

The Burden and Trends of Ischemic Heart Disease Attributable to Low Physical Activity Globally and in China,1990—2021
-
摘要:
目的 系统分析1990—2021年全球及中国归因于低体力活动(low physical activity,LPA)的缺血性心脏病(ischemic heart disease,IHD)负担,并预测2022—2030年的变化趋势。 方法 基于全球疾病负担2021数据库,采用Joinpoint回归、年龄-时期-队列(age-period-cohort,APC)模型、分解分析及贝叶斯年龄-时期-队列(Bayesian age-period-cohort,BAPC)模型进行趋势分析。 结果 2021年,全球归因于LPA的IHD年龄标准化死亡率(age-standardized mortality rates,ASMR)和伤残调整生命年率(age-standardized DALYs rates,ASDR)分别为2.88/10万和46.63/10万,中国分别为3.52/10万和46.05/10万。Joinpoint回归显示全球ASMR和ASDR呈下降趋势,而中国呈M型波动上升,且性别差异显著。相似地,APC模型也表明全球疾病负担呈下降趋势,而中国呈现先减缓后增长再趋缓的变化趋势,且中国男性的疾病负担较女性增长明显。分解分析显示人口增长和人口老龄化是疾病负担的主要驱动因素。BAPC模型预测显示,预计2030年中国疾病负担增长将高于全球,年轻男性群体更明显。 结论 全球归因于LPA的IHD负担呈下降趋势,但中国因人口增长和人口老龄化导致疾病负担持续攀升,其中女性群体的绝对负担更重,而年轻男性群体呈现上升趋势。 Abstract:Objective To systematically analyze the burden of ischemic heart disease (IHD) attributable to low physical activity (LPA) globally and in China from 1990 to 2021, and to predict its trends up to 2030, thereby providing evidence for formulating relevant healthcare policies. Methods Based on the global burden of disease (GBD) 2021 data, a comprehensive analysis and projection were conducted using Joinpoint regression, age-period-cohort (APC) modeling, decomposition analysis, and Bayesian age-period-cohort (BAPC) modeling. Results In 2021, the global age-standardized mortality rates (ASMR) and age-standardized DALYs rates (ASDR) for IHD attributable to LPA were 2.88 per 100,000 and 46.63 per 100,000, respectively. In China, the corresponding figures were 3.52 per 100,000 and 46.05 per 100,000. Joinpoint regression analysis revealed a declining trend in global ASMR and ASDR, whereas in China, these rates showed an M-shaped fluctuating rise with significant gender disparities. Similarly, the APC model also indicates a downward trend in the global burden of disease, while China shows a pattern of initial deceleration, followed by an increase, and then a renewed moderation. Moreover, the burden of disease among Chinese males has grown more markedly compared to that among females. Decomposition analysis highlighted population growth and aging as the primary drivers of the disease burden. BAPC model projections suggested that by 2030, China’ s disease burden was expected to grow faster than the global average, with the trend being more pronounced among younger male populations. Conclusion The global burden of IHD attributable to LPA is declining. However, in China, due to population growth and aging, the disease burden continues to rise, characterized by a heavier absolute burden among females and a particularly pronounced increasing trend among young males. -
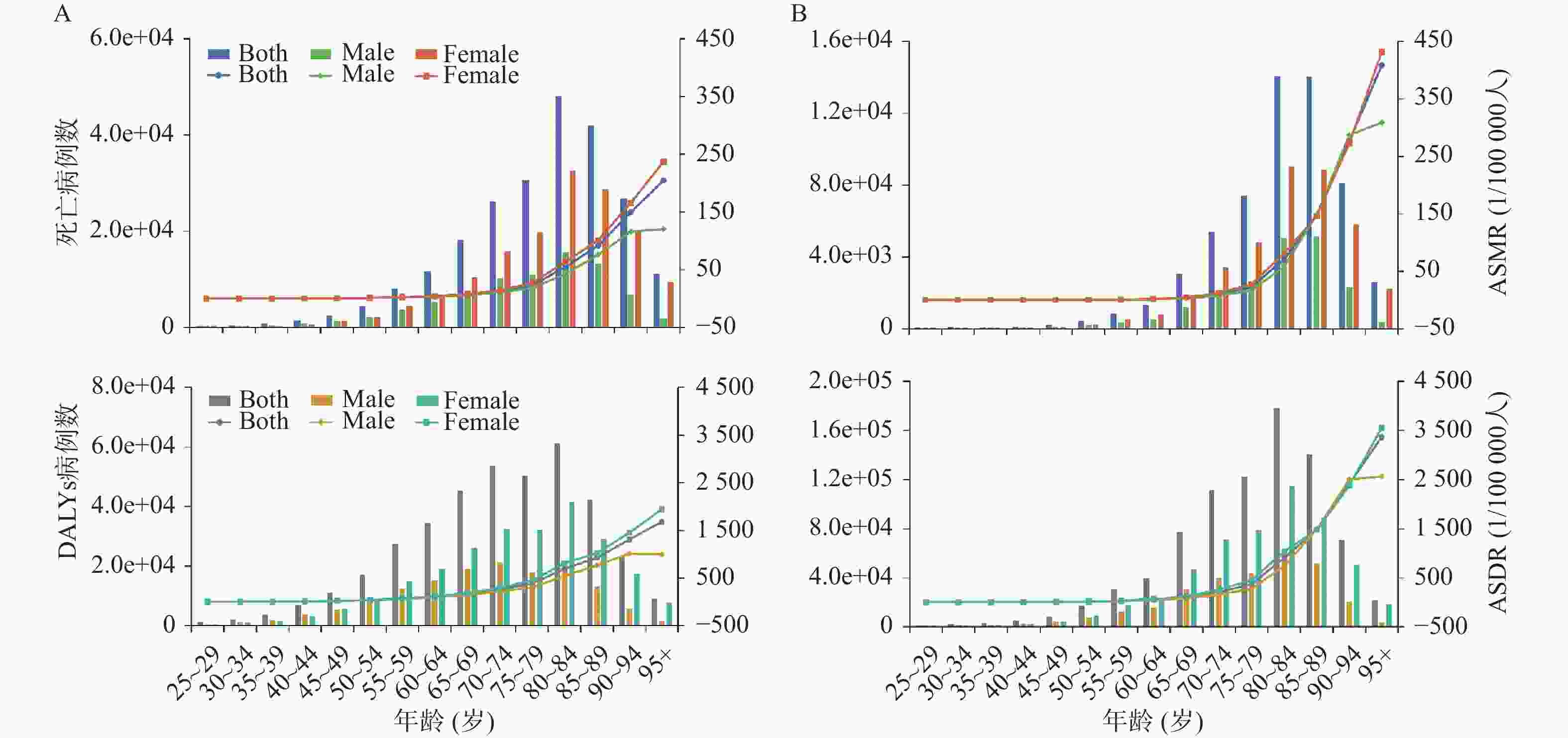
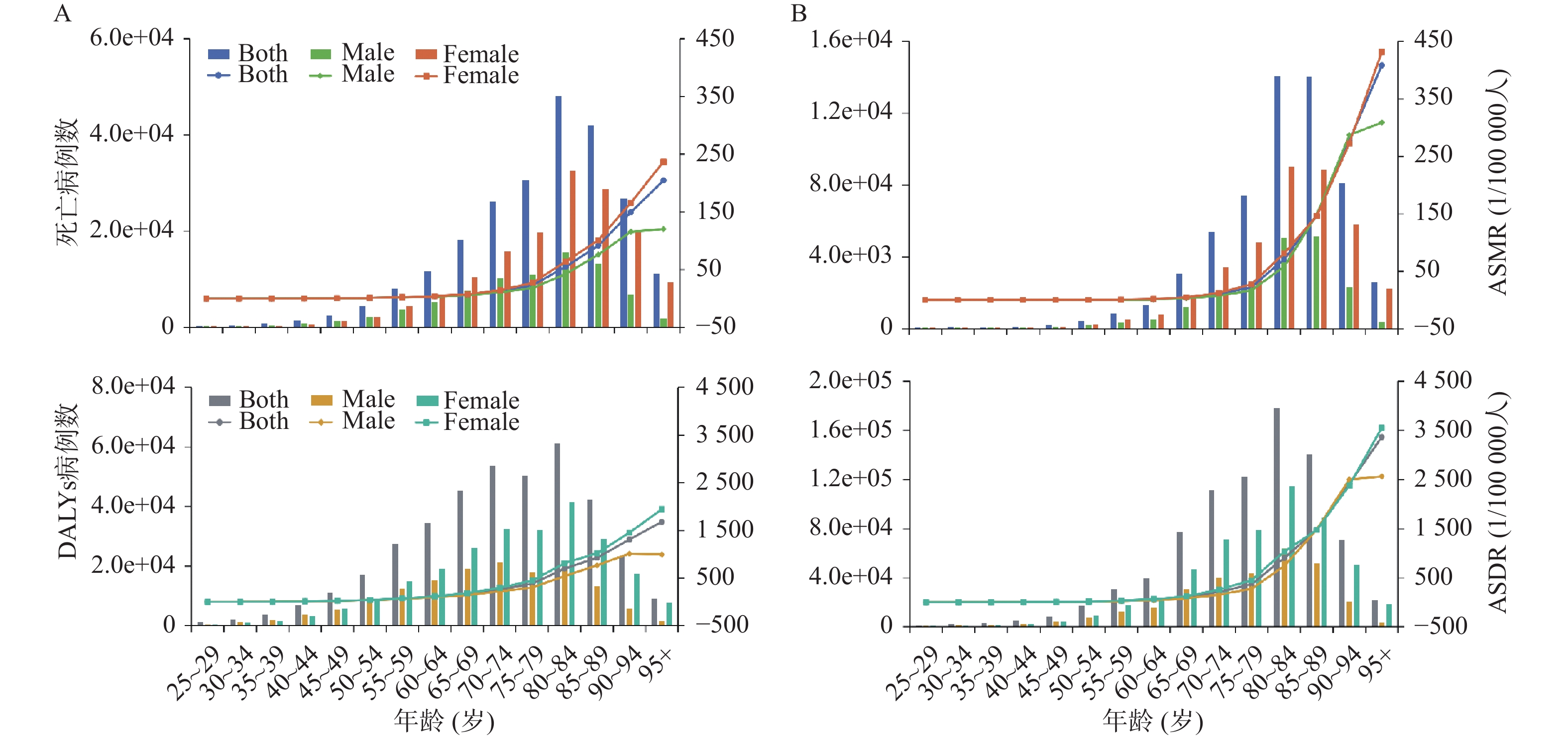
图 1 2021年全球与中国各年龄组死亡及DALYs变化趋势
A:全球变化趋势;B:中国变化趋势。
Figure 1. Trends in deaths and DALYs across age groups globally and in China,2021
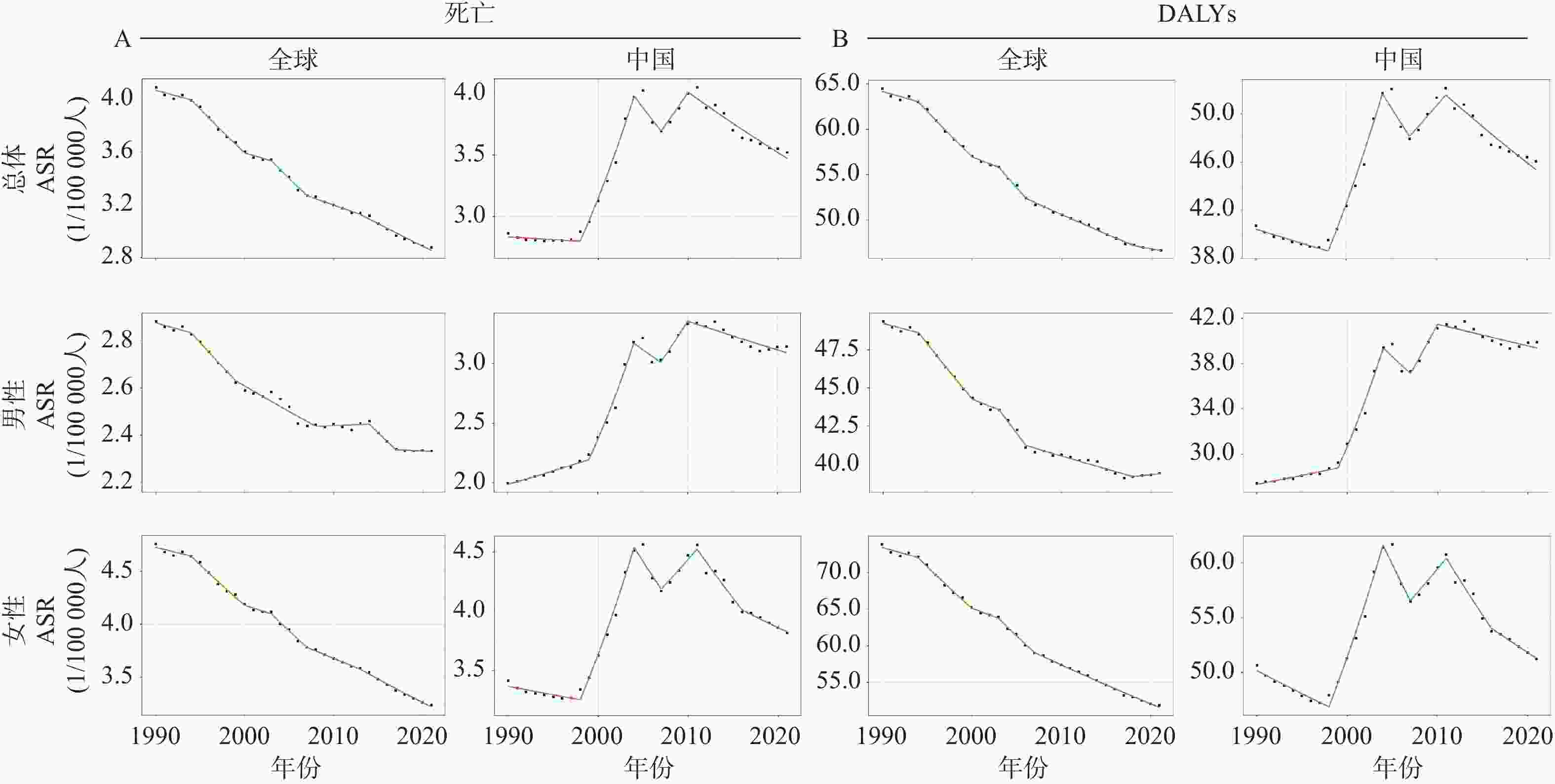
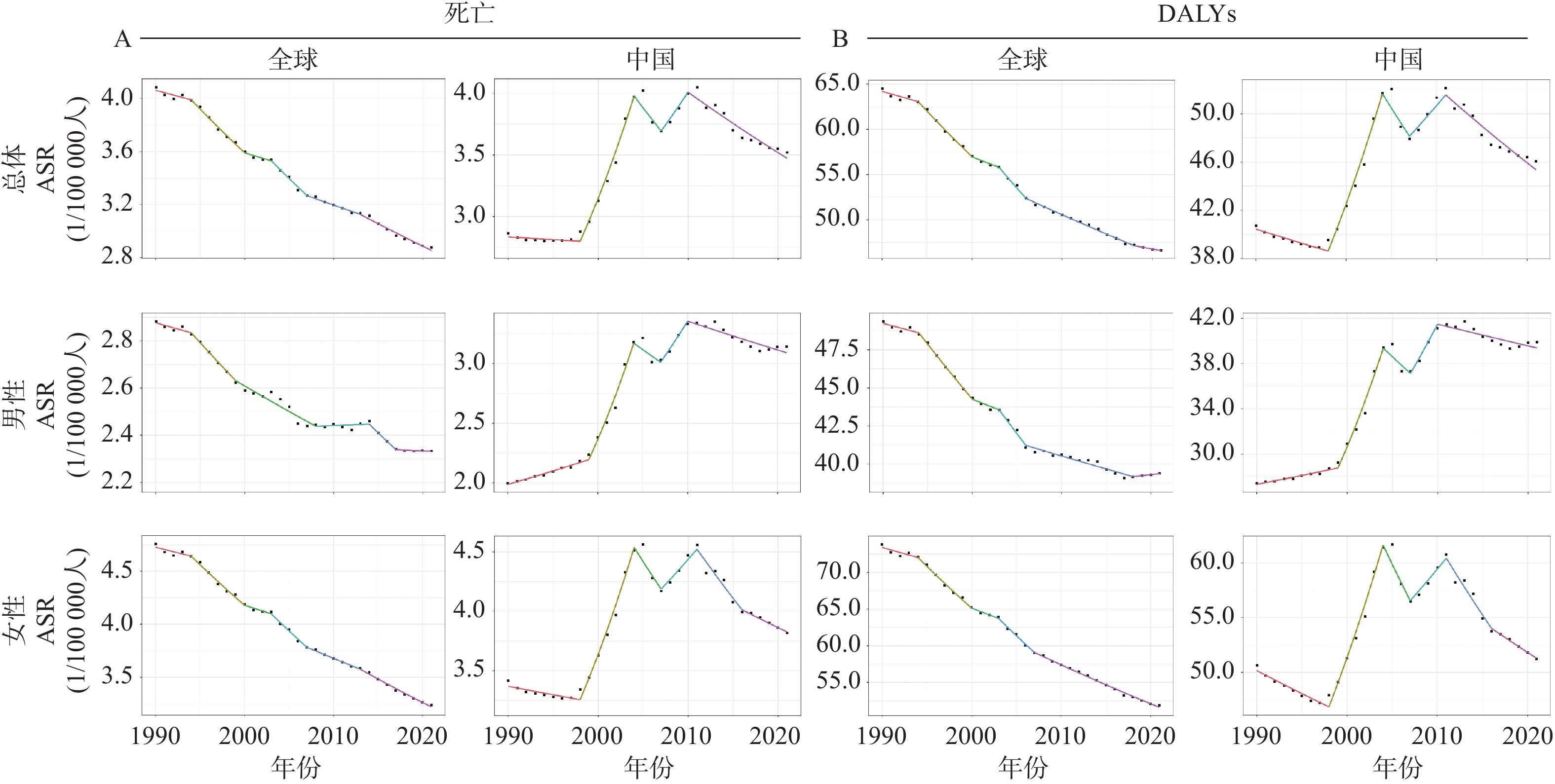
图 2 基于Joinpoint回归法分析1990—2021年全球与中国ASMR及ASDR时序演变趋势
A:全球演变趋势;B:中国演变趋势。
Figure 2. Temporal trends in ASMR and ASDR based on Joinpoint regression analysis globally and in China from 1990 to 2021
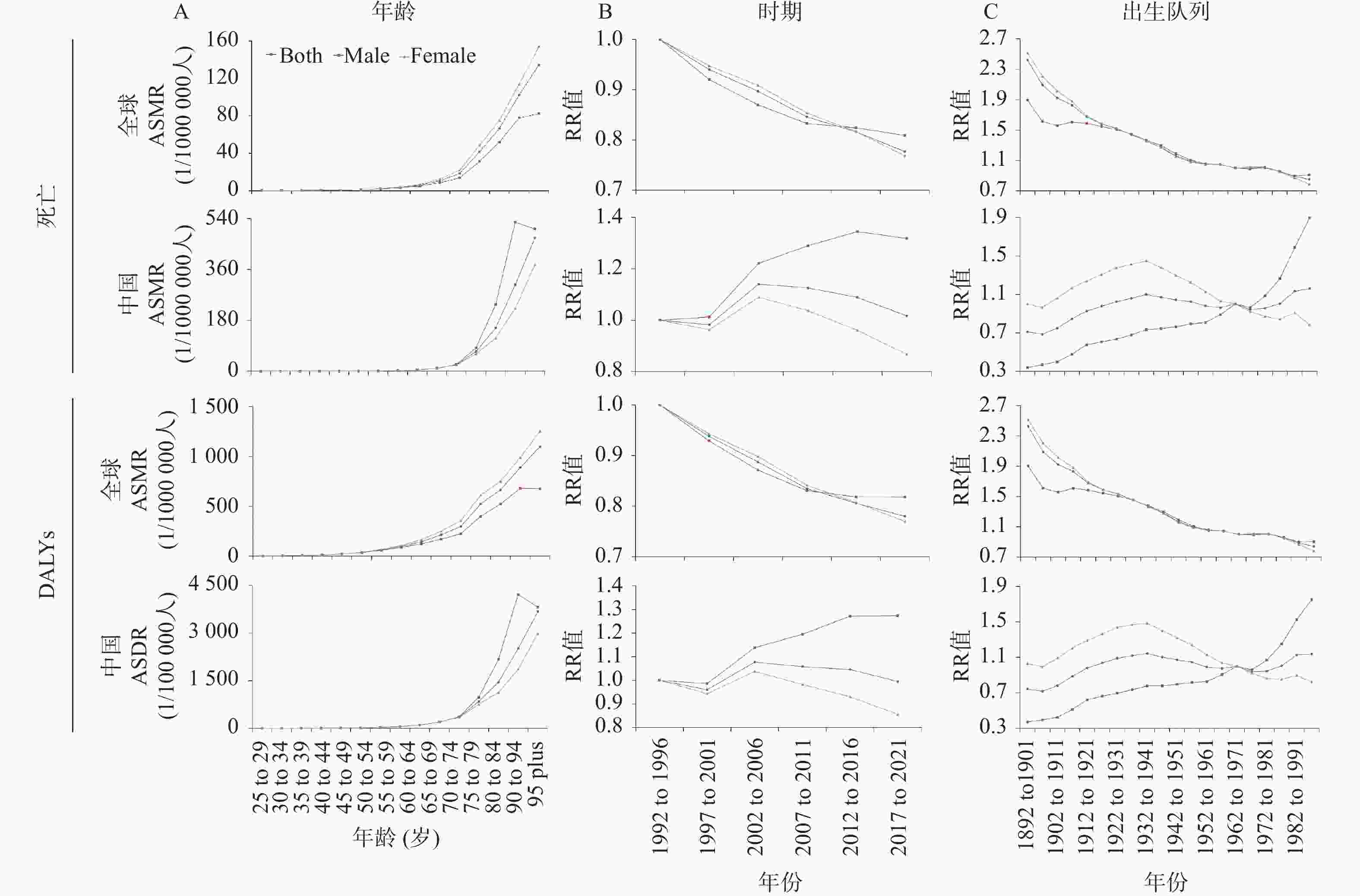
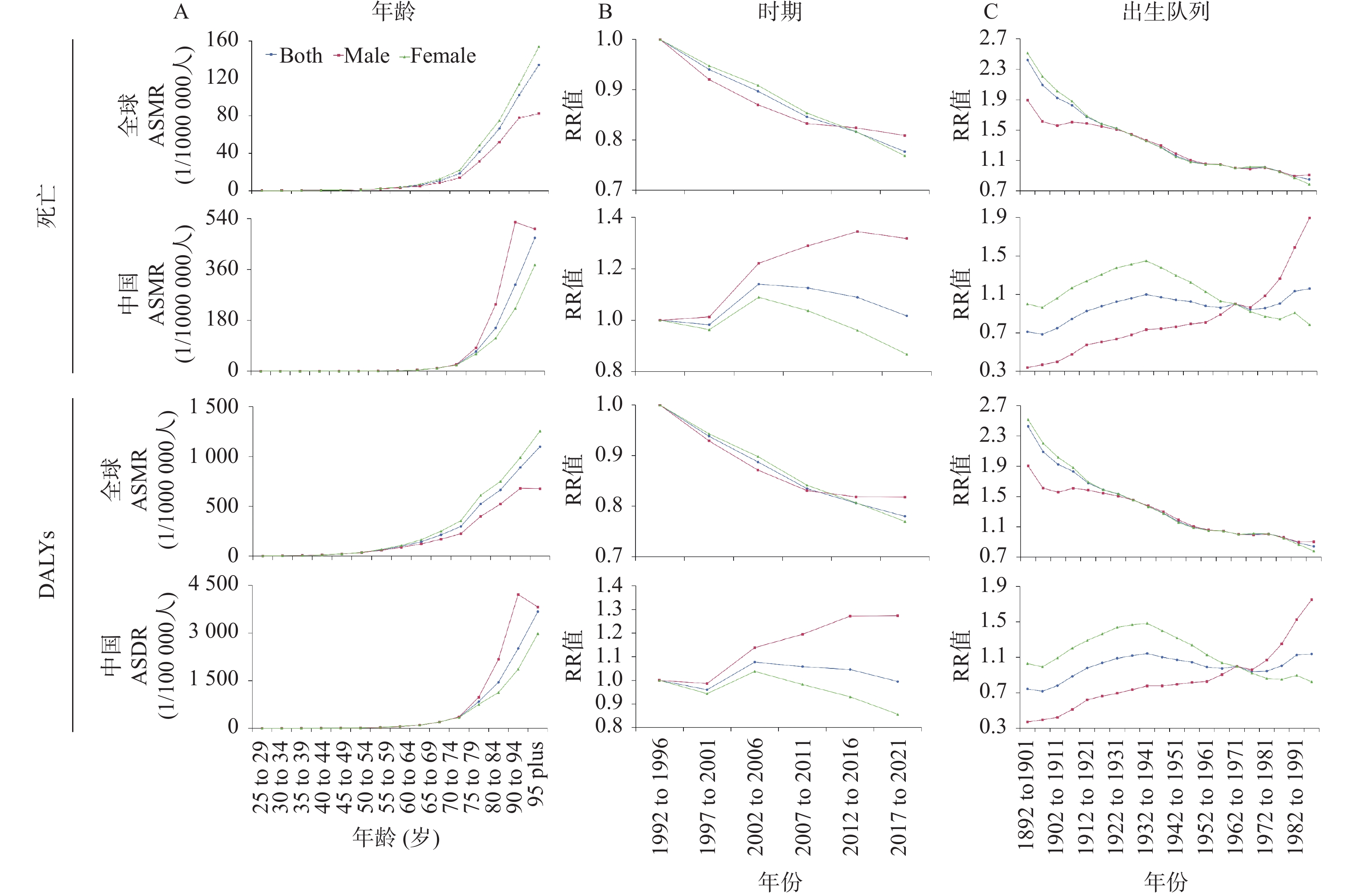
图 3 全球与中国ASMR及ASDR的年龄-时期-队列分析
A:年龄分析;B:时期分析;C:队列分析。
Figure 3. Age - period - cohort analysis of ASMR and ASDR globally and in China
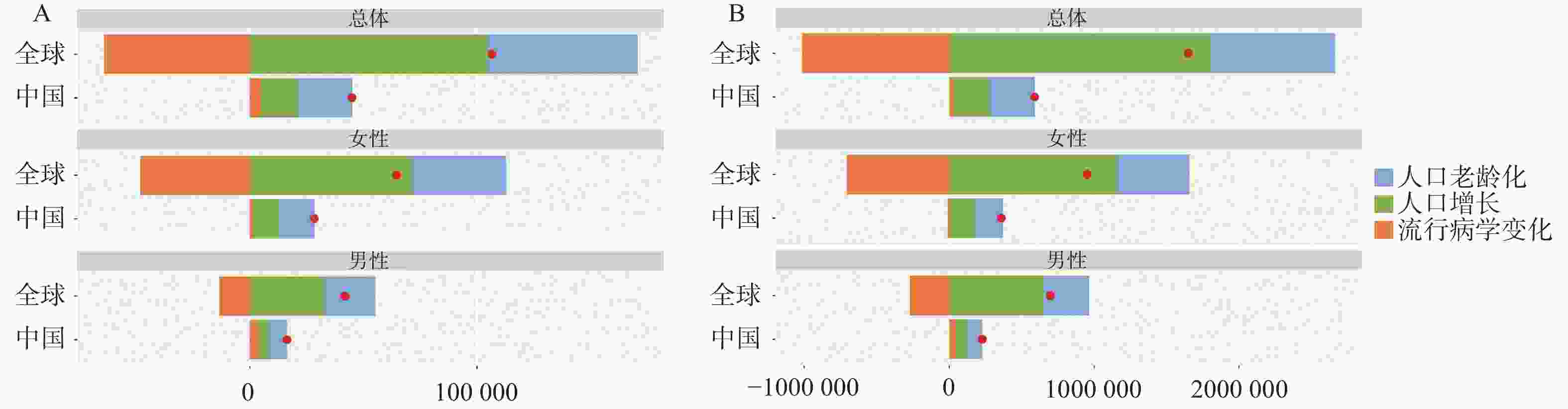
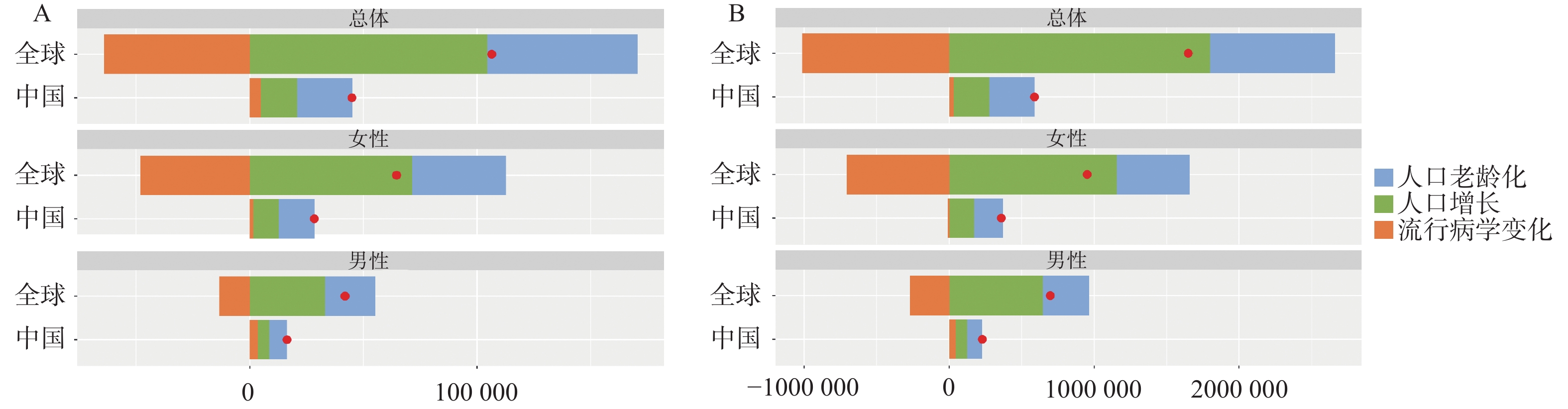
图 4 1990—2021年全球与中国死亡及DALYs的分解分析
A:死亡数的分解分析;B:DALYs数的分解分析。
Figure 4. Decomposition analysis of deaths and DALYs globally and in China,1990—2021
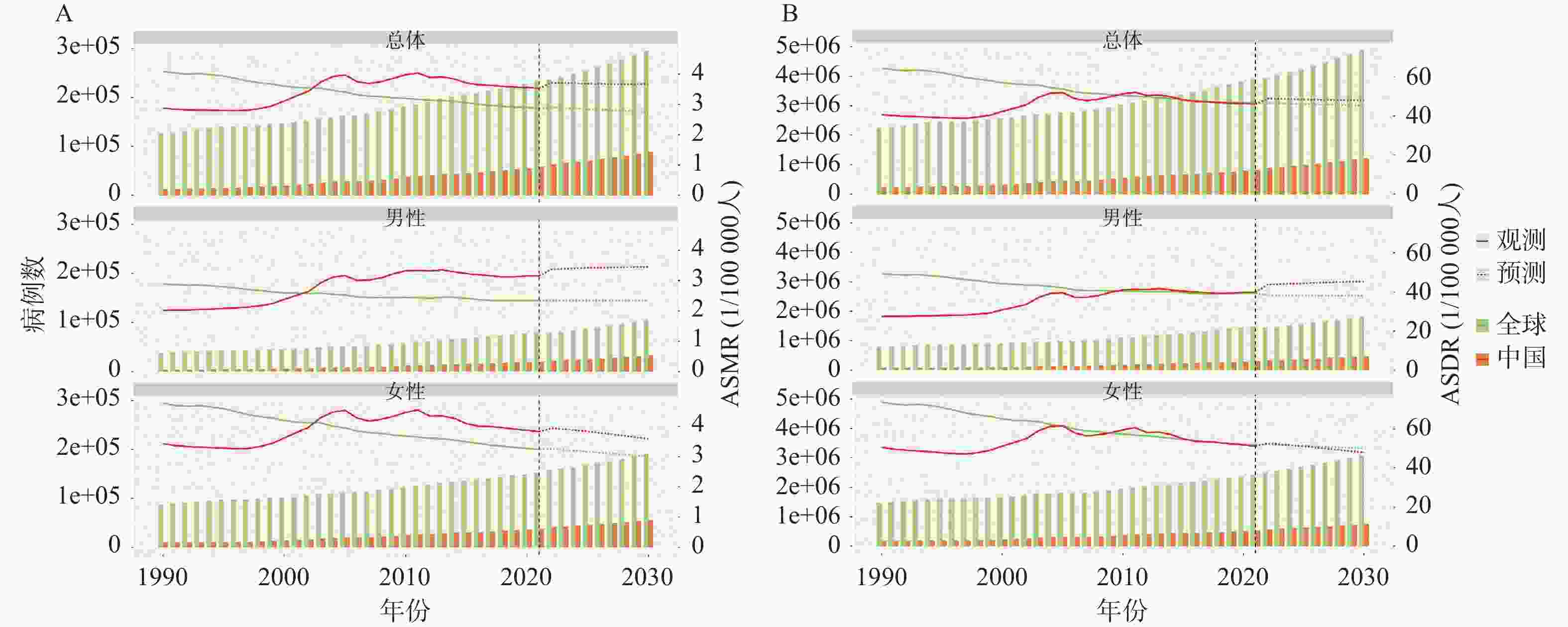
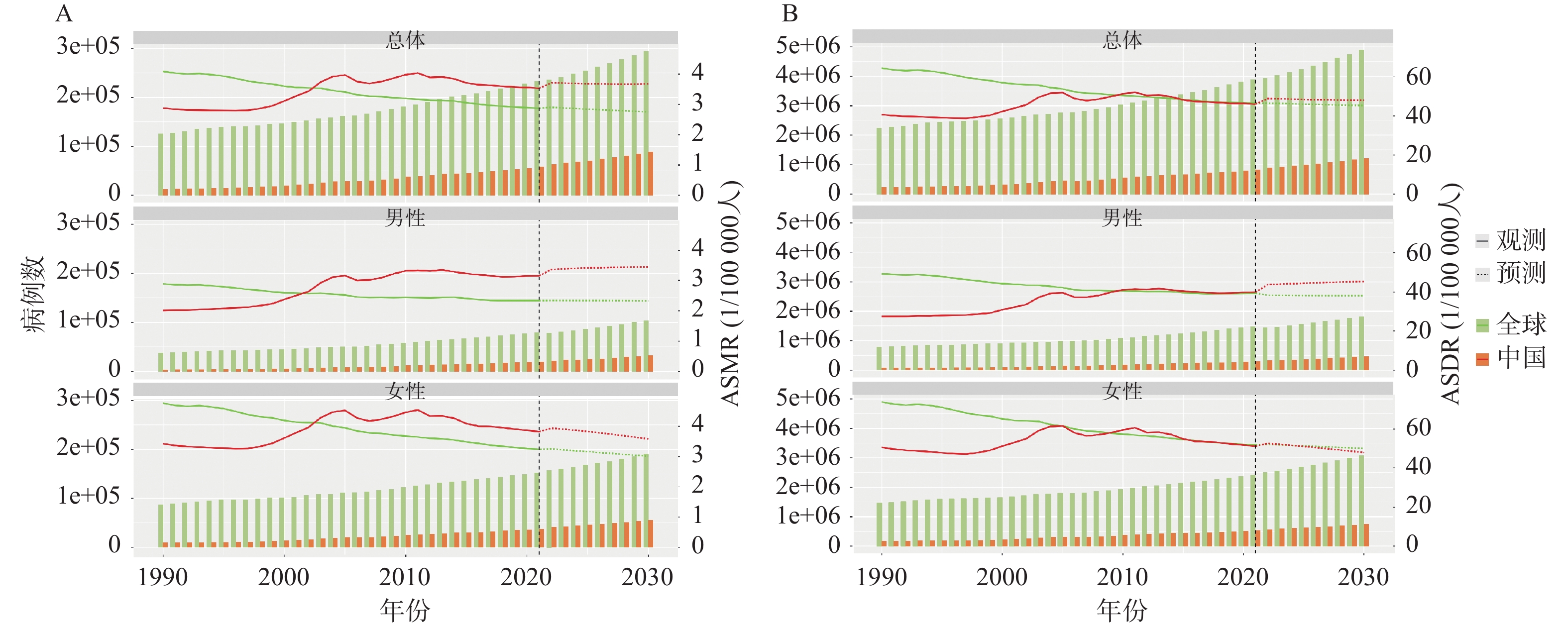
图 5 全球及中国死亡率与DALYs率2022—2030年的预测趋势
A:死亡率的预测趋势;B:DALYs率的预测趋势。
Figure 5. Projected trends in mortality and DALYs globally and in China from2022 to 2030
表 1 1990年与2021年全球和中国归因于LPA的IHD疾病负担
Table 1. Disease burden of IHD attributable to LPA globally and in China,1990 and 2021
类别 病例数(95%UI) 变化百分比 (%) ASR(1/100,000人,95%UI) EAPC
(95%CI)1990 2021 1990 2021 死亡 总体 全球 125,730 (55,488~199,339) 232,250 (103,518~371,375) 84.72 4.09 (1.78~6.56) 2.88 (1.28~4.59) -1.19 (-1.23 to -1.15) 中国 12,808 (5,227~22,545) 57,721 (23,735~106,094) 350.66 2.86 (1.12~5.37) 3.52 (1.43~6.58) 1.12 (0.78 to 1.46) 男性 全球 38,023 (16,293~60,944) 79,945 (36,705~129,067) 110.25 2.88 (1.21~4.80) 2.33 (1.07~3.82) -0.71(-0.78 to -0.65) 中国 3,478 (1,308~6,722) 19,968 (6,770~41,355) 474.12 1.99 (0.63~4.32) 3.14 (0.99~6.75) 1.88 (1.53 to 2.24) 女性 全球 87,707 (38,827~139,152) 152,305 (66,250~248,989) 73.65 4.76 (2.11~7.66) 3.24 (1.41~5.29) -1.29 (-1.32 to -1.25) 中国 9,330 (3,700~16,837) 37,753 (14,452~72,337) 304.64 3.41 (1.28~6.30) 3.82 (1.45~7.45) 0.82 (0.48 to 1.16) DALYs 总体 全球 2,248,011 (1,013,161~3,466,301) 3,897,941 (1,767,043~6,116,373) 73.40 64.51 (28.79~101.42) 446.63 ( (21.15~73.38) -1.14 (-1.19 to -1.09) 中国 237,710 (103,506~396,304) 827,789 (365,855~1,470,328) 248.23 40.72 (16.75~71.08) 46.05 (19.74~83.48) 0.80 (0.52 to 1.07) 男性 全球 785,494 (347,068~1,216,683) 1,482,151 (693,907~2,337,776) 89.69 49.36 (21.34~78.43) 39.41 (18.46~62.34) -0.83 (-0.91 to -0.75) 中国 67,960 (26,365~127,958) 298,139 (106,539~569,059) 339.70 27.40 (9.66~55.38) 39.89 (13.55~80.83) 1.54 (1.25 to 1.82) 女性 全球 1,462,516 (657,058~2,257,655) 2,415,790 (1,072,448~3,832,823) 65.18 73.85 (33.00~114.68) 51.88 (23.05~82.18) -1.22 (-1.26 to -1.18) 中国 169,751 (66,965~291,627) 529,650 (206,021~966,577) 212.02 50.65 (19.90~90.15) 51.24 (20.08~94.75) 0.44 (0.16 to 0.73)  下载: 导出CSV
下载: 导出CSV
-
[1] Mensah G A, Fuster V, Murray C J L, et al. Global burden of cardiovascular diseases and risks, 1990-2022[J]. J Am Coll Cardiol, 2023, 82(25): 2350-2473. [2] Jensen R V, Hjortbak M V, Bøtker H E. Ischemic heart disease: An update[J]. Semin Nucl Med, 2020, 50(3): 195-207. doi: 10.1053/j.semnuclmed.2020.02.007 [3] Byrne R A, Rossello X, Coughlan J J, et al. 2023 ESC Guidelines for the management of acute coronary syndromes[J]. Eur Heart J Acute Cardiovasc Care, 2024, 13(1): 55-161. [4] Tan J, Xue M, Li H, et al. Global, regional, and national burden of ischemic heart disease attributable to 25 risk factors and their summary exposure value across 204 countries with different socio-demographic index levels, 1990-2021: A systematic fixed-effects analysis and comparative study[J]. Clin Epidemiol, 2025, 17: 105-129. [5] Kraus W E, Powell K E, Haskell W L, et al. Physical activity, all-cause and cardiovascular mortality, and cardiovascular disease[J]. Med Sci Sports Exerc, 2019, 51(6): 1270-1281. [6] Vasankari V, Halonen J, Vasankari T, et al. Physical activity and sedentary behaviour in secondary prevention of coronary artery disease: A review[J]. Am J Prev Cardiol, 2021, 5: 100146. doi: 10.1016/j.ajpc.2021.100146 [7] Li Y, Chen Y, Huang K, et al. Physical activity and ischemic heart disease risk: A prospective cohort study among Chinese adults[J]. J Phys Act Health, 2025, 22(5): 546-554. doi: 10.1123/jpah.2024-0496 [8] Xu Y Y, Xie J, Yin H, et al. The global burden of disease attributable to low physical activity and its trends from 1990 to 2019: An analysis of the global burden of disease study[J]. Front Public Health, 2022, 10: 1018866. [9] 吴霞, 张译匀, 姚承志, 等. 1990—2021年中国归因于饮食因素的缺血性心脏病疾病负担变化趋势及预测研究[J]. 中国全科医学, 2025, 28(3): 305-312. doi: 10.12114/j.issn.1007-9572.2024.0253 [10] 姜璎硕, 张明慧, 贾莹, 等. 1990—2021年中国缺血性心脏病发病死亡趋势的年龄-时期-队列模型[J]. 现代医学, 2025, 53(1): 10-16. [11] 闫昱名, 付宏利, 关礼春, 等. 1990—2021年中国和全球归因于烟草的缺血性心脏病疾病负担现状及变化趋势研究[J]. 中国心血管病研究, 2025, 23(4): 366-372. [12] GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: A systematic analysis for the global burden of disease Study 2021[J]. Lancet, 2024, 403(10440): 2133-2161. [13] GBD 2021 Diseases and Injuries Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: A systematic analysis for the global burden of disease Study 2021[J]. Lancet, 2024, 403(10440): 2100-2132. doi: 10.1016/S0140-6736(24)00367-2 [14] Kyu H H, Bachman V F, Alexander L T, et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: Systematic review and dose-response meta-analysis for the global burden of disease Study 2013[J]. BMJ, 2016, 354: i3857. [15] GBD 2021 Diseases and Injuries Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2021: A systematic analysis for the global burden of disease Study 2021[J]. Lancet Neurol, 2024, 23(10): 973-1003. [16] GBD 2021 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the global burden of disease study 2019[J]. Lancet, 2020, 396(10258): 1204-1222. doi: 10.1016/S0140-6736(20)30925-9 [17] Yang C, Jia Y, Zhang C, et al. Global, regional, and national burdens of heart failure in adolescents and young adults aged 10-24 years from 1990 to 2021: An analysis of data from the global burden of disease study 2021[J]. E Clinical Medicine, 2024, 79: 102998. [18] Rosenberg P S, Check D P, Anderson W F. A web tool for age-period-cohort analysis of cancer incidence and mortality rates[J]. Cancer Epidemiol Biomarkers Prev, 2014, 23(11): 2296-2302. [19] Murray C J L. Findings from the global burden of disease study 2021[J]. Lancet, 2024, 403(10440): 2259-2262. doi: 10.1016/S0140-6736(24)00769-4 [20] Wang H, Chen H. Aging in China: Challenges and opportunities[J]. China CDC Wkly, 2022, 4(27): 601-602. [21] Chen X, Giles J, Yao Y, et al. The path to healthy ageing in China: A Peking University-Lancet Commission[J]. Lancet, 2022, 400(10367): 1967-2006. [22] 林思琪, 彭文瑶, 林鑫, 等. 中国缺血性心脏病主要危险因素的系统综述[J]. 疾病监测, 2024, 39(4): 488-496. doi: 10.3784/jbjc.202311150595 [23] Chen P, Li F, Harmer P. Healthy China 2030: Moving from blueprint to action with a new focus on public health[J]. Lancet Public Health, 2019, 4(9): e447. doi: 10.1016/S2468-2667(19)30160-4 [24] Vaccarezza M, Papa V, Milani D, et al. Sex/gender-specific imbalance in CVD: Could physical activity help to improve clinical outcome targeting CVD molecular mechanisms in women?[J]. Int J Mol Sci, 2020, 21(4): 1477. doi: 10.3390/ijms21041477 [25] Raparelli V, Proietti M, Lenzi A, et al. Sex and gender differences in ischemic heart disease: Endocrine vascular disease approach (EVA) study design[J]. J Cardiovasc Transl Res, 2020, 13(1): 14-25. doi: 10.1007/s12265-018-9846-5 [26] Liu Q, Liu F, Li J, et al. Sedentary behavior and risk of incident cardiovascular disease among Chinese adults[J]. Sci Bull (Beijing), 2020, 65(20): 1760-1766. [27] Pan F, Wang Z, Wang H, et al. Association between ultra-processed food consumption and metabolic syndrome among adults in China-results from the China health and nutrition survey[J]. Nutrients, 2023, 15(3): 752. [28] Li F. Physical activity and health in the presence of China’ s economic growth: Meeting the public health challenges of the aging population[J]. J Sport Health Sci, 2016, 5(3): 258-269. [29] 郑家鲲, 徐丽萍, 王思贝, 等. 《全民健身计划纲要》颁布30周年: 历程、成就、经验与展望[J]. 成都体育学院学报, 2024, 50(6): 8-20. [30] Fu X, Wang J, Jiang S, et al. Mortality trend analysis of ischemic heart disease in China between 2010 and 2019: A joinpoint analysis[J]. BMC Public Health, 2023, 23(1): 644. doi: 10.1186/s12889-023-15549-3 [31] Zhang C, Chen Q, Yin F, et al. Burden, trends, and predictions of low physical activity-related diseases in China: Analysis from the global burden of disease Study, 1990-2021, with projections to 2035[J]. Front Public Health, 2025, 13: 1461554. [32] Li Y, Chen Y, Huang K, et al. Physical activity and ischemic heart disease risk: A prospective cohort study among Chinese adults[J]. J Phys Act Health, 2025, 22(5): 546-554. doi: 10.1123/jpah.2024-0496 [33] Pasanen T P, Lanki T, Siponen T, et al. What makes a liveable neighborhood? Role of socio-demographic, dwelling, and environmental factors and participation in finnish urban and suburban areas[J]. J Urban Health, 2024, 101(6): 1207-1220. doi: 10.1007/s11524-024-00927-y [34] Abedi A, Verma A, Jain D, et al. AI-driven real-time monitoring of cardiovascular conditions with wearable devices: scoping review[J]. JMIR Mhealth Uhealth, 2025, 13: e73846. doi: 10.2196/73846 [35] Li Q, Cai W, Li Y, et al. Effects of a theory-based exercise intervention on physical activity levels and health-related outcomes in older people with chronic diseases[J]. Geriatr Gerontol Int, 2023, 23(2): 78-84. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 711
- HTML全文浏览量: 519
- PDF下载量: 157
- 被引次数: 0
