

Correlation between T1-mapping and Feature Tracking in Hypertrophic Cardiomyopathy
-
摘要:
目的 探讨肥厚型心肌病(hypertrophic cardiomyopathy,HCM)患者T1-mapping与特征追踪的相关性。 方法 回顾性收集2016年1月至2021年7月在云南省第一人民医院住院的86例HCM患者的心脏磁共振(cardiovascular magnetic resonance,CMR)数据,对比钆延迟增强(late gadolinium enhancement,LGE)阳性组(n = 59)与LGE阴性组(n = 27)患者增强前后T1值、心肌细胞外容积比率(extracellular volume,ECV)、纵向应变(longitudinal strain,LS)、圆周应变(circumferential strain,CS)、径向应变(radial strain,RS)和应变率参数差异。 结果 (1)LGE阳性组患者年龄小,NYHA Ⅲ~Ⅳ级比例高,舒张末期最大室壁厚度和左心室质量指数大(P < 0.05);(2)LGE(+)组增强前T1值较LGE(−)组大,LGE阳性组ECV值较LGE阴性组高(P < 0.05);(3)LGE阳性组中整体纵向应变(global longitudinal strain,GLS)与左心室质量指数、左室舒张末期最大室壁厚度、LGE%、T1值、和ECV呈负性相关(分别为r = −0.418,P = 0.008;r = −0.711,P = 0.021;r = −0.621,P = 0.015;r = −0.372,P = 0.020;r = −0.583,P = 0.010)。 结论 HCM患者心肌增强后,LGE阳性者GLS降低,后者与左心室舒张末期容积、左心室质量指数、舒张末期最大室壁厚度、LGE%、以及增强前的T1值和ECV呈明显负相关。 -
关键词:
- 肥厚型心肌病 /
- T1-mapping /
- 细胞外容积 /
- 延迟强化 /
- 整体纵向应变
Abstract:Objective To explore the correlation between T1-mapping and feature tracking in patients with Hypertrophic Cardiomyopathy (HCM). Methods Cardiac magnetic resonance (CMR) data were retrospectively collected from 86 HCM patients hospitalized at Yunnan Provincial First People's Hospital between January 2016 and July 2021. The differences in T1 values before and after contrast enhancement, extracellular volume (ECV), longitudinal strain (LS), circumferential strain (CS), radial strain (RS), and strain rate parameters were compared between the late gadolinium enhancement (LGE)-positive group (59 cases) and LGE-negative group (27 cases). Results (1) Patients in the LGE-positive group were younger with a higher proportion of NYHA class III-IV, larger end-diastolic maximal wall thickness, and greater left ventricular mass index (P < 0.05); (2) Pre-contrast T1 values were higher in the LGE(+) group compared to the LGE(-) group, and ECV values were elevated in the LGE-positive group (P < 0.05); (3) In the LGE-positive group, global longitudinal strain (GLS) showed negative correlations with left ventricular mass index, left ventricular end-diastolic maximal wall thickness, LGE%, T1 value, and ECV (r = −0.418, P = 0.008; r = −0.711, P = 0.021; r = −0.621, P = 0.015; r = −0.372, P = 0.020; r = −0.583, P = 0.010, respectively). Conclusion In HCM patients with myocardial enhancement, GLS is reduced in LGE-positive cases, which shows significant negative correlations with left ventricular end-diastolic volume, left ventricular mass index, end-diastolic maximal wall thickness, LGE%, and pre-contrast T1 value and ECV. -
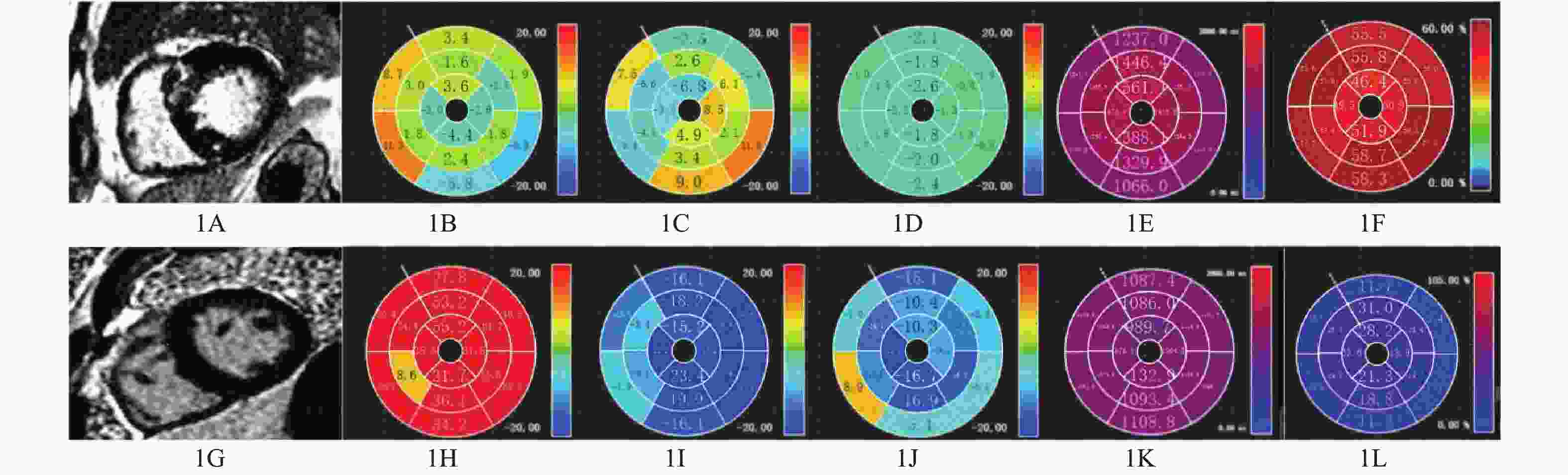
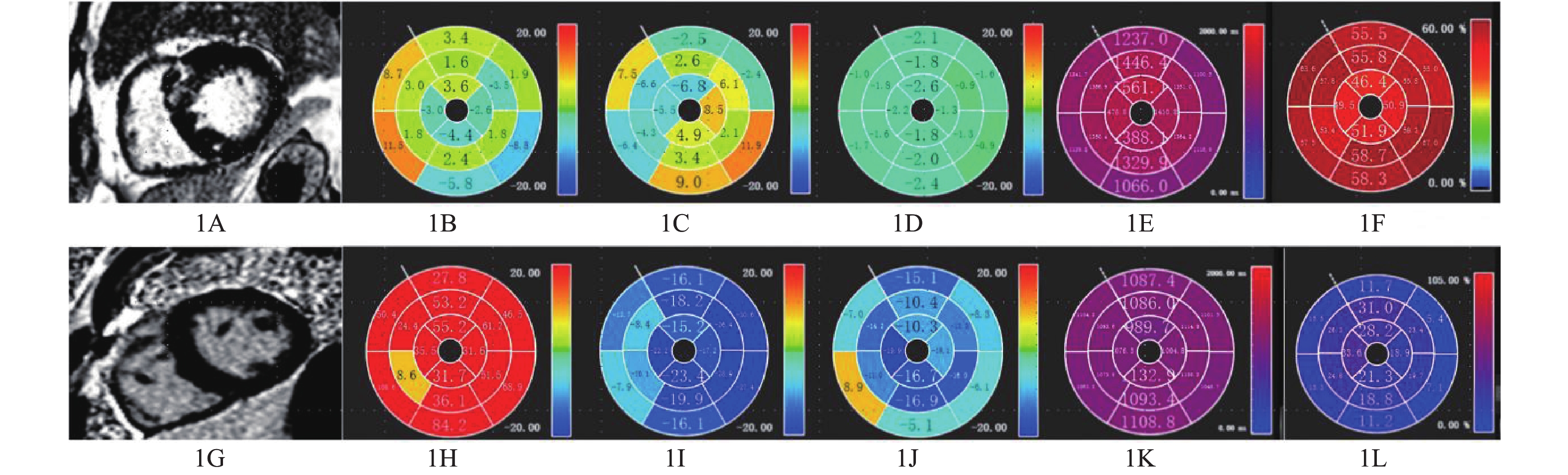
图 1 肥厚型心肌病患者心脏磁共振成像
A:LGE阳性;B~D:特征追踪显示GLS、GCS、GRS明显降低;E~F:增强前T1值及ECV值明显增加;G:LGE阴性;H~J:特征追踪显示GLS、GCS、GRS轻度降低;K~L:增强前T1值及ECV值轻度增加。
Figure 1. Cardiac magnetic resonance imaging in patients with hypertrophic cardiomyopathy
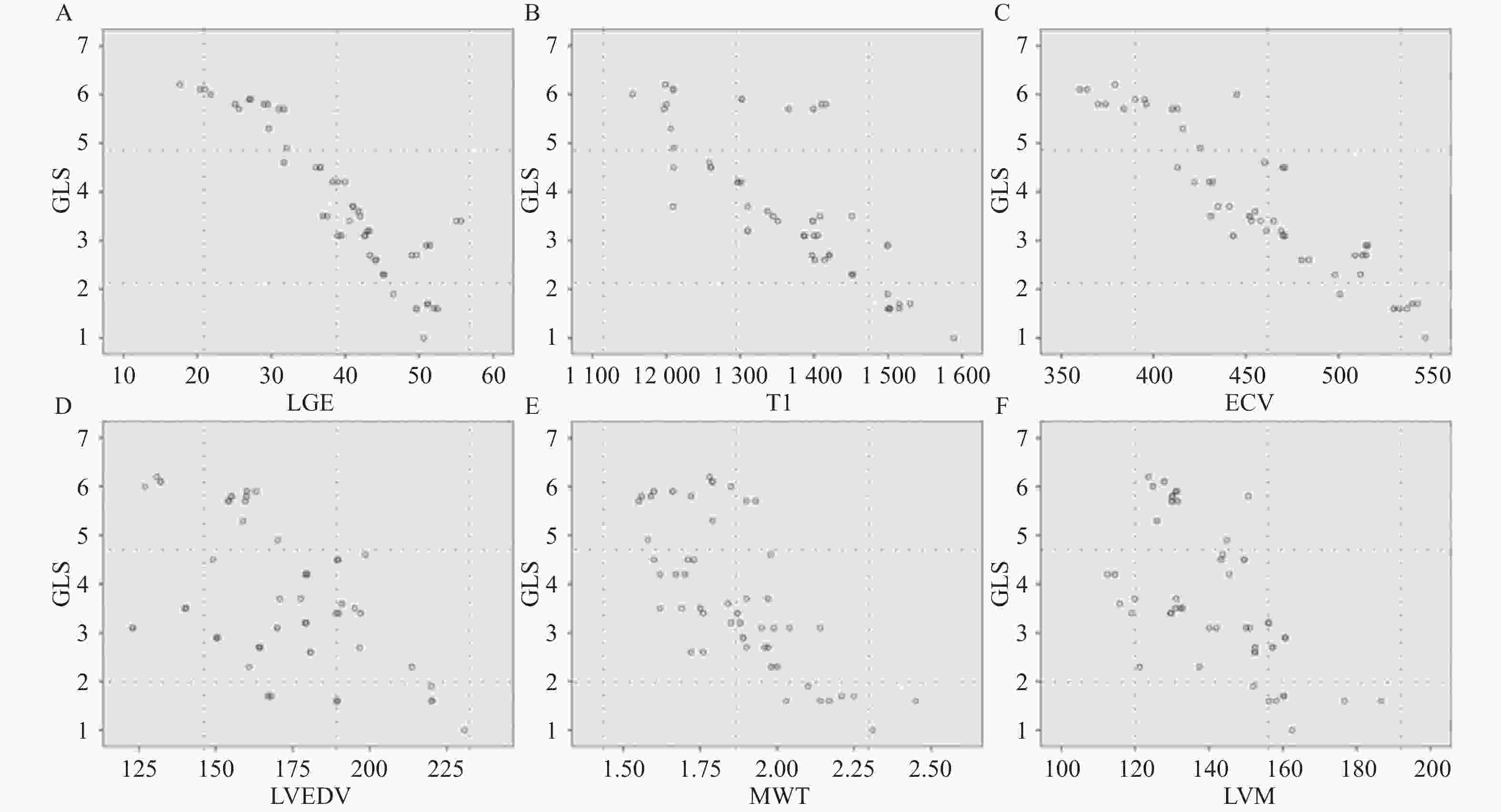
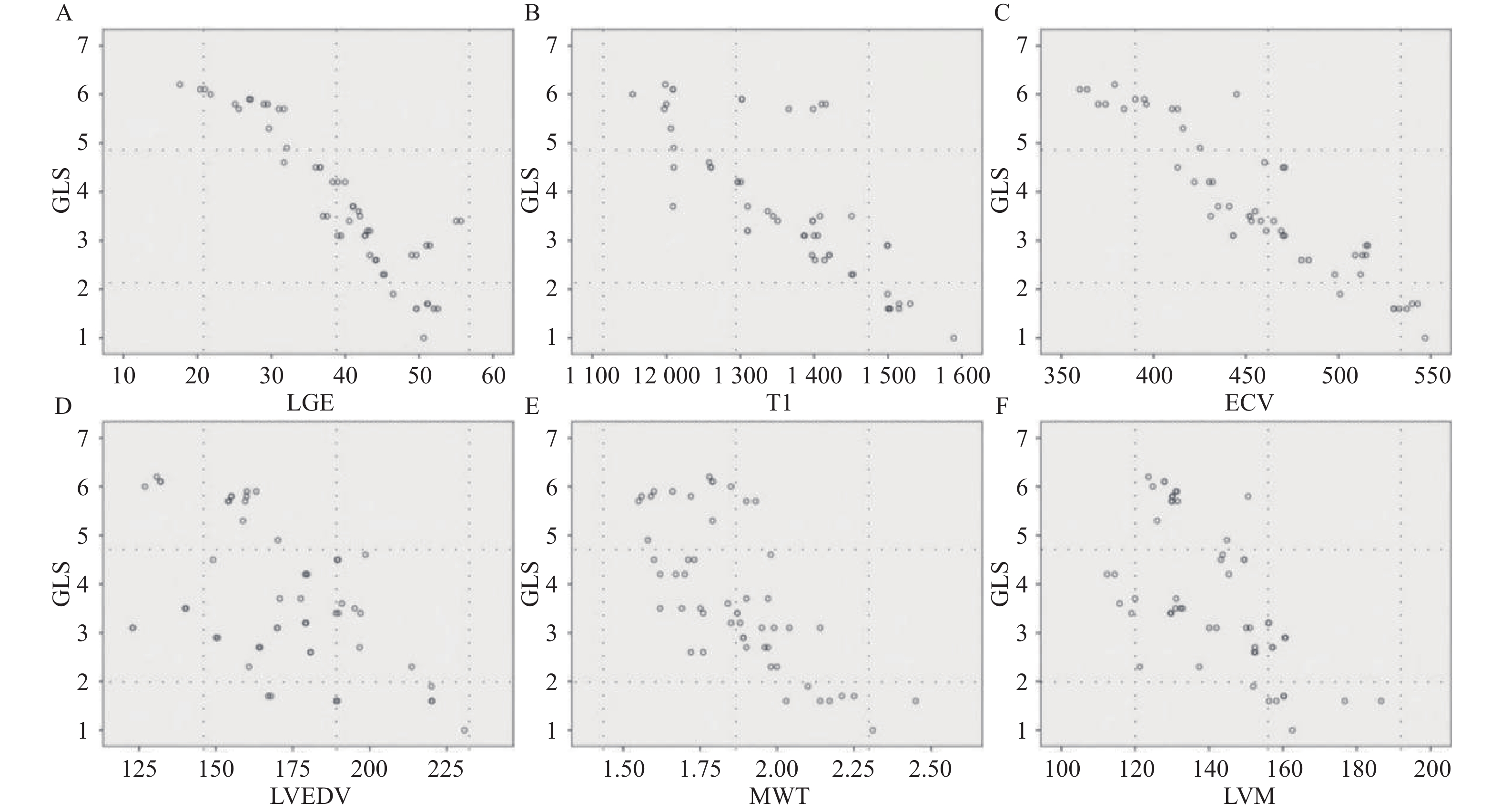
图 2 LGE阳性组患者中整体纵向应变(GLS)与LGE%、增强后T1值、ECV、左心室舒张末期最大室壁厚度和左心室质量指数相关性散点图
A:LGE%;B:增强后T1值;C:ECV;D~E:左心室舒张末期最大室壁厚度;F:左心室质量指数。
Figure 2. LGE-positive group, global longitudinal strain (GLS) and LGE%, post-enhanced T1 value, ECV, LVEDMWT and LVMI correlation scatter plot
表 1 肥厚型心肌病患者LGE阳性组与LGE阴性组一般临床资料的比较[n (%)/($ \bar x \pm s $)/M(Q1,Q3)]
Table 1. Comparison of general clinical data of two groups[n (%)/($ \bar x \pm s $)/M(Q1,Q3)]
项目 LGE阴性组 (n = 27) LGE阳性组 (n = 59) X2/t/Z P 男性 17(62.9) 51(86.4) 1.032 0.658 年龄(岁) 50.7 ± 17.1 41.4 ± 15.2 −1.074 0.027* 收缩压(mmHg) 133.75 ± 12.17 140.00 ± 21.64 2.836 0.530 舒张压(mmHg) 91.50 ± 8.99 87.91 ± 13.96 3.170 0.161 NT-proBNP (ng/L) 865.2(451.2, 1597.2 )4967.5 (1303.4 ,8183.6 )65.471 0.012* 肌酐(μmol/L) 87.75 ± 19.02 80.64 ± 13.34 1.035 0.314 心肌肌钙蛋白I(μg/L) 0.175(0.053,0.321) 0.898(0.247,1.783) 7.230 0.040* NHYA心功能III/IV 0 36(59) 1.000 <0.001* 症状 胸痛 15(50) 26(74) 0.791 0.312 晕厥 2(7) 14(18) −1.173 0.020* 呼吸困难 10(43) 37(62.7) 0.716 0.044* 注:NT-proBNP:N末端B型利钠肽前体;NHYA:纽约心脏病协会;*P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 两组肥厚型心肌病患者CMR检查结果比较($\bar x \pm s $)
Table 2. Comparison of imaging findings between the two groups($\bar x \pm s $)
项目 LGE阴性组 (n = 27) LGE阳性组 (n = 59) t P 左室射血分数(%) 69.6 ± 4.8 63.2 ± 7.5 0.714 0.037* 心脏指数(L/(min·m2) 2.98 ± 0.68 2.6 ± 0.92 0.990 0.001* 左心室舒张末期容积(mL/m2) 139.37 ± 24.25 163.02 ± 72.13 −0.133 0.039* 左心室收缩末期容积(mL/m2) 58.42 ± 34.78 45.87 ± 13.93 −0.962 0.073 每搏输出量(mL/m2) 116.00 ± 9.67 94.11 ± 11.75 0.234 0.239 左心室舒张末期最大室壁厚度(cm) 1.82 ± 0.21 1.96 ± 0.46 −2.975 0.024* 左心室质量指数(g/m2) 81.03 ± 11.87 137.53 ± 14.16 −8.006 0.001* *P < 0.05。
下载: 导出CSV
表 3 肥厚型心肌病LGE阳性组与LGE阴性组患者的T1-mapping值比较($\bar x \pm s $)
Table 3. Comparison of T1-mapping between LGE-positive group and LGE-nagative group in hypertrophic cardiomyopathy ($\bar x \pm s $)
项目 LGE 阴性组 (n = 27) LGE 阳性组 (n = 59) t P 增强前T1值(ms) 1214.62 ± 330.251392.74 ± 284.52−2.351 0.027* 增强后T1值(ms) 765.71 ± 103.40 893.23 ± 165.42 0.593 0.053 ECV(%) 0.24 ± 0.07 0.49 ± 0.06 −1.490 0.014* *P < 0.05。
下载: 导出CSV
表 4 肥厚型心肌病LGE阳性组与LGE阴性组患者特征追踪值比较($\bar x \pm s $)
Table 4. Comparison of feature values between LGE-positive group and LGE-nagative group in hypertrophic cardiomyopathy ($\bar x \pm s $)
项目 LGE 阴性组 (n = 27) LGE 阳性组 (n = 59) t P 收缩期峰值局部应变(%) 纵向应变 −6.3 ± 2.7 −9.1 ± 4.7 −1.579 0.023* 圆周应变 −11.2 ± 5.3 −17.4 ± 3.9 −7.804 0.001* 径向应变 12.6 ± 4.2 19.3 ± 4.1 −4.453 0.006* 收缩期峰值局部应变率(s-1) 纵向应变率 −89.4 ± 15.6 −119.4 ± 24.7 −8.903 < 0.001* 圆周应变率 −95.0 ± 12.3 −139.2 ± 15.9 −9.542 < 0.001* 径向应变率 81.9 ± 8.0 141.3 ± 22.5 −8.750 < 0.001* *P < 0.05。
下载: 导出CSV
-
[1] Chan R H, Maron B J, Olivotto I, et al. Prognostic value of quantitative contrast-enhanced cardiovascular magnetic resonance for the evaluation of sudden death risk in patients with hypertrophic cardiomyopathy[J]. Circulation, 2014, 130(6): 484-495. [2] 李志明, 韩丹, 杞天付, 等. 心脏磁共振T1mapping技术评估肥厚型心肌病心肌纤维化[J]. 中国医学影像学杂志, 2022, 30(4): 341-347. doi: 10.3969/j.issn.1005-5185.2022.04.008 [3] 中国医师协会心力衰竭专业委员会, 中华心力衰竭和心肌病杂志编辑委员会. 中国肥厚型心肌病管理指南2017[J]. 中华心力衰竭和心肌病杂志(中英文), 2017, 1(2): 65-86. [4] 张艳, 吴昆华, 李清, 等. 肥厚型心肌病患者心肌纤维化范围的相关因素分析[J]. 中华心血管病杂志, 2021, 49(1): 31-36. doi: 10.3760/cma.j.cn112148-20200609-00475 [5] 张艳, 庞明杰, 陈浩强, 等. 心脏磁共振组织追踪技术定量评价心肌运动参数在肥厚型心肌病心源性猝死风险评估中的应用价值[J]. 放射学实践, 2024, 39(11): 1472-1480. [6] Zhang Y, Wu K H, Li Q, et al. Analysis on related factors of myocardial fibrosis in patients with hypertrophic cardiomyopathy[J]. Zhonghua Xin Xue Guan Bing Za Zhi, 2021, 49(1): 31-36. [7] Ho C Y, López B, Coelho-Filho O R, et al. Myocardial fibrosis as an early manifestation of hypertrophic cardiomyopathy[J]. N Engl J Med, 2010, 363(6): 552-563. doi: 10.1056/NEJMoa1002659 [8] Rowin E J, Maron M S. The role of cardiac MRI in the diagnosis and risk stratification of hypertrophic cardiomyopathy[J]. Arrhythm Electrophysiol Rev, 2016, 5(3): 197-202. [9] 张艳, 赵燕, 吴昆华, 等. 心脏磁共振特征追踪技术在检测成人非梗阻性肥厚型心肌病患者心肌纤维化中的应用[J]. 中华心力衰竭和心肌病杂志, 2021, 5(1): 30-34. [10] Bravo P E, Zimmerman S L, Luo H C, et al. Relationship of delayed enhancement by magnetic resonance to myocardial perfusion by positron emission tomography in hypertrophic cardiomyopathy[J]. Circ Cardiovasc Imaging, 2013, 6(2): 210-217. doi: 10.1161/CIRCIMAGING.112.000110 [11] Moorman A F M, Christoffels V M. Cardiac chamber formation: Development, genes, and evolution[J]. Physiol Rev, 2003, 83(4): 1223-1267. [12] Xu J, Zhuang B, Sirajuddin A, et al. MRI T1 mapping in hypertrophic cardiomyopathy: Evaluation in patients without late gadolinium enhancement and hemodynamic obstruction[J]. Radiology, 2020, 294(2): 275-286. doi: 10.1148/radiol.2019190651 [13] 张艳, 庞明杰, 张宏江, 等. T1-mapping和ECV在诊断肥厚型心肌病和H型高血压心室肥厚中的临床价值[J]. 昆明理工大学学报(自然科学版), 2020, 45(4): 109-114. doi: 10.16112/j.cnki.53-1223/n.2020.04.253 [14] Shi R Y, Wu R, An D L, et al. Texture analysis applied in T1 maps and extracellular volume obtained using cardiac MRI in the diagnosis of hypertrophic cardiomyopathy and hypertensive heart disease compared with normal controls[J]. Clin Radiol, 2021, 76(3): 236. e9-236. e19. [15] Chu L C, Corona-Villalobos C P, Halushka M K, et al. Structural and functional correlates of myocardial T1 mapping in 321 patients with hypertrophic cardiomyopathy[J]. J Comput Assist Tomogr, 2017, 41(4): 653-660. doi: 10.1097/RCT.0000000000000564 [16] Arcari L, Hinojar R, Engel J, et al. Native T1 and T2 provide distinctive signatures in hypertrophic cardiac conditions - comparison of uremic, hypertensive and hypertrophic cardiomyopathy[J]. Int J Cardiol, 2020, 306: 102-108. doi: 10.1016/j.ijcard.2020.03.002 [17] Neisius U, El-Rewaidy H, Nakamori S, et al. Radiomic analysis of myocardial native T(1) imaging discriminates between hypertensive heart disease and hypertrophic cardiomyopathy[J]. JACC Cardiovasc Imaging, 2019, 12(10): 1946-1954. doi: 10.1016/j.jcmg.2018.11.024 [18] Huang L, Ran L, Zhao P, et al. MRI native T1 and T2 mapping of myocardial segments in hypertrophic cardiomyopathy: Tissue remodeling manifested prior to structure changes[J]. Br J Radiol, 2019, 92(1104): 20190634. doi: 10.1259/bjr.20190634 [19] Deborde E, Dubourg B, Bejar S, et al. Differentiation between Fabry disease and hypertrophic cardiomyopathy with cardiac T1 mapping[J]. Diagn Interv Imaging, 2020, 101(2): 59-67. doi: 10.1016/j.diii.2019.08.006 [20] Chen Xiuyu, Zhao Shihua. 2017 SCMR cardiac MRI parameters quantitative technical expert consensus interpretation[J]. Magnetic Resonance Imaging, 2018, 9(5): 368-373. [21] Wang J, Yang F, Liu W, et al. Radiomic analysis of native T(1) mapping images discriminates between MYH7 and MYBPC3-related hypertrophic cardiomyopathy[J]. J Magn Reson Imaging, 2020, 52(6): 1714-1721. doi: 10.1002/jmri.27209 [22] Yang Y, Yin G, Jiang Y, et al. Quantification of left atrial function in patients with non-obstructive hypertrophic cardiomyopathy by cardiovascular magnetic resonance feature tracking imaging: A feasibility and reproducibility study[J]. J Cardiovasc Magn Reson, 2020, 22(1): 1. doi: 10.1186/s12968-019-0589-5 [23] Cavus E, Muellerleile K, Schellert S, et al. CMR feature tracking strain patterns and their association with circulating cardiac biomarkers in patients with hypertrophic cardiomyopathy[J]. Clin Res Cardiol, 2021, 110(11): 1757-1769. doi: 10.1007/s00392-021-01848-5 [24] Zhang Q, Werys K, Popescu I A, et al. Quality assurance of quantitative cardiac T1-mapping in multicenter clinical trials - A T1 phantom program from the hypertrophic cardiomyopathy registry (HCMR) study[J]. Int J Cardiol, 2021, 330: 251-258. doi: 10.1016/j.ijcard.2021.01.026 [25] Yang L, Zhang L, Cao S, et al. Advanced myocardial characterization in hypertrophic cardiomyopathy: Feasibility of CMR-based feature tracking strain analysis in a case-control study[J]. Eur Radiol, 2020, 30(11): 6118-6128. doi: 10.1007/s00330-020-06922-6 [26] Burrage M K, Shanmuganathan M, Masi A, et al. Cardiovascular magnetic resonance stress and rest T1-mapping using regadenoson for detection of ischemic heart disease compared to healthy controls[J]. Int J Cardiol, 2021, 333: 239-245. doi: 10.1016/j.ijcard.2021.03.010 [27] Moore C C, McVeigh E R, Zerhouni E A. Quantitative tagged magnetic resonance imaging of the normal human left ventricle[J]. Top Magn Reson Imaging, 2000, 11(6): 359-371. doi: 10.1097/00002142-200012000-00005 [28] Neisius U, Myerson L, Fahmy A S, et al. Cardiovascular magnetic resonance feature tracking strain analysis for discrimination between hypertensive heart disease and hypertrophic cardiomyopathy[J]. PLoS One, 2019, 14(8): e0221061. doi: 10.1371/journal.pone.0221061 [29] Hinojar R, Fernández-Golfín C, González-Gómez A, et al. Prognostic implications of global myocardial mechanics in hypertrophic cardiomyopathy by cardiovascular magnetic resonance feature tracking. Relations to left ventricular hypertrophy and fibrosis[J]. Int J Cardiol, 2017, 249: 467-472. doi: 10.1016/j.ijcard.2017.07.087 [30] Timmer S A J, Knaapen P. Coronary microvascular function, myocardial metabolism, and energetics in hypertrophic cardiomyopathy: Insights from positron emission tomography[J]. Eur Heart J Cardiovasc Imaging, 2013, 14(2): 95-101. doi: 10.1093/ehjci/jes242 [31] Nucifora G, Muser D, Gianfagna P, et al. Systolic and diastolic myocardial mechanics in hypertrophic cardiomyopathy and their link to the extent of hypertrophy, replacement fibrosis and interstitial fibrosis[J]. Int J Cardiovasc Imaging, 2015, 31(8): 1603-1610. doi: 10.1007/s10554-015-0720-0 [32] Dusenbery S M, Lunze F I, Jerosch-Herold M, et al. Left ventricular strain and myocardial fibrosis in congenital aortic stenosis[J]. Am J Cardiol, 2015, 116(8): 1257-1262. doi: 10.1016/j.amjcard.2015.07.042 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 256
- HTML全文浏览量: 163
- PDF下载量: 73
- 被引次数: 0
