

Predictive Value of MDSCs,B7-H2 and Treg/Th17 Levels for Therapeutic Efficacy in Patients with Primary Immune Thrombocytopenia
-
摘要:
目的 探究原发免疫性血小板减少症(immune thrombocytopenia,ITP)患者髓源性抑制性细胞(myeloid-derived suppressor cells,MDSCs)、可诱导共刺激分子配体(B7 Homolog 2,B7-H2)与调节性T细胞(regulatory T cell,Treg)/辅助性T细胞17(T helper 17 cell,Th17)免疫失衡的相关性,并分析其对疗效的预测价值。 方法 选取2020年1月至2025年1月株洲市中心医院收治的191例ITP患者(ITP组,建模集)进行前瞻性研究,按照1∶1另选同期191例健康体检者作为对照组。比较两组MDSCs、B7-H2、Treg/Th17、骨髓巨核细胞形态及血小板相关抗体血小板相关免疫球蛋白G(platelet-associated Immunoglobulin G,PAIgG)、血小板相关免疫球蛋白A(platelet-associated Immunoglobulin A,PAIgA)、血小板相关免疫球蛋白M(platelet-associated Immunoglobulin M,PAIgM)。分析MDSCs、B7-H2、Treg/Th17对ITP疗效的影响,并分析其对疗效的预测价值。另选取2025年1月至2025年12月52例ITP患者作为独立外部验证集,对MDSCs、B7-H2联合Treg/Th17预测价值进行验证。 结果 ITP组MDSCs、Treg、Treg/Th17低于对照组,B7-H2、Th17高于对照组(P < 0.05);总有效亚组治疗后MDSCs、Treg/Th17高于无效亚组,B7-H2低于无效亚组(P < 0.05);治疗前MDSCs、B7-H2、Treg/Th17均是ITP疗效的相关影响因素(P < 0.05);治疗前MDSCs、Treg/Th17与疗效呈正相关(P趋势 < 0.05,P非线性>0.05),B7-H2与疗效呈负相关(P趋势 < 0.05,P非线性 > 0.05);联合的AUC值(0.898)显著大于单独的MDSCs(0.764)、B7-H2(0.739)、Treg/Th17(0.761)。验证集中,联合预测模型在验证队列中的AUC与研究队列接近。Pearson相关性分析显示,颗粒型巨核细胞与 MDSCs、Treg/Th17呈负相关,与B7-H2呈正相关(P < 0.001);产板型巨核细胞与MDSCs、Treg/Th17呈正相关,与B7-H2呈负相关(P < 0.001);PAIgG、PAIgA、PAIgM均与MDSCs、Treg/Th17呈负相关,与B7-H2呈正相关(P < 0.001)。 结论 ITP患者MDSCs、B7-H2与Treg/Th17密切相关,这些指标的检测对疗效具有预测价值,联合分析可提高预测效能。 -
关键词:
- 原发免疫性血小板减少症 /
- 髓源性抑制性细胞 /
- 可诱导共刺激分子配体 /
- 调节性T细胞 /
- 辅助性T细胞17 /
- 预测价值
Abstract:Objective To investigate the correlation between myeloid-derived suppressor cells (MDSCs), B7 Homolog 2 (B7-H2), and regulatory T cell (Treg)/T helper 17 cell (Th17) immune imbalance in patients with primary immune thrombocytopenia (ITP), and to analyze their predictive value for therapeutic efficacy. Methods A total of 191 ITP patients (ITP group, modeling set) admitted to Zhuzhou Central Hospital from January 2020 to January 2025 were selected for prospective study, and another 191 healthy in the same period were selected in a 1:1 ratio as the control group. MDSCs, B7-H2, Treg/Th17, bone marrow megakaryocyte morphology and platelet-associated antibodies [platelet-associated Immunoglobulin G (PAIgG), platelet-associated Immunoglobulin A (PAIgA), platelet-associated Immunoglobulin M (PAIgM)] were compared between the two groups. The effects of MDSCs, B7-H2 and Treg/Th17 on ITP treatment efficacy and their predictive value were analyzed. In addition, another 52 ITP patients from January 2025 to December 2025 were selected as independent external validation set to validate the combined predictive value of MDSCs, B7-H2, and Treg/Th17. Results The ITP group showed lower MDSCs, Treg, and Treg/Th17 ratio, and higher B7-H2 and Th17 levels compared to the control group (P < 0.05). After treatment, the effective subgroup had higher MDSCs and Treg/Th17 ratio, and lower B7-H2 than the ineffective subgroup (P < 0.05). Before treatment, MDSCs, B7-H2, and Treg/Th17 ratio were all related factors affecting the efficacy of ITP treatment (P < 0.05). Before treatment, MDSCs and Treg/Th17 showed a positive correlation with efficacy (Ptrend <0.05, Pnonlinea>0.05), while B7-H2 showed a negative correlation with efficacy (Ptrend < 0.05, Pnonlinea>0.05). The combined AUC value (0.898) was significantly greater than that of MDSCs alone (0.764), B7-H2 alone (0.739), and Treg/Th17 alone (0.761). In the validation set, the AUC of the combined prediction model was similar to that in the training set. Pearson correlation analysis showed that granular megakaryocytes were negatively correlated with MDSCs and Treg/Th17, and positively correlated with B7-H2 (P < 0.001). Plate-forming megakaryocytes were positively correlated with MDSCs and Treg/Th17, and negatively correlated with B7-H2 (P < 0.001). PAIgG, PAIgA and PAIgM were negatively correlated with MDSCs and Treg/Th17, and positively correlated with B7-H2 (P < 0.001). Conclusion MDSCs and b7-h2 in ITP patients are closely related to Treg/Th17. The detection of these indicators has predictive value for curative effect, and combined analysis can improve the predictive efficiency. -
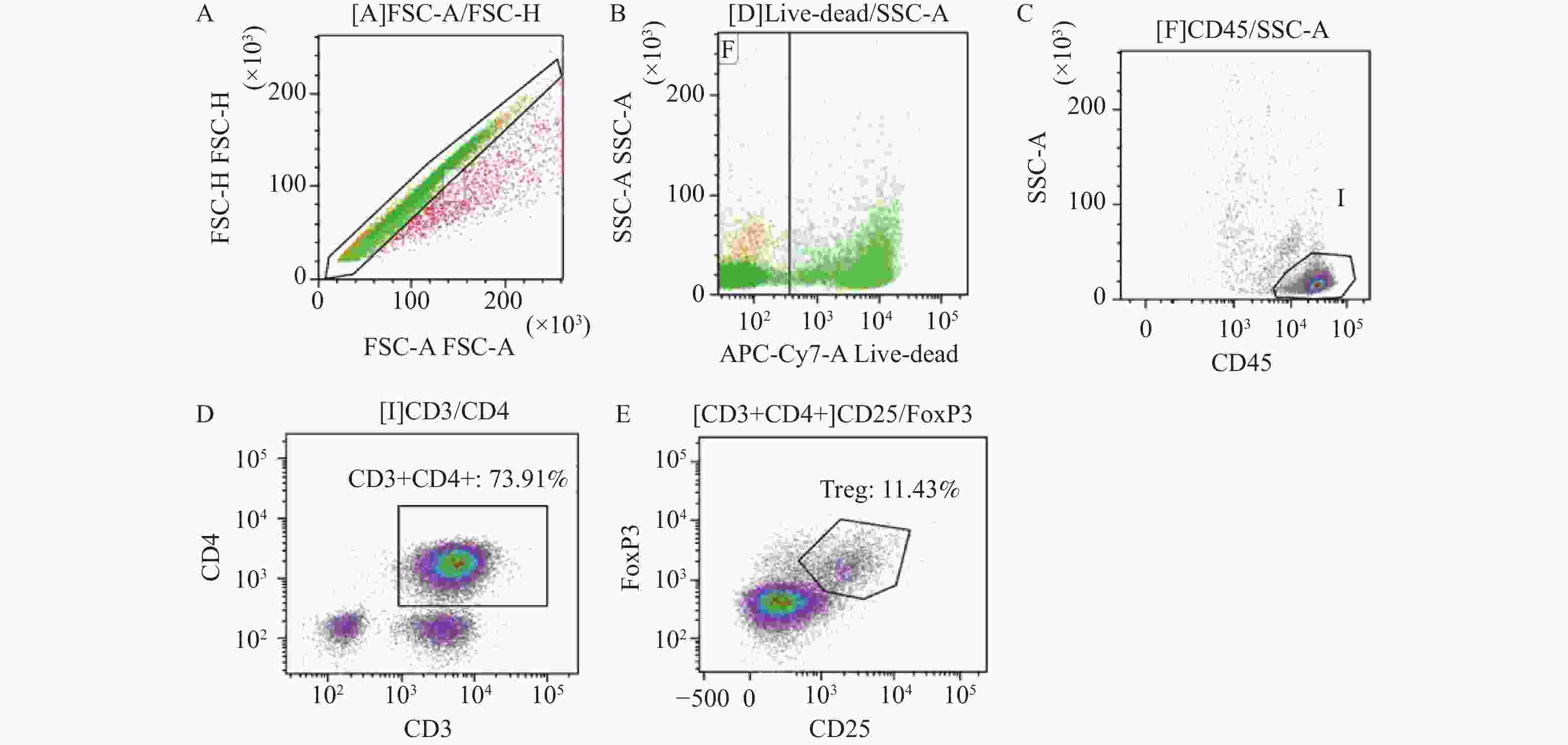
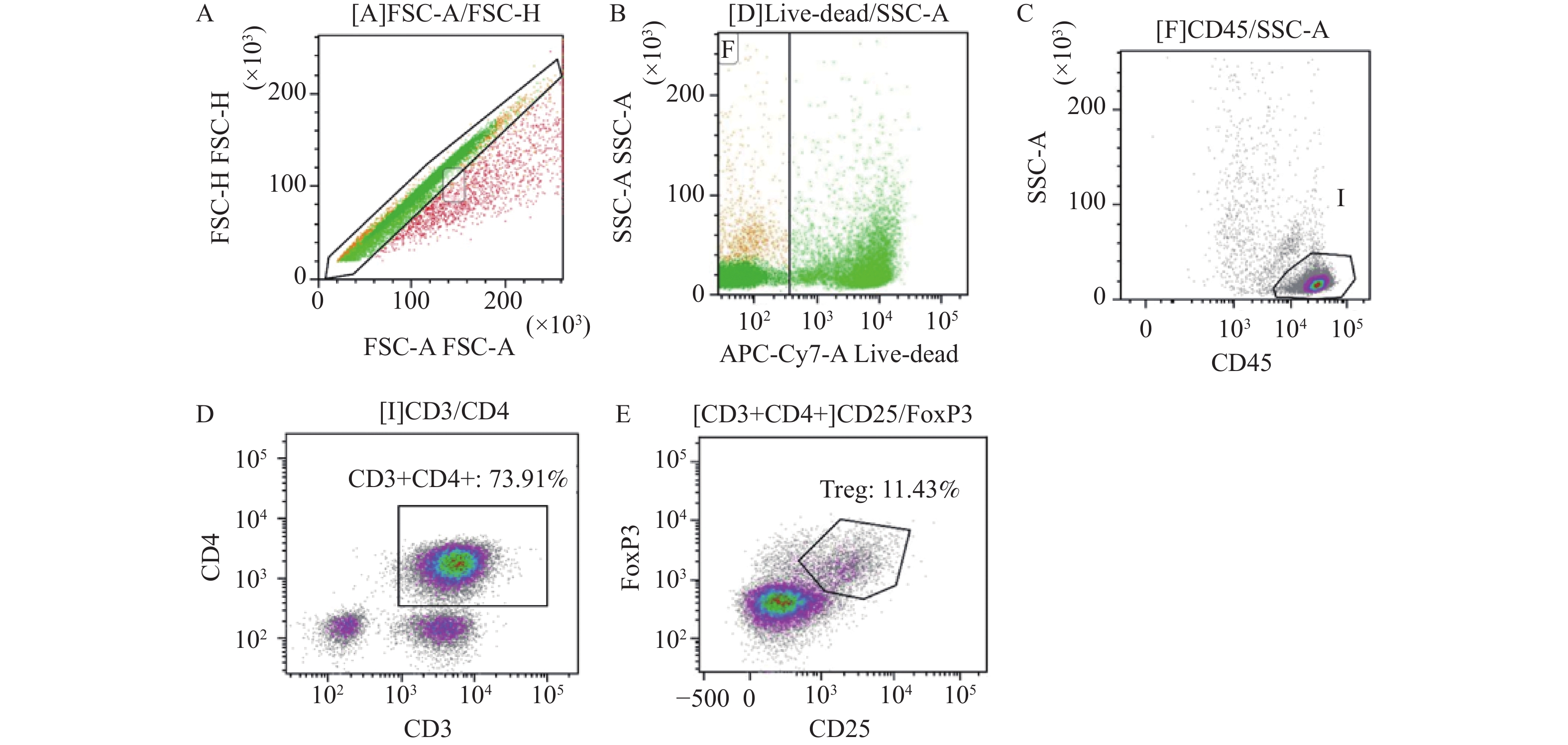
图 1 两组Treg(CD4+CD25+Foxp3+)流式细胞分析图
A:有核细胞散点图;B:活细胞门;C:显示所有有核细胞;D:显示有核细胞门并圈中CD3+CD4细胞;E:显示所有CD3+CD4细胞,圈中CD25+FoxP3为Treg细胞。
Figure 1. Flow cytometric analysis of Treg in the two groups (CD4+CD25+Foxp3+)
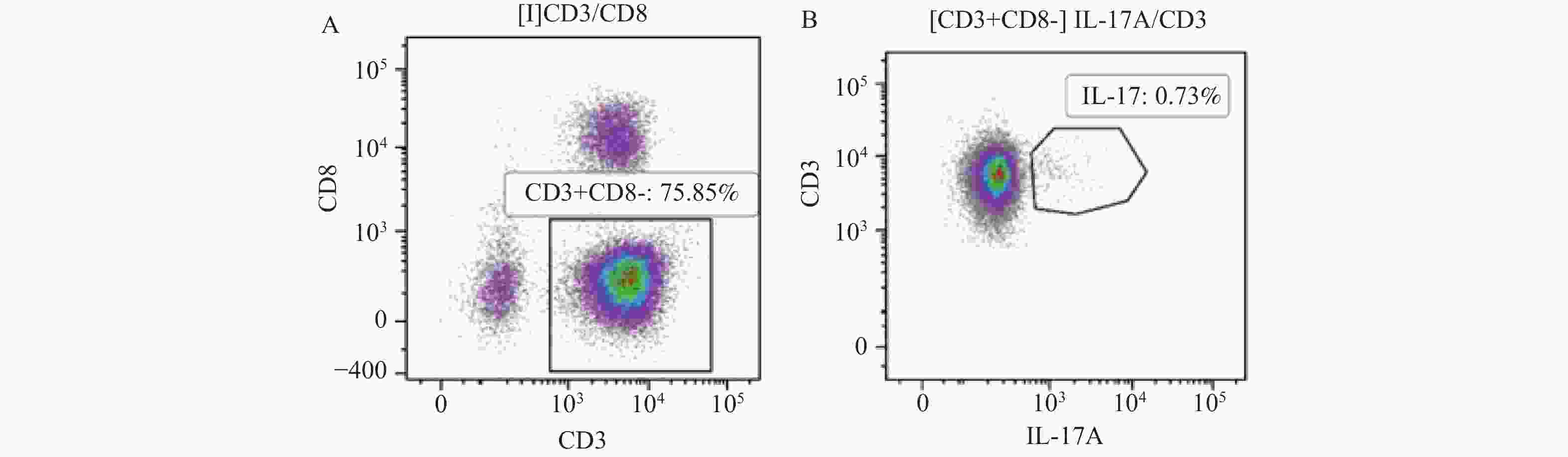
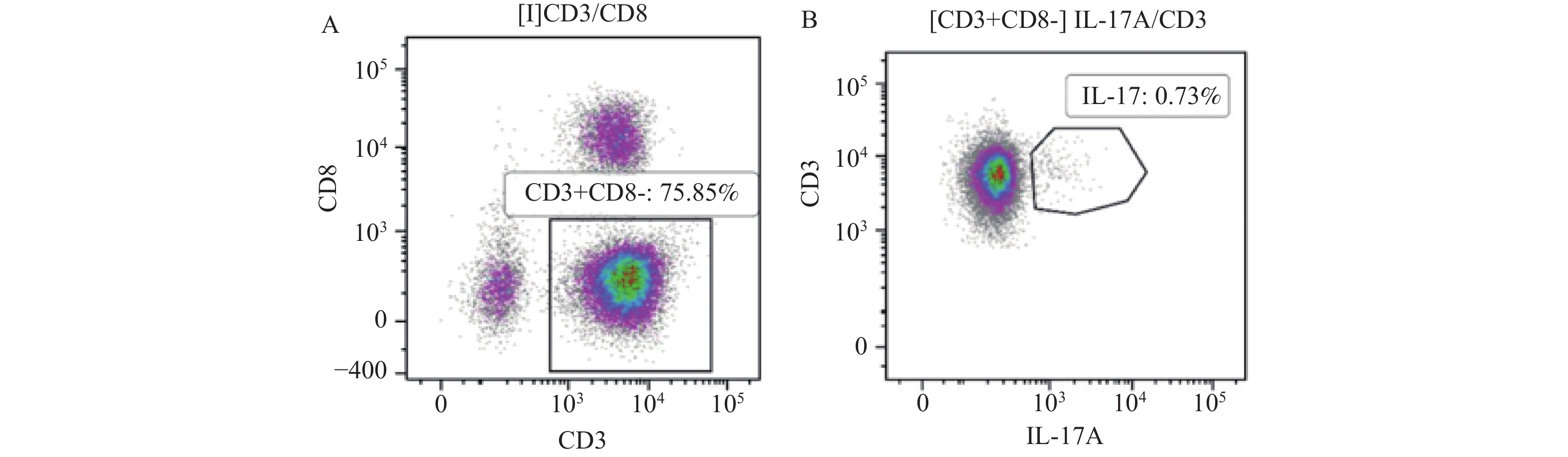
图 2 两组Th17(CD3+CD8-IL-17+)流式细胞分析图
A:显示有核细胞门并圈中CD3+CD8-细胞;B:显示所有CD3+CD8-细胞,IL-17A+为1L-17阳性细胞。
Figure 2. Flow cytometric analysis of Th17 (CD3+CD8-IL-17+) in the two groups
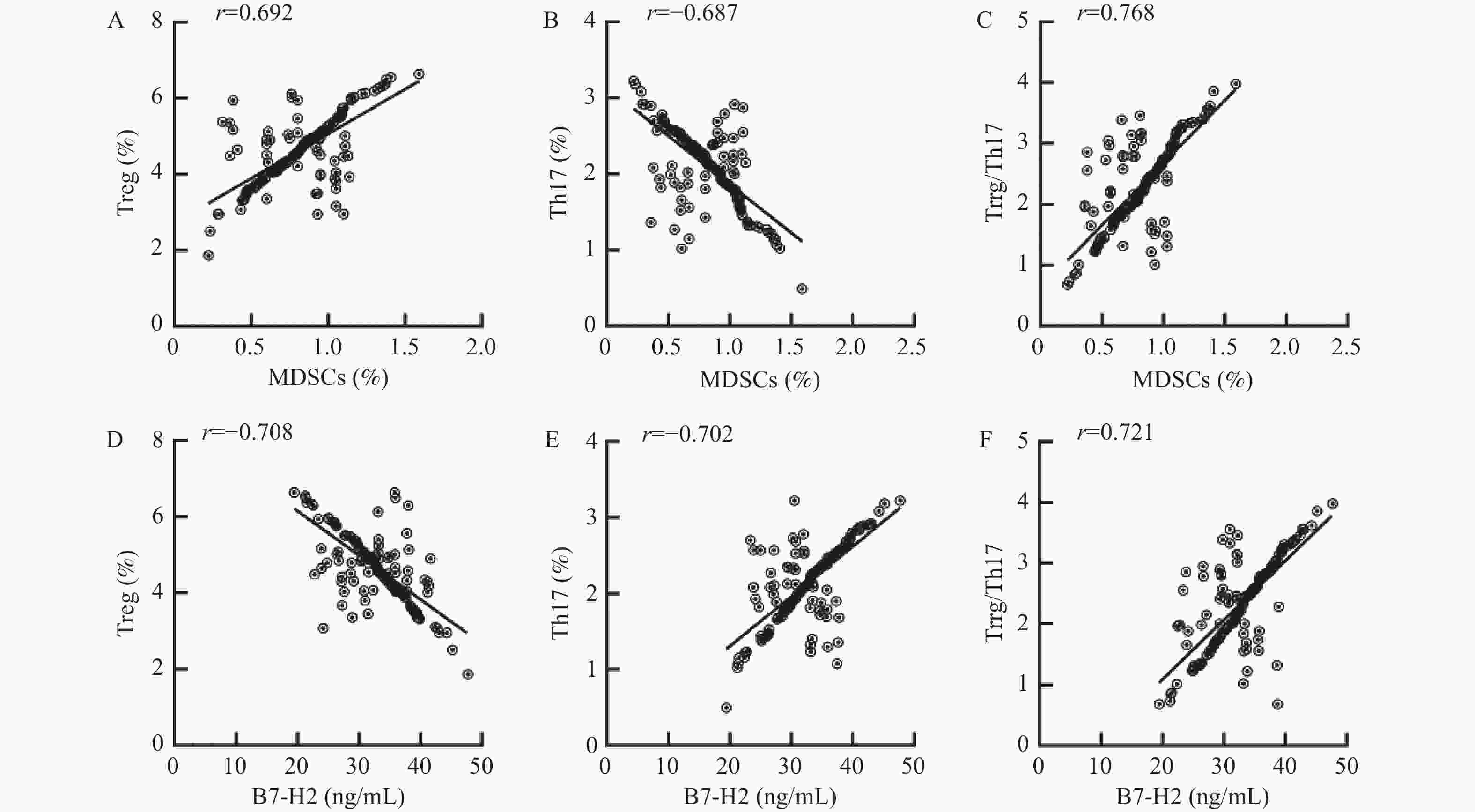
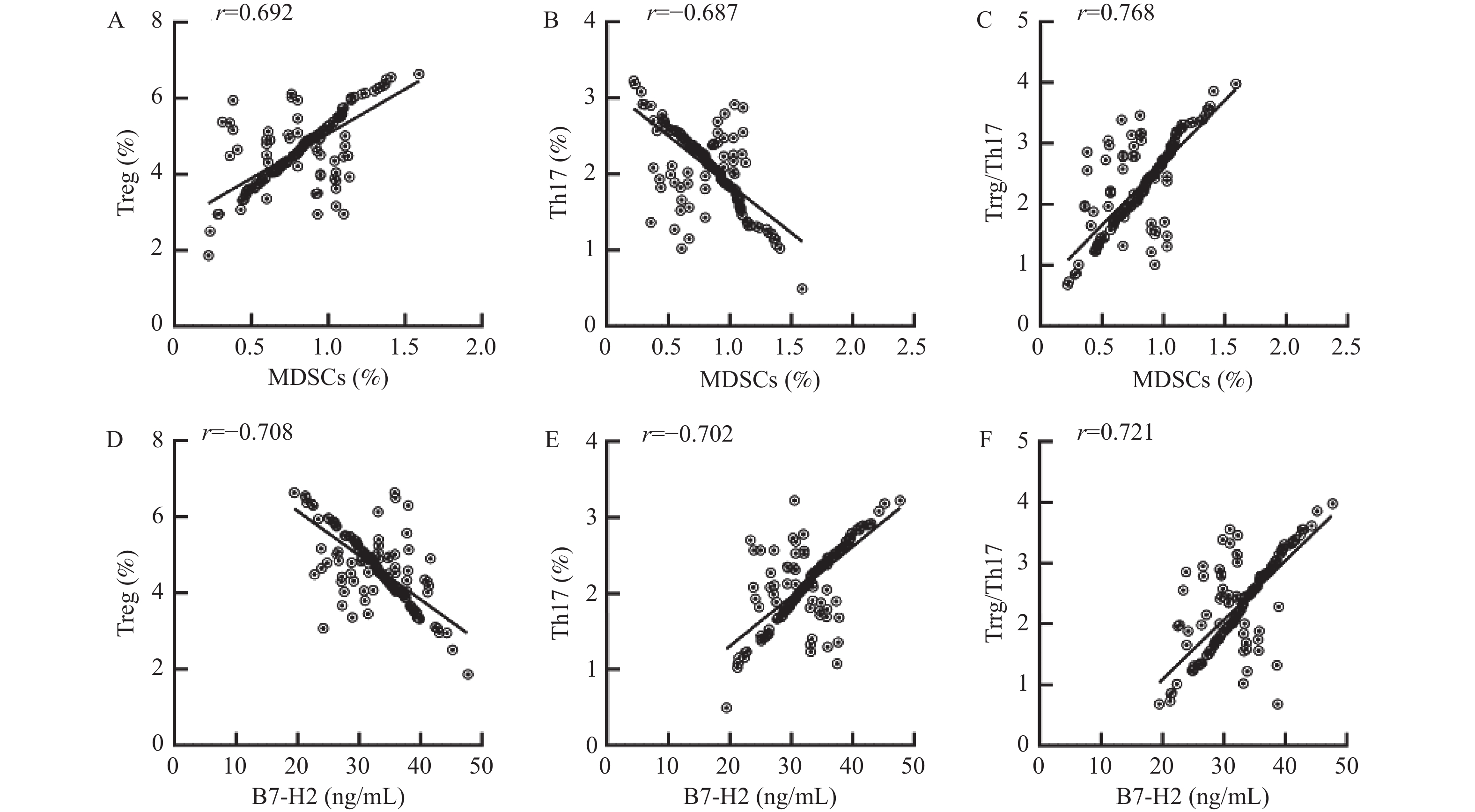
图 3 ITP组治疗前MDSCs、B7-H2与Treg/Th17免疫失衡相关性
A:MDSCs与Treg相关性;B:MDSCs与Th17相关性;C:MDSCs与Treg/Th17相关性;D:B7-H2与Treg相关性;E:B7-H2与Th17相关性;F:B7-H2与Treg/Th17相关性。
Figure 3. Correlation of MDSCs,B7-H2 with Treg/Th17 immune imbalance before treatment in ITP group
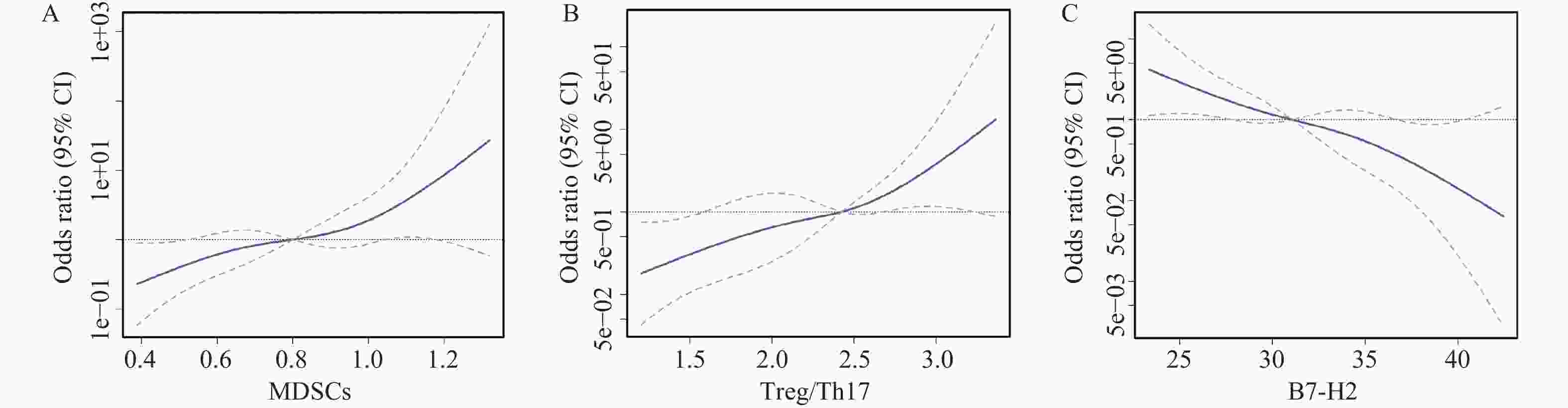
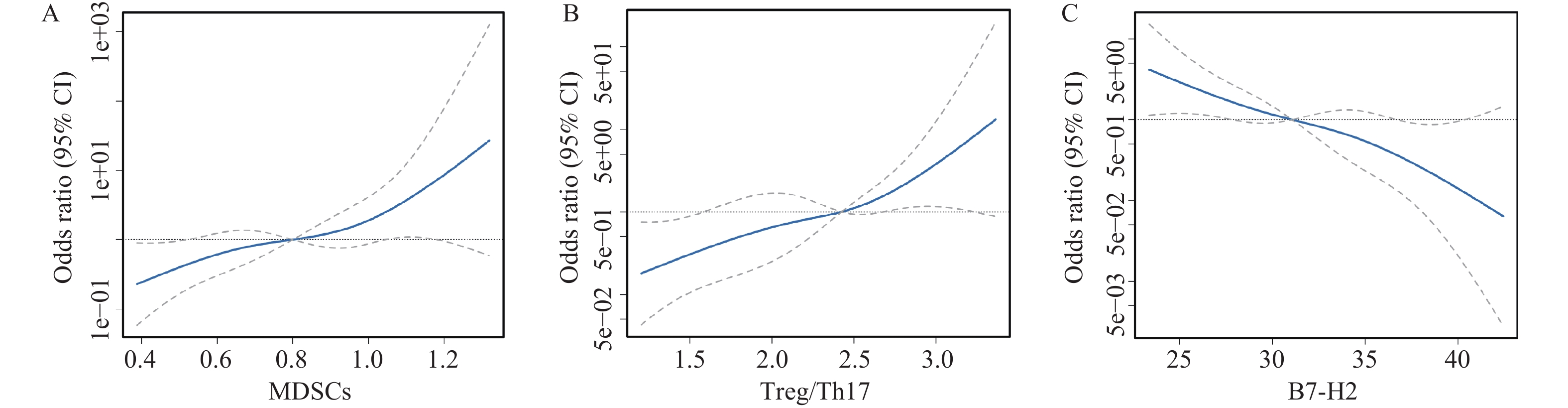
图 4 治疗前MDSCs、B7-H2、Treg/Th17与疗效的相关性
A:治疗前MDSCs与疗效的相关性;B:治疗前Treg/Th17与疗效的相关性;C:治疗前B7-H2与疗效的相关性。
Figure 4. Correlation of pre-treatment MDSCs,B7-H2,Treg/Th17 with treatment efficacy
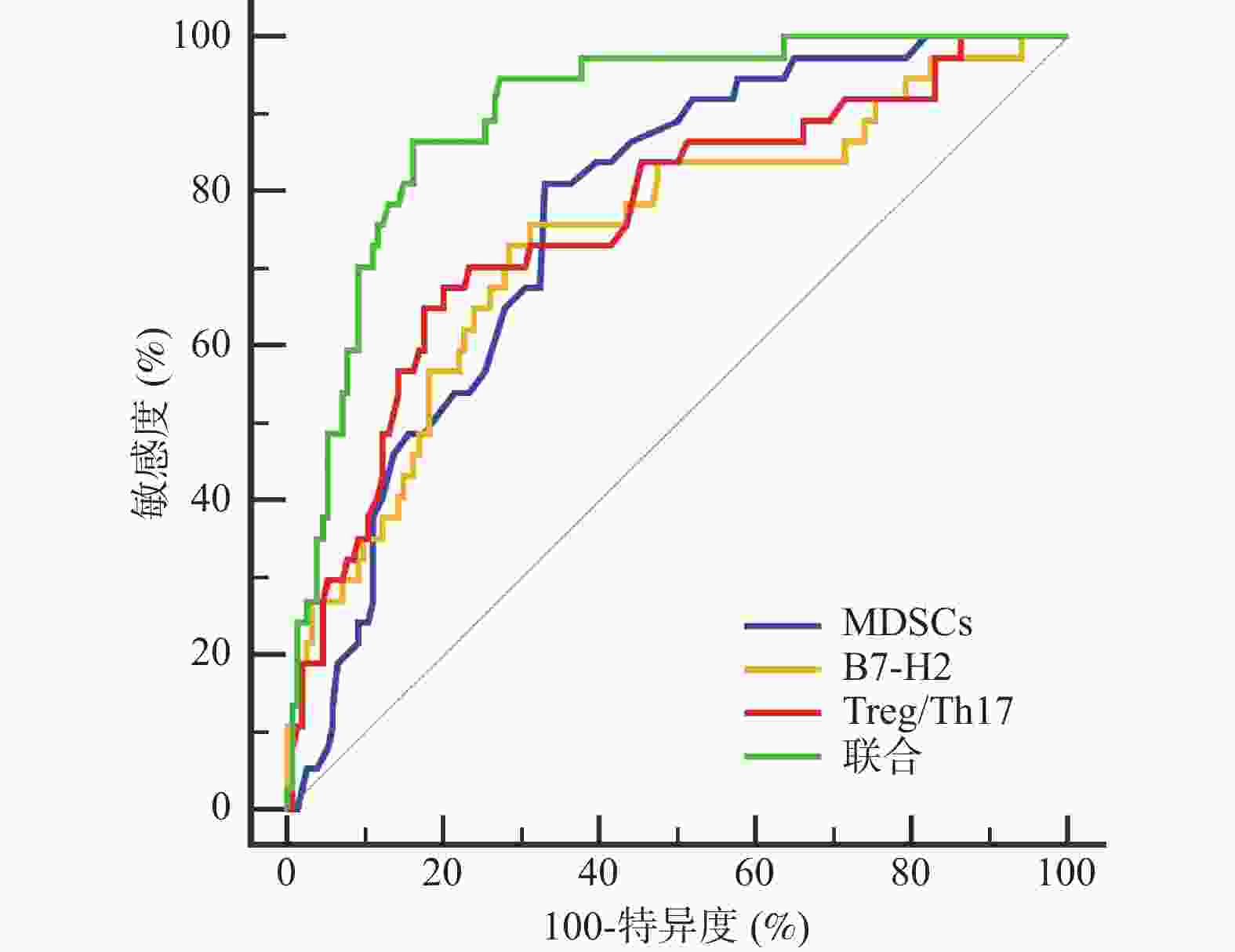
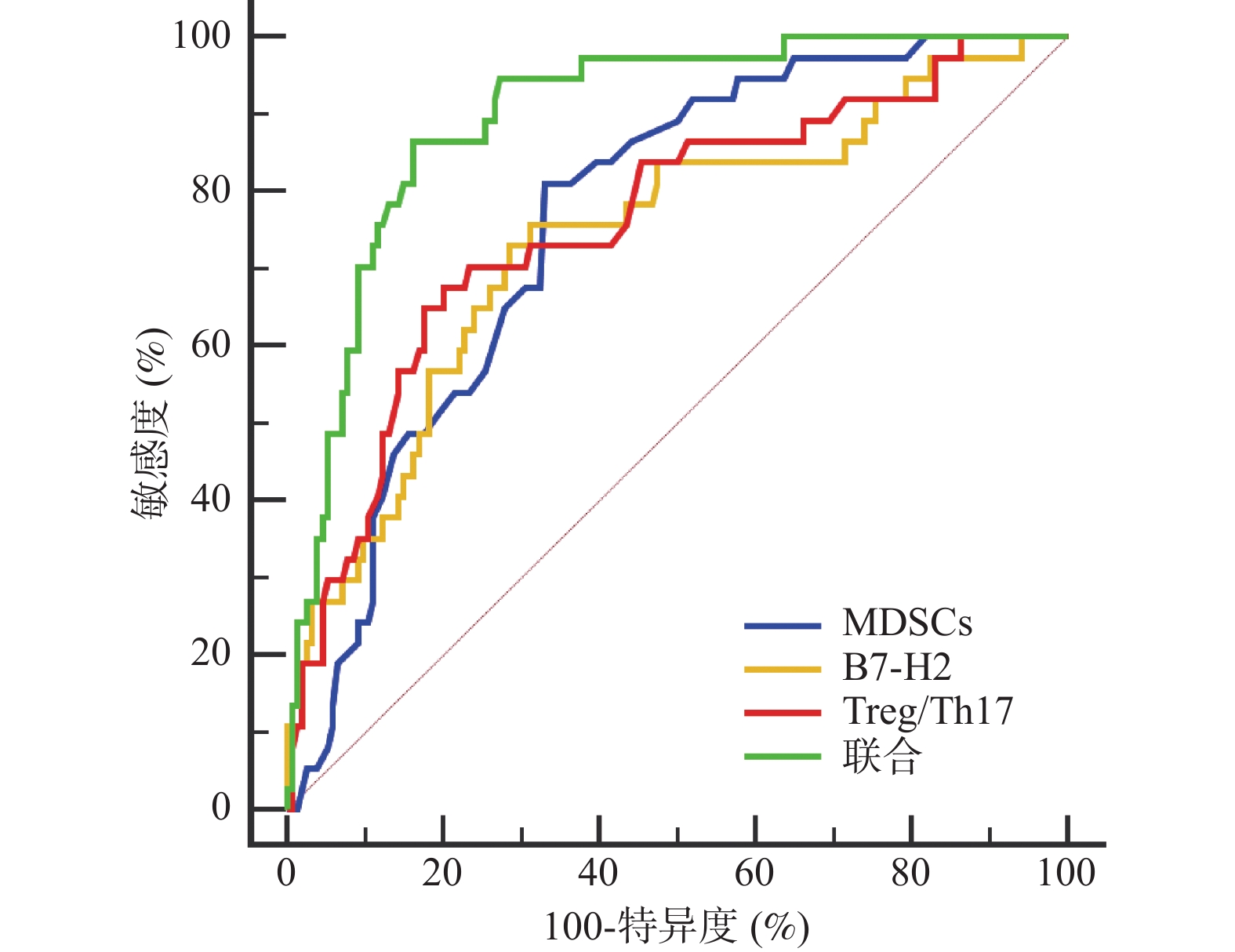
图 5 治疗前MDSCs、B7-H2、Treg/Th17预测疗效的ROC曲线
Figure 5. ROC curves of pre-treatment MDSCs,B7-H2,and Treg/Th17 for predicting treatment efficacy
表 1 两组一般资料比较[($ \bar x \pm s $)/n(%)]
Table 1. Comparison of general data between the two groups [($ \bar x \pm s $)/n(%)]
组别 n 性别 年龄(岁) 体质量指数(kg/m2) 男 女 ITP组 191 25(13.09) 166(86.91) 44.32 ± 6.22 24.11 ± 2.74 对照组 191 31(16.23) 160(83.77) 43.26 ± 5.09 23.88 ± 3.02 t/χ2 0.753 1.823 0.780 P 0.385 0.069 0.436  下载: 导出CSV
下载: 导出CSV
表 2 建模集与验证集患者的一般资料比较[($ \bar x \pm s $)/n(%)]
Table 2. Comparison of general data between training set and the validation set [($ \bar x \pm s $)/ n (%)]
组别 n 性别 年龄(岁) 体质量
指数
(kg/m2)基线血
小板
(×109/L)巨核细胞
总数
(个/全片)原始+
幼稚型
(%)颗粒型
(%)产板型
(%)裸核型
(%)PAIgG
(ng/mL)PAIgA
(ng/mL)PAIgM
(ng/mL)男 女 建模集 191 25(13.09) 166(86.91) 44.32±6.22 24.11±2.74 16.62±5.35 86.35±15.42 12.58±3.61 65.37±10.25 8.42±2.75 13.63±4.28 68.54±15.32 32.45±8.66 45.62±11.37 验证集 52 11(21.15) 41(78.85) 45.20±7.14 24.02±2.25 17.11±4.98 84.99±13.20 11.86±3.05 63.99±9.86 8.12±2.63 12.57±3.94 66.96±14.29 30.99±9.14 42.23±10.26 t/χ2 2.107 −0.876 0.218 −0.594 0.581 1.316 0.868 0.704 1.610 0.669 1.065 1.945 P 0.147 0.382 0.828 0.553 0.562 0.190 0.386 0.482 0.109 0.504 0.288 0.053
下载: 导出CSV
表 3 ITP组与对照组MDSCs、B7-H2、Treg/Th17比较($ \bar x \pm s $)
Table 3. Comparison of MDSCs,B7-H2,Treg/Th17 between ITP group and control group ($ \bar x \pm s $)
组别 n MDSCs(%) B7-H2(ng/mL) Treg(%) Th17(%) Treg/Th17 ITP组 191 0.82 ± 0.27 31.94 ± 5.13 4.78 ± 0.92 2.04 ± 0.45 2.34 ± 0.66 对照组 191 1.76 ± 0.40 20.56 ± 3.78 7.20 ± 1.85 0.96 ± 0.30 7.50 ± 0.92 t 26.919 24.681 16.187 27.598 62.983 P <0.001* <0.001* <0.001* <0.001* <0.001* *P < 0.05。
下载: 导出CSV
表 4 ITP患者治疗前后MDSCs、B7-H2、Treg/Th17比较($ \bar x \pm s $)
Table 4. Comparison of MDSCs,B7-H2,Treg/Th17 in ITP patients before and after treatment ($ \bar x \pm s $)
组别 n MDSCs(%) B7-H2(ng/mL) Treg/Th17 总有效 154 治疗前 0.89 ± 0.27 30.33 ± 5.02 2.45 ± 0.61 治疗后 1.45 ± 0.43∆ 25.10 ± 4.63∆ 5.47 ± 0.85∆ t 13.687 9.504 35.821 P <0.001* <0.001* <0.001* 无效 37 治疗前 0.53 ± 0.15 38.64 ± 4.99 1.88 ± 0.60 治疗后 0.56 ± 0.18 37.25 ± 5.04 1.95 ± 0.66 t 0.779 1.192 0.477 P 0.439 0.237 0.635 *P < 0.001;与无效治疗后比较,∆P < 0.05。
下载: 导出CSV
表 5 治疗前MDSCs、B7-H2、Treg/Th17对ITP疗效的影响
Table 5. Effect of pre-treatment MDSCs,B7-H2,and Treg/Th17 on ITP treatment efficacy
自变量 β SE Wald χ2 OR 95%CI P 下限 上限 MDSCs −0.672 0.256 6.895 0.511 0.289 0.902 0.009* B7-H2 0.455 0.144 9.934 1.576 1.326 1.874 0.002* Treg/Th17 −0.537 0.205 6.868 0.584 0.379 0.901 0.009* 常数项 1.914 0.482 15.768 − − − <0.001* *P < 0.05。
下载: 导出CSV
表 6 PSM后两组的临床资料比较
Table 6. Comparison of clinical data between the two groups after PSM
组别 n 性别 年龄(岁) 病程(月) 体质量指数(kg/m2) 基线血小板(×10⁹/L) 男 女 总有效组 37 18(48.65) 19(51.35) 44.32 ± 6.22 5.62 ± 1.79 23.99 ± 2.61 25.89 ± 6.35 无效组 37 17(45.95) 20(54.05) 45.20 ± 7.14 5.70 ± 1.58 24.05 ± 2.38 27.03 ± 7.19 t/χ2 0.054 0.565 0.204 0.103 0.723 P 0.816 0.574 0.839 0.918 0.472
下载: 导出CSV
表 7 匹配后Logistic回归结果
Table 7. Results of Logistic regression after matching
自变量 OR 95%CI P 下限 上限 MDSCs 0.656 0.463 0.930 0.018* B7-H2 1.697 1.250 2.304 <0.001* Treg/Th17 0.627 0.404 0.972 0.037* *P < 0.05。
下载: 导出CSV
表 8 治疗前MDSCs、B7-H2、Treg/Th17预测疗效的价值
Table 8. Predictive values of pre-treatment MDSCs,B7-H2,and Treg/Th17 for treatment efficacy
指标 AUC 95%CI cut-off值 敏感度(%) 特异度(%) P MDSCs 0.764 0.697~0.822 0.63 81.08 66.88 <0.001* B7-H2 0.739 0.671~0.800 35.18 75.68 68.83 <0.001* Treg/Th17 0.761 0.694~0.820 2.06 67.57 79.87 <0.001* 联合 0.898 0.846~0.937 86.49 83.77 <0.001* *P < 0.05。
下载: 导出CSV
表 9 骨髓巨核细胞、血小板抗体与MDSCs、B7-H2、Treg/Th17相关性(r值)
Table 9. Correlation of bone marrow megakaryocytes and platelet antibodies with MDSCs,B7-H2 and Treg/Th17 (r value)
指标 MDSCs B7-H2 Treg/Th17 颗粒型巨核细胞 −0.685* 0.712* −0.703* 产板型巨核细胞 0.724* −0.695* 0.731* 裸核型巨核细胞 0.315* −0.332* 0.326* PAIgG −0.673* 0.708* −0.689* PAIgA −0.592* 0.635* −0.614* PAIgM −0.625* 0.651* −0.638* *P < 0.05。
下载: 导出CSV
-
[1] 侯兰芬, 李文静, 李丽. 免疫性血栓性血小板减少性紫癜临床误诊分析[J]. 临床误诊误治, 2024, 37(14): 1-4. [2] Ben Abdesslem N, Mahjoub A, Fendouli I, et al. Choroidal ischemia and optic neuropathy as manifestations of idiopathic thrombocytopenic Purpura[J]. J Fr Ophtalmol, 2023, 46(6): e183-e186. doi: 10.1016/j.jfo.2022.12.007 [3] Demir A M, Ümit E G, Ar M C, et al. Management of adult primary immune thrombocytopenia: Delphi- based consensus recommendations[J]. Tjh, 2024, 41(2): 97-104. doi: 10.4274/tjh.galenos.2024.2024.0055 [4] 李芹芝, 段东升, 王秀娟, 等. 高迁移率族蛋白B1(HMGB1)促进髓样树突状细胞成熟增加原发免疫性血小板减少症患者Th17细胞/Treg比例[J]. 细胞与分子免疫学杂志, 2025, 41(1): 45-50. doi: 10.13423/j.cnki.cjcmi.009894 [5] Wang L, Wang H, Zhu M, et al. Platelet-derived TGF-β1 induces functional reprogramming of myeloid-derived suppressor cells in immune thrombocytopenia[J]. Blood, 2024, 144(1): 99-112. doi: 10.1182/blood.2023022738 [6] 王超, 韩萍, 唐丽丽. 原发免疫性血小板减少症患者血清B7同源蛋白2、肿瘤坏死因子相关凋亡诱导配体、白细胞介素-37、白细胞介素-17A水平及临床意义[J]. 中国医师进修杂志, 2023, 46(6): 516-520. [7] 中华医学会血液学分会止血与血栓学组. 成人原发免疫性血小板减少症诊断与治疗中国专家共识(2016年版)[J]. 中华血液学杂志, 2016, 37(2): 89-93. [8] Liu X G, Hou M. Interpretation of the updated international consensus report on the investigation and management of adult primary immune thrombocytopenia (version 2019)[J]. Chin J Hematol, 2020, 41(2): 89-92. doi: 10.1182/bloodadvances.2019000812 [9] Gu H, Wang Z, Xie X, et al. HIF-1α induced by hypoxic condition regulates Treg/Th17 axis polarization in chronic immune thrombocytopenia[J]. Int Immunopharmacol, 2024, 131: 111810. doi: 10.1016/j.intimp.2024.111810 [10] 赵萌, 金立方, 李小丰, 等. 原发免疫性血小板减少症miRNA181a-5p表达与Treg/Th17失衡关系的研究[J]. 中国实验血液学杂志, 2022, 30(1): 237-243. [11] Hou Y, Xie J, Wang S, et al. Glucocorticoid receptor modulates myeloid-derived suppressor cell function via mitochondrial metabolism in immune thrombocytopenia[J]. Cell Mol Immunol, 2022, 19(7): 764-776. doi: 10.1038/s41423-022-00859-0 [12] Yazdanbakhsh K, Provan D, Semple J W. The role of T cells and myeloid-derived suppressor cells in refractory immune thrombocytopenia[J]. Br J Haematol, 2023, 203(1): 54-61. doi: 10.1111/bjh.19079 [13] Ni X, Wang L, Wang H, et al. Low-dose decitabine modulates myeloid-derived suppressor cell fitness via LKB1 in immune thrombocytopenia[J]. Blood, 2022, 140(26): 2818-2834. doi: 10.1182/blood.2022016029 [14] Zhu Y, Wang Y, Zhao Y, et al. Thrombopoietin receptor agonists regulate myeloid-derived suppressor cell-mediated immunomodulatory effects in ITP[J]. Ann Hematol, 2024, 103(8): 2729-2741. doi: 10.1007/s00277-024-05846-1 [15] 张宝君, 杨亚丽, 雷蕊. 银杏内酯B注射液对ITP患者T细胞亚群、MDSCs免疫失衡的影响[J]. 湖南中医药大学学报, 2025, 45(3): 529-533. [16] Kapur R. Impaired glucocorticoid receptor expression and mitochondrial metabolism in MDSCs contribute to glucocorticoid resistance in immune thrombocytopenia[J]. Cell Mol Immunol, 2022, 19(7): 858-860. doi: 10.1038/s41423-022-00880-3 [17] 林隆, 彭峰, 金海丽, 等. MDSCs可调控Th1、Th2、Th17相关细胞因子水平加重哮喘小鼠肺损伤[J]. 广东医学, 2022, 43(9): 1112-1117. doi: 10.13820/j.cnki.gdyx.20213288 [18] Park R, Yu J, Shahzad M, et al. The immune regulatory function of B7-H3 in malignancy: Spotlight on the IFN-STAT1 axis and regulation of tumor-associated macrophages[J]. Immunol Res, 2024, 72(4): 526-537. doi: 10.1007/s12026-024-09458-9 [19] 陈冰燕, 徐绘婷, 丁翔宇, 等. 乙型肝炎病毒相关原发性肝癌患者血清B7-H2、 白细胞介素6水平及其与预后相关性研究[J]. 创伤与急危重病医学, 2022, 10(4): 292-295+299. [20] Mortezaee K, Majidpoor J. Alternative immune checkpoints in immunoregulatory profile of cancer stem cells[J]. Heliyon, 2023, 9(12): e23171. doi: 10.1016/j.heliyon.2023.e23171 [21] Ge J, Yin X, Sun X, et al. Chemotherapy resistance in acute myeloid leukemia is associated with decreased anti-tumor immune response through MHC molecule and B7 family members[J]. Discov Oncol, 2024, 15(1): 221. doi: 10.1007/s12672-024-01072-3 [22] Fan J, Wang Y, Liang X, et al. B7-H6 enhances F-actin rearrangement by targeting c-MYC activation to promote medulloblastoma migration and invasion[J]. Med Oncol, 2023, 40(3): 85. doi: 10.1007/s12032-023-01947-5 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 85
- HTML全文浏览量: 68
- PDF下载量: 64
- 被引次数: 0
