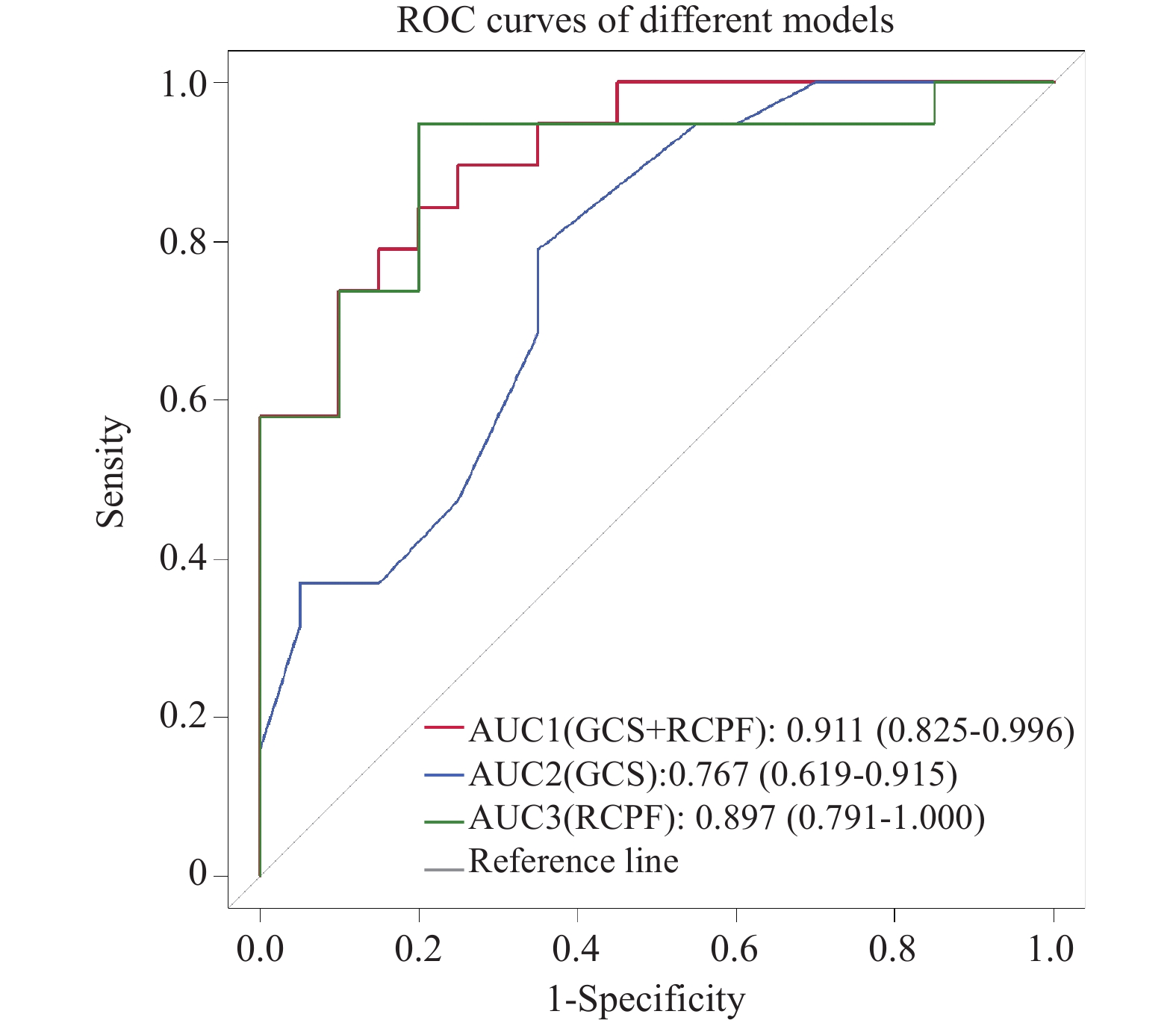
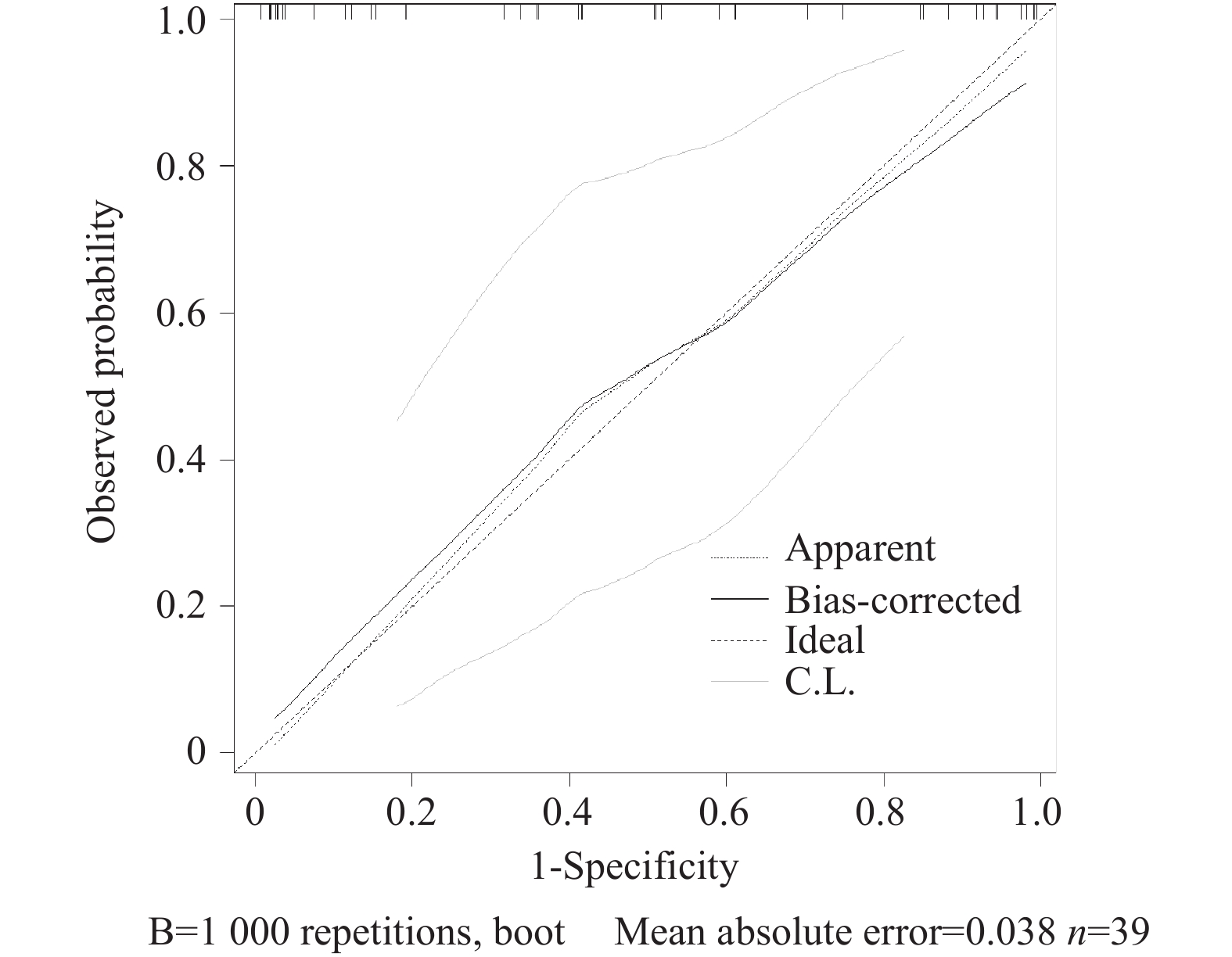
目的 探讨膈肌超声、反射性咳嗽峰流速(reflex cough peak flow,RCPF)、拉斯哥昏迷评分(glasgow coma scale,GCS)在脑损伤气管切开术后患者拔管评估中的应用价值。 方法 回顾性分析昆明医科大学第二附属医院康复医学中心2024年8月至2025年10月收治的39例脑损伤气管切开术后患者,按住院期间拔管情况分为拔管成功组(19例)和拔管未成功组(20例)。收集患者的一般临床资料、膈肌超声、RCPF、GCS、白介素6(interleukin-6,IL-6)等指标,检测均于拔管前24 h内完成。采用单因素分析、逐步法二元Logistic回归及ROC曲线进行探索性统计分析。 结果 拔管成功组的膈肌增厚分数(diaphragm thickening fraction,DTF)、膈肌移动度(diaphragmatic excursion,DE)、RCPF、GCS显著高于拔管未成功组(P < 0.05);两组吸气末膈肌厚度(diaphragm thickness at end inspiration,DTei)、IL-6比较差异无统计学意义(P > 0.05)。Logistic回归显示,RCPF、GCS评分与拔管结局相关(P < 0.05);二者联合评估AUC达0.911,其检测敏感度为89.50%、特异度为75.00%;模型拟合及验证效果良好。 结论 DTF、DE、RCPF、GCS均与拔管情况相关,其中RCPF与GCS联合评估效能较好。 Abstract:Objective To investigate the application value of diaphragmatic ultrasound, reflex cough peak flow (RCPF) and Glasgow Coma Scale (GCS) in extubation evaluation of patients with brain injury after tracheotomy. Methods A retrospective analysis was performed on 39 patients with brain injury after tracheotomy admitted to the Rehabilitation Medicine Center of The Second Affiliated Hospital of Kunming Medical University from August 2024 to October 2025. The patients were divided into successful extubation group (19 cases) and a failed extubation group (20 cases) according to extubation outcomes during hospitalization. General clinical data, diaphragm ultrasound parameters, RCPF, GCS and interleukin-6 (IL-6) were collected and all examinations were completed within 24 hours before extubation. Exploratory statistical analyses were conducted using univariate analysis, stepwise binary Logistic regression, and receiver operating characteristic (ROC) curve. Results The diaphragm thickening fraction (DTF), diaphragm excursion (DE), RCPF, and GCS in the successful extubation group were significantly higher than those in the failed extubation group (P < 0.05). There were no significant differences in diaphragm thickness at end inspiration (DTei) or IL-6 between the two groups (P > 0.05). Logistic regression showed that RCPF and GCS were correlated with extubation outcomes (P < 0.05). The area under the ROC curve (AUC) of combined evaluation of the two indicators was 0.911, with a sensitivity of 89.50% and a specificity of 75.00%, indicating satisfactory model fitting and validation performance. Conclusion This study demonstrates that DTF, DE, RCPF, and GCS score are all associated with extubation outcomes, among which the combined evaluation of RCPF and GCS score presents favorable predictive efficacy. -
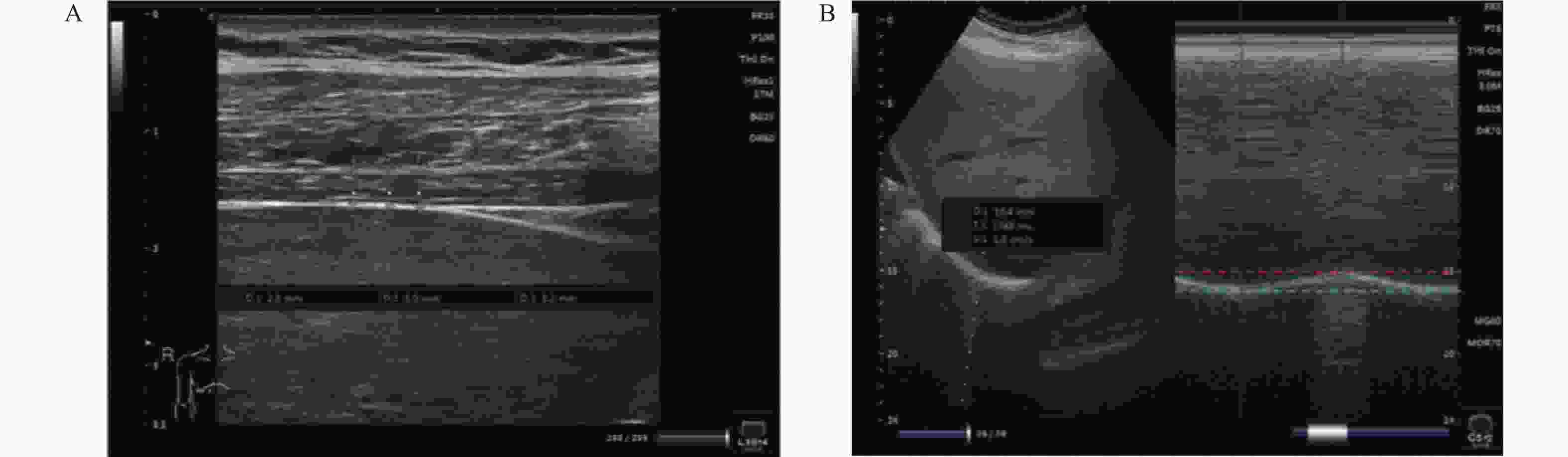
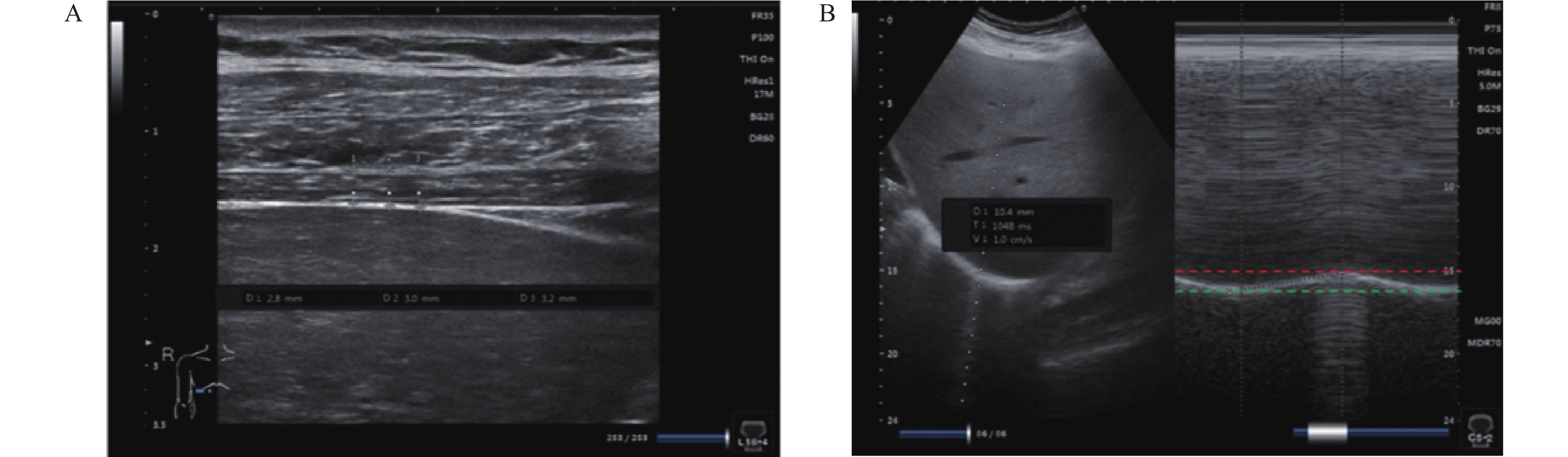
图 1 膈肌超声测量图
A:平静呼吸时膈肌厚度的测量方式;B:平静呼吸时膈肌移动度测量方式。
Figure 1. Diaphragm ultrasound measurement
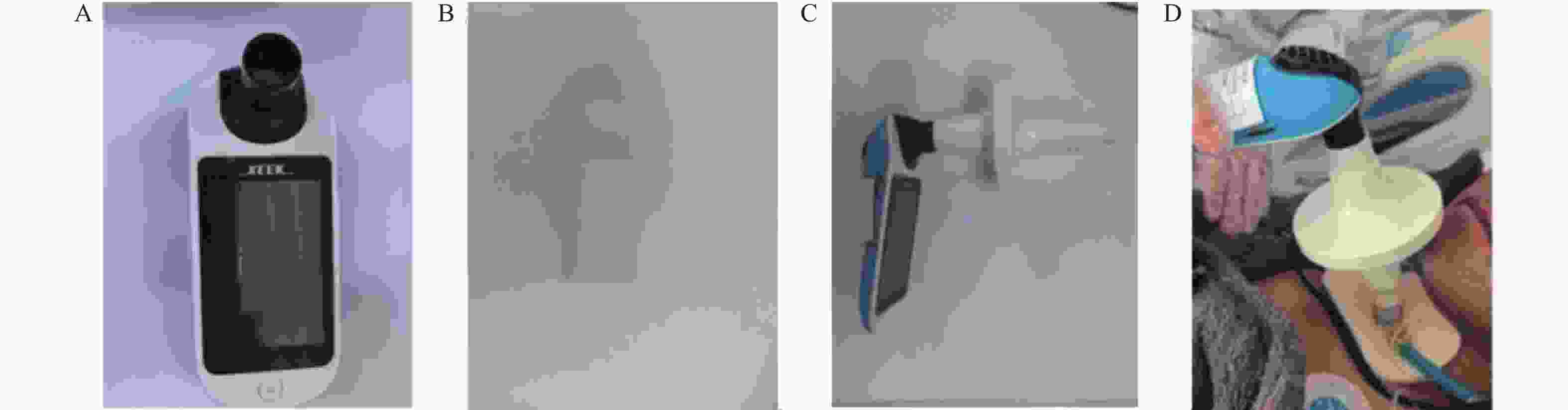
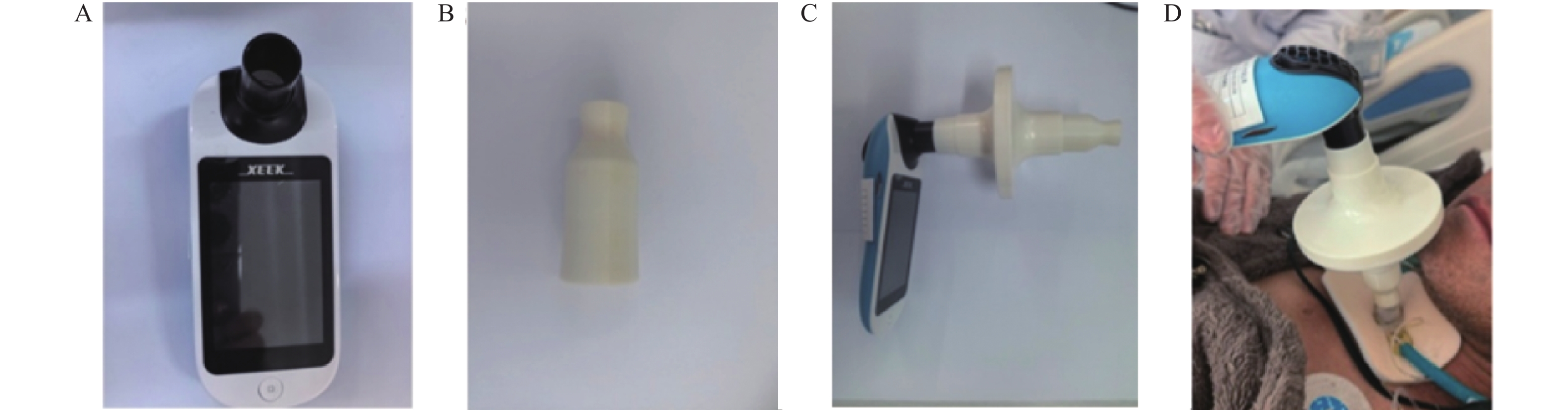
图 2 反射性咳嗽峰流速的测量图
A:赛克便携式肺功能仪(型号:X1);B:3D打印的转接头;C:连接方式;D:RCPF的测量方式。
Figure 2. Measurement of reflex cough peak flow
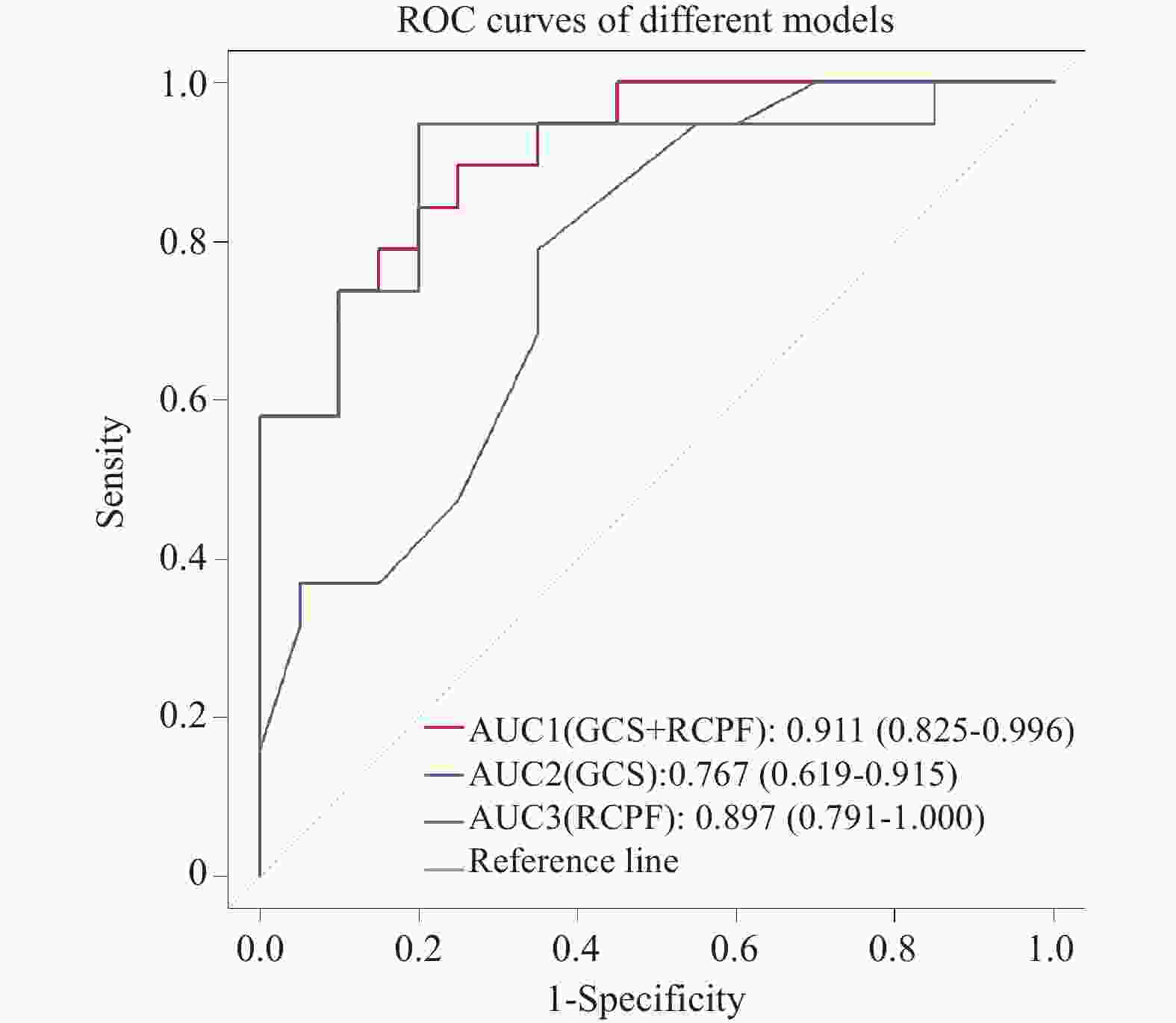
图 3 脑损伤患者气管套管拔除预测模型的ROC曲线
Figure 3. ROC curve of the predictive model for extubation in patients with brain injury
表 1 拔管成功组与拔管未成功组一般资料比较[$ \bar x \pm s $/n(%)/M(P25,P75)]
Table 1. Comparison of general data between successful extubation group and unsuccessful extubation group [$ \bar x \pm s $/n(%)/M(P25,P75)]
指标 拔管成功组(n = 19) 拔管未成功组(n = 20) t/z/χ2 P 年龄(岁) 52.84 ± 14.435 59.30 ± 7.665 1.758 0.087 性别 0.067 男 10(47.37) 16(80.00) 女 9(52.63) 4(20.00) 偏瘫侧 0.892 左偏瘫 6(31.58) 5(25.00) 右侧偏瘫 4(21.05) 5(25.00) 四肢瘫 9(47.37) 10(50.00) 脑损伤类型 0.521 脑卒中 15(78.95) 14(70.00) 脑外伤 4(21.05) 6(30.00) BMI (kg/m2) 22.62 ± 4.22 23.81 ± 3.36 0.977 0.335 性别、偏瘫侧、脑损伤类型比较采用Fisher确切概率法,P < 0.05为差异有统计学意义。  下载: 导出CSV
下载: 导出CSV
表 2 拔管成功组与拔管未成功组膈肌超声结果比较($ \bar x \pm s $)
Table 2. Comparison of diaphragmatic ultrasound results between successful extubation group and unsuccessful extubation group ($ \bar x \pm s $)
组别 DTei(mm) DTF(%) DE(mm) 拔管成功组(n = 19) 2.20 ± 0.50 20.33 ± 9.00 13.88 ± 7.63 拔管未成功组(n = 20) 1.94 ± 0.25 12.77 ± 9.08 7.65 ± 3.51 t −2.026 −2.611 −3.250 P 0.053 0.013* 0.003* *P < 0.05。
下载: 导出CSV
表 3 拔管成功组与拔管未成功组反射性咳嗽峰流速结果比较[M(P25,P75)]
Table 3. Comparison of reflex cough peak flow between successful extubation group and unsuccessful extubation group [M(P25,P75)]
指标 拔管成功组(n = 19) 拔管未成功组(n = 20) Z P RCPF(L/min) 150.33(125.67,174.00) 95.17(61.25,108.75) −4.243 <0.001* *P < 0.05。
下载: 导出CSV
表 4 拔管成功组与拔管未成功组其他相关评估指标比较[($ \bar x \pm s $)/M(P25,P75)]
Table 4. Comparison of other relevant assessment indicators between successful extubation group and unsuccessful extubation group group[($ \bar x \pm s $)/M(P25,P75)]
指标 拔管成功组(n = 19) 拔管未成功组(n = 20) t/z P GCS(分) 11.05 ± 2.82 7.80 ± 3.17 −3.78 0.002* IL-6(pg/mL) 9.08(5.56,18.26) 22.37(6.98,34.71) −1.50 0.13 *P < 0.05。
下载: 导出CSV
表 5 成功拔除气管套管的logistic回归分析
Table 5. Logistic regression analysis of successful extubation
参数 β SE waldχ2 P OR(95%CI) RCPF(L/min) 0.049 0.021 5.589 0.018* 1.050(1.008,1.093) GCS(分) 0.487 0.226 4.643 0.031* 1.628(1.045,2.535) DE(mm) 0.268 0.165 2.643 0.104 1.308(0.946,1.808) 常量 −12.897 4.887 6.965 *P < 0.05为差异有统计学意义。
下载: 导出CSV
-
[1] Pillai I N, Chandini N C, Joseph S, et al. Decannulation patterns and predictors in acquired brain injury: a retrospective study[J]. Int J Rehabil Res, 2025, 48(3): 143-148. doi: 10.1097/MRR.0000000000000675 [2] Li Y, Wang S S, Li K Y, et al. Application of bedside ultrasound assessment of diaphragmatic function in preparing tracheostomised patients for ventilator liberation and decannulation: a narrative review[J]. J Thorac Dis, 2026, 18(3): 246. doi: 10.21037/jtd-2025-1-2737 [3] Erickson E L, Katta J, Sun S, et al. Retrospective review of acute post-tracheostomy complications and contributing risk factors[J]. Clin Otolaryngology, 2024, 49(2): 277-282. doi: 10.1111/coa.14131 [4] Wu H, Wang H, Yang X, et al. Multistage investigation of predictive factors for tracheostomy in brain injury: a bibliometric, descriptive, and retrospective analysis[J]. Front Neurol, 2025, 16: 1648046. doi: 10.3389/fneur.2025.1648046 [5] 周叶子, 张阳普, 张伟, 等. 膈肌超声在脑卒中患者气管套管拔除中应用的临床观察[J]. 中国康复, 2024, 39(8): 494-497. [6] Al-Husinat L, Araydah M, Haddad F, et al. Ventilator weaning and extubation in acute brain injury: Challenges and evidence-based approaches [J]. Anaesth Crit Care Pain Med, 2026: 101816. [7] 赵蕾, 关晨霞, 闫莹莹, 等. 重度获得性脑损伤气管切开患者拔管影响因素的研究进展[J]. 中国康复, 2023, 38(9): 563-567. [8] Duan J, Zhang X, Song J. Predictive power of extubation failure diagnosed by cough strength: a systematic review and meta-analysis[J]. Crit Care, 2021, 25(1): 357. doi: 10.1186/s13054-021-03781-5 [9] 李秋怡. 气管切开患者拔管的临床预测模型构建与验证 [D]. 昆明: 昆明医科大学, 2023. [10] 《成人气管切开拔管中国专家共识》编写组, 中华医学会物理医学与康复学分会心肺康复学组, 中国康复医学会重症康复专业委员会. 成人气管切开拔管中国专家共识(下)[J]. 中华物理医学与康复杂志, 2023, 45(7): 577-584. [11] 李勍, 姜宏英, 周婷, 等. 气管切开术后拔管困难患者成功拔除气切套管的相关因素分析[J]. 中国康复医学杂志, 2023, 38(9): 1227-1232. [12] Zhou T, Wang J, Zhang C, et al. Tracheostomy decannulation protocol in patients with prolonged tracheostomy referred to a rehabilitation hospital: A prospective cohort study[J]. J Intensive Care, 2022, 10(1): 34. doi: 10.1186/s40560-022-00626-3 [13] Chen Z H, Wu H T, Yao Z, et al. Using ML techniques to predict extubation outcomes for patients with central nervous system injuries in the Yun-Gui Plateau[J]. Sci Rep, 2025, 15(1): 17773. [14] Dubé B P, Dres M, Mayaux J, et al. Ultrasound evaluation of diaphragm function in mechanically ventilated patients: comparison to phrenic stimulation and prognostic implications[J]. Thorax, 2017, 72(9): 811-818. [15] Elsayed A A, Mousa R M, Beshey B N. Impact of early versus late tracheotomy on diaphragmatic function assessed by ultrasonography in mechanically ventilated stroke patients[J]. Egypt J Anaesth, 2022, 38(1): 229-235. [16] Zhou Q, Xu Y, Chen J, et al. Prediction of weaning outcomes from mechanical ventilation in critically ill patients based on the combination of ultrasound parameters of the heart, lung, and diaphragm: A prospective observational cohort study[J]. Quant Imaging Med Surg, 2025, 15(9): 7697-7710. [17] 王娜, 舒琪, 贺娟, 等. 膈肌超声在支气管肺发育不良患儿撤机中的应用[J]. 分子影像学杂志, 2023, 46(06): 1107-11 [18] Marques M R, Pereira J M, Paiva J A, et al. Ultrasonography to access diaphragm dysfunction and predict the success of mechanical ventilation weaning in critical care: A narrative review[J]. J Ultras Med, 2024, 43(2): 223-236. [19] Le Neindre A, Philippart F, Luperto M, et al. Diagnostic accuracy of diaphragm ultrasound to predict weaning outcome: A systematic review and meta-analysis[J]. Int J Nurs Stud, 2021, 117: 103890. [20] Liu X, Yang Y, Jia J. Respiratory muscle ultrasonography evaluation and its clinical application in stroke patients: A review[J]. Front Neurosci, 2023, 17: 1132335. [21] 高敏. 反射性咳嗽峰流速对创伤性颅脑损伤患者气管拔管的预测价值 [D]. 长沙: 湖南师范大学, 2022. [22] Wei Y. Predictive Value of diaphragmatic thickening fraction combined with cough peak flow rate for weaning from mechanical ventilation[J]. J Clin Nurs Res, 2025, 9(3): 241-247. [23] Brennan M, Mcdonnell M J, Duignan n, et al. The use of cough peak flow in the assessment of respiratory function in clinical practice- A narrative literature review[J]. Resp Med, 2022, 193: 106740. [24] Blackwell V K, Van G J J, Prescott S L. The airway-brain axis: Connecting breath, brain, and behavior[J]. Cell Rep, 2025, 44(9): 116239. [25] Christiansen K J, Devantier L, Pasgaard T, et al. Tracheostomy healing time after decannulation[J]. Multidiscip Resp Med, 2022, 16(1): 822. [26] 杨玲, 安磊, 俞芃, 等. 重型急性脑卒中患者气管套管拔出困难因素分析[J]. 中国医药科学, 2021, 11(6): 8-12. [27] Chen Y, Aishan G, Fan S, et al. Predictors of long-term decannulation in patients with disorders of consciousness[J]. Front Neurol, 2023, 14: 1099307. [28] Brennan P M, Whittingham C, Sinha V D, et al. Assessment of level of consciousness using Glasgow Coma Scale tools[J]. BMJ, 2024, 384: e077538. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 191
- HTML全文浏览量: 148
- PDF下载量: 54
- 被引次数: 0
