

Prediction of Major Adverse Cardiovascular Events Following PCI in NSTEMI Patients Using Combined Myocardial Contrast Echocardiography and Three-dimensional Speckle Tracking Imaging
-
摘要:
目的 探讨心肌超声造影心动图(myocardial contrast echocardiography,MCE)联合三维斑点追踪成像(three-dimensional speckle tracking imaging,3D-STI)对非ST段抬高型心肌梗死(non-ST-segment elevation myocardial infarction,NSTEMI)患者经皮冠状动脉介入治疗(percutaneous coronary intervention,PCI)术后主要心血管不良事件(major adverse cardiovascular events,MACEs)的预测作用。 方法 选取2022年5月至2024年3月中国人民解放军联勤保障部队第九二八医院254例NSTEMI患者,行PCI术,根据出院1年内MACEs发生情况分为MACEs组(n = 63)、无MACEs组(n = 191),比较两组临床资料、常规超声心动图参数、MCE参数[平台期峰值强度(peak intensity,A)、灌注计分指数(perfusion score index,PSI)、曲线斜率(beta value,β)、心肌血流量(myocardial blood flow,A·β)]及3D-STI参数[左室整体面积应变(left ventricular global area strain,LVGAS)、左室整体环向应变(left ventricular global circumferential strain,LVGCS)、左室整体纵向应变(left ventricular global longitudinal strain,LVGLS)、左室整体径向应变(left ventricular global radial strain,LVGRS)]的差异;分析MCE、3D-STI参数与左室射血分数(left ventricular ejection fraction,LVEF)的关系;以受试者工作特征(receiver operating characteristic,ROC)曲线分析MCE、3D-STI参数预测MACEs的价值。 结果 与无MACEs组相比,MACEs组N末端脑钠肽前体(N-terminal pro-brain natriuretic peptide,NT-proBNP)、白介素-6(interleukin-6,IL-6)、可溶性生长刺激表达基因2蛋白(soluble suppression of tumorigenicity 2,sST2)较高,LVEF、血管内皮生长因子(vascular endothelial growth factor,VEGF)较低(P < 0.05);术后3个月与无MACEs组相比,MACEs组A、β、A·β较低,PSI较高,两组A、PSI、β、A·β术后3个月-术后24 h差值比较差异有统计学意义(P < 0.05);术后3个月MACEs组LVGAS、LVGCS、LVGLS、LVGRS均低于无MACEs组,两组LVGAS、LVGCS、LVGLS、LVGRS术后3个月-术后24 h差值比较差异有统计学意义(P < 0.05);术后3个月MCE、3D-STI参数联合预测MACEs的AUC为0.933(95%CI:0.895~0.961),术后3个月-术后24 h MCE、3D-STI参数差值联合预测MACEs的AUC为0.915(95%CI:0.873~0.946)。 结论 MCE、3D-STI定量参数联合对NSTEMI患者PCI术后MACEs风险有较高预测价值,监测术后3个月-术后24 h MCE及3D-STI参数的动态变化,有助于早期识别高风险患者,为制定个体化治疗与随访策略提供依据。 -
关键词:
- 非ST段抬高型心肌梗死 /
- 心肌超声造影心动图 /
- 三维斑点追踪成像 /
- 经皮冠状动脉介入治疗 /
- 主要心血管不良事件
Abstract:Objective To investigate the predictive value of myocardial contrast echocardiography (MCE) combined with three-dimensional speckle tracking imaging (3D-STI) for major adverse cardiovascular events (MACEs) following percutaneous coronary intervention (PCI) in patients with non-ST-segment elevation myocardial infarction (NSTEMI). Methods A total of 254 NSTEMI patients who underwent PCI at the 928th Hospital of the Joint Logistics Support Force, People's Liberation Army from May 2022 to March 2024 were selected. Patients were stratified into MACEs group and non-MACEs group based on the occurrence of MACEs within one year of discharge. Clinical data, conventional echocardiographic parameters, MCE parameters [peak intensity (A), perfusion score index (PSI), curve slope (β) and myocardial blood flow (A·β)] and 3D-STI parameters [left ventricular global area strain (LVGAS), left ventricular global circumferential strain (LVGCS), left ventricular global longitudinal strain (LVGLS), left ventricular global radial strain (LVGRS)] were compared between the two groups. The relationships between MCE, 3D-STI parameters and left ventricular ejection fraction (LVEF) were analyzed. Receiver operating characteristic (ROC) curve were used to assess the predictive value of MCE and 3D-STI parameters for MACEs. Results Compared with the non-MACEs group, the MACEs group had higher levels of N-terminal pro-brain natriuretic peptide (NT-proBNP), interleukin-6 (IL-6), and soluble suppression of tumorigenicity 2 (sST2), with lower LVEF and vascular endothelial growth factor (VEGF) levels (P < 0.05). At 3 months post-operatively, the MACEs group showed lower A, β, A·β values, and higher PSI compared with the non-MACEs group, with significant differences in the changes of A, PSI, β, A·β from 3 months to 24 hours post-operatively between groups (P < 0.05). At 3 months post-operatively, LVGAS, LVGCS, LVGLS and LVGRS were all lower in the MACEs group than in the non-MACEs group, with significant differences in the changes of these parameters from 3 months to 24 hours post-operatively (P < 0.05). The combined AUC of MCE and 3D-STI parameters at 3 months post-operatively for predicting MACEs was 0.933 (95%CI: 0.895–0.961), and the combined AUC using the differences in MCE and 3D-STI parameters between 3 months and 24 hours post-operatively was 0.915 (95%CI: 0.873~0.946). Conclusion The combined quantitative parameters of MCE and 3D-STI demonstrate high predictive value for MACEs risk following PCI in NSTEMI patients. Monitoring dynamic changes in MCE and 3D-STI parameters from 3 months to 24 hours post-operatively is helpful for early identification of high-risk patients and provides evidence for developing individualized therapeutic and follow-up strategies. -
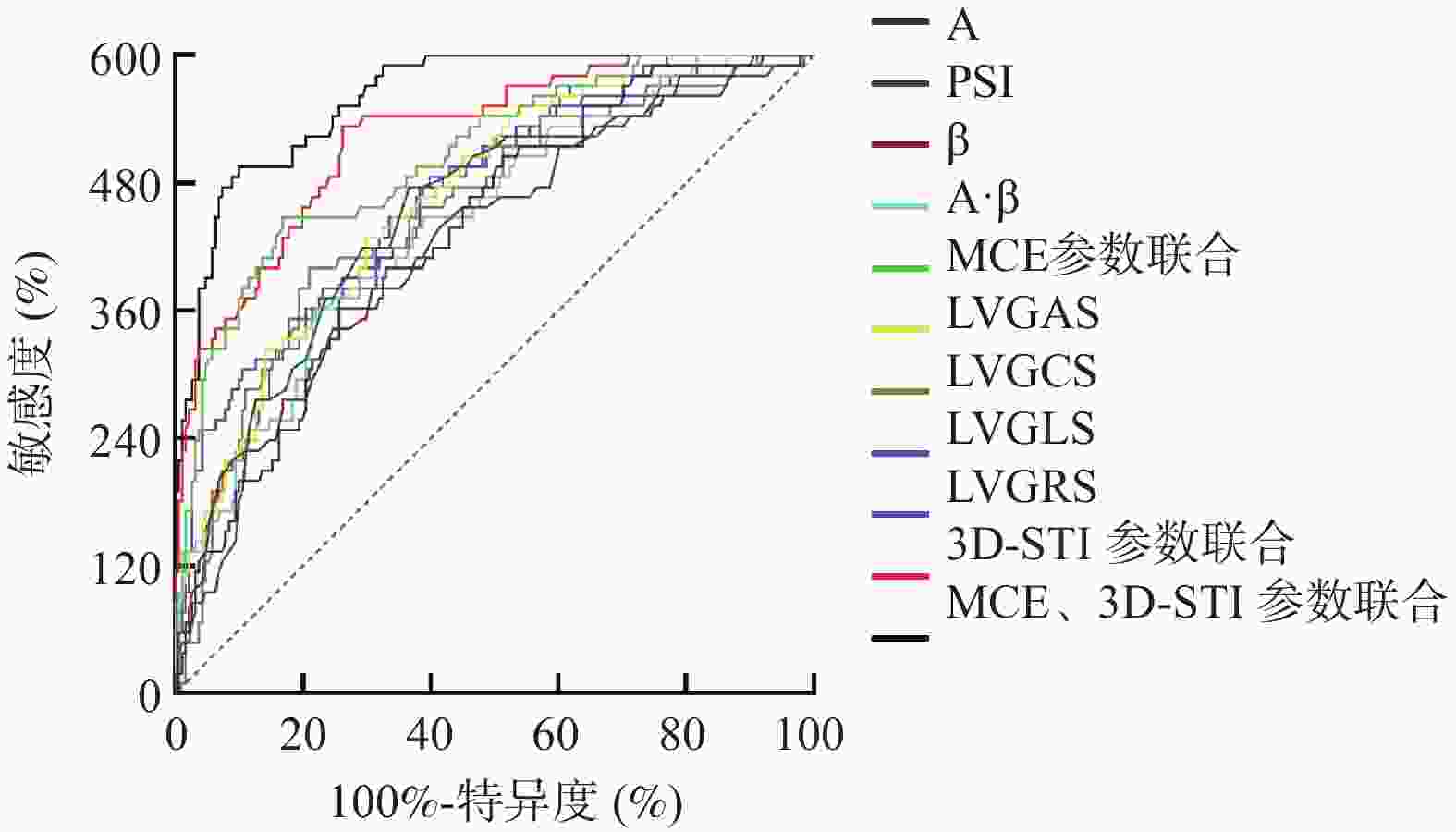
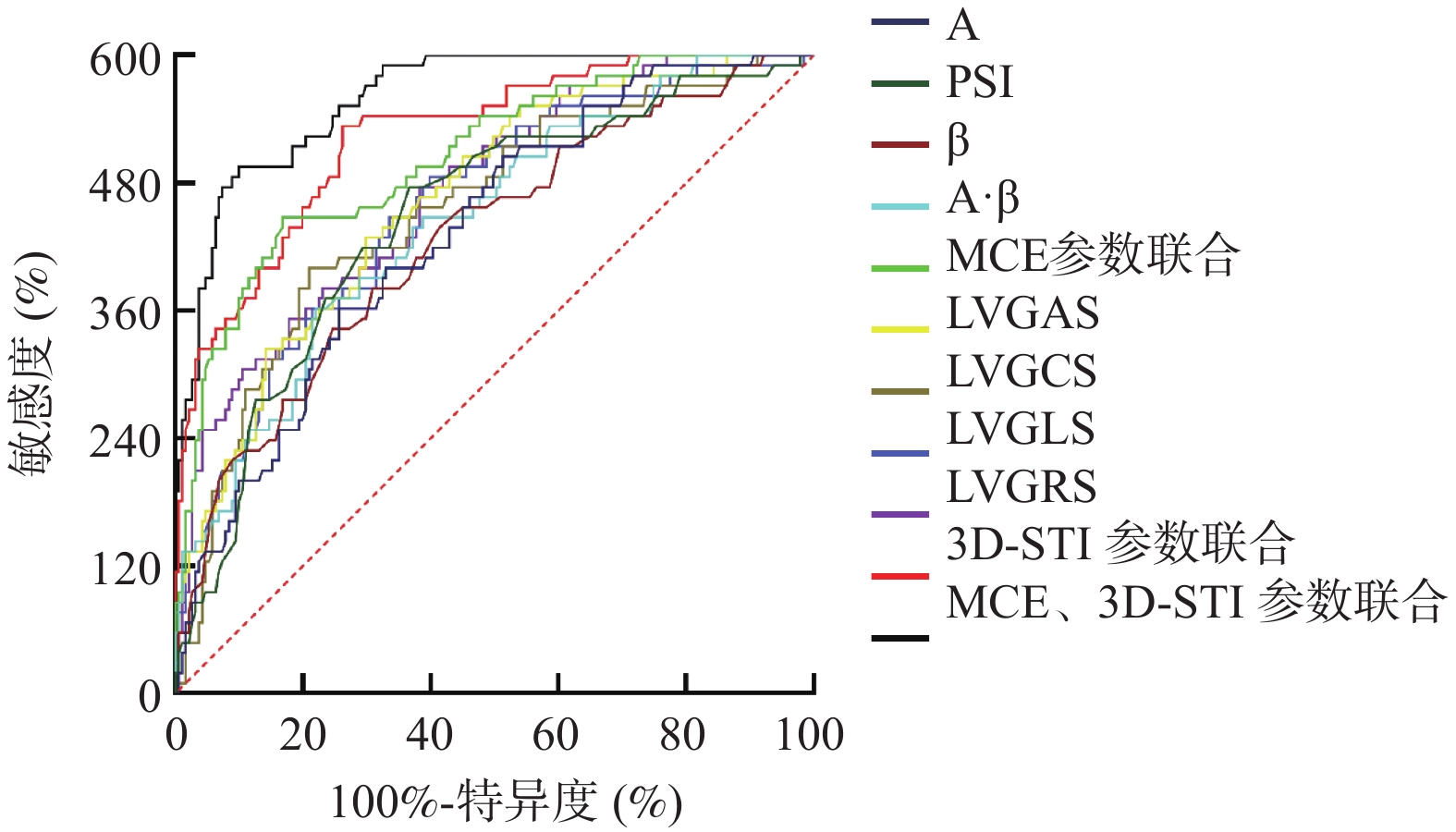
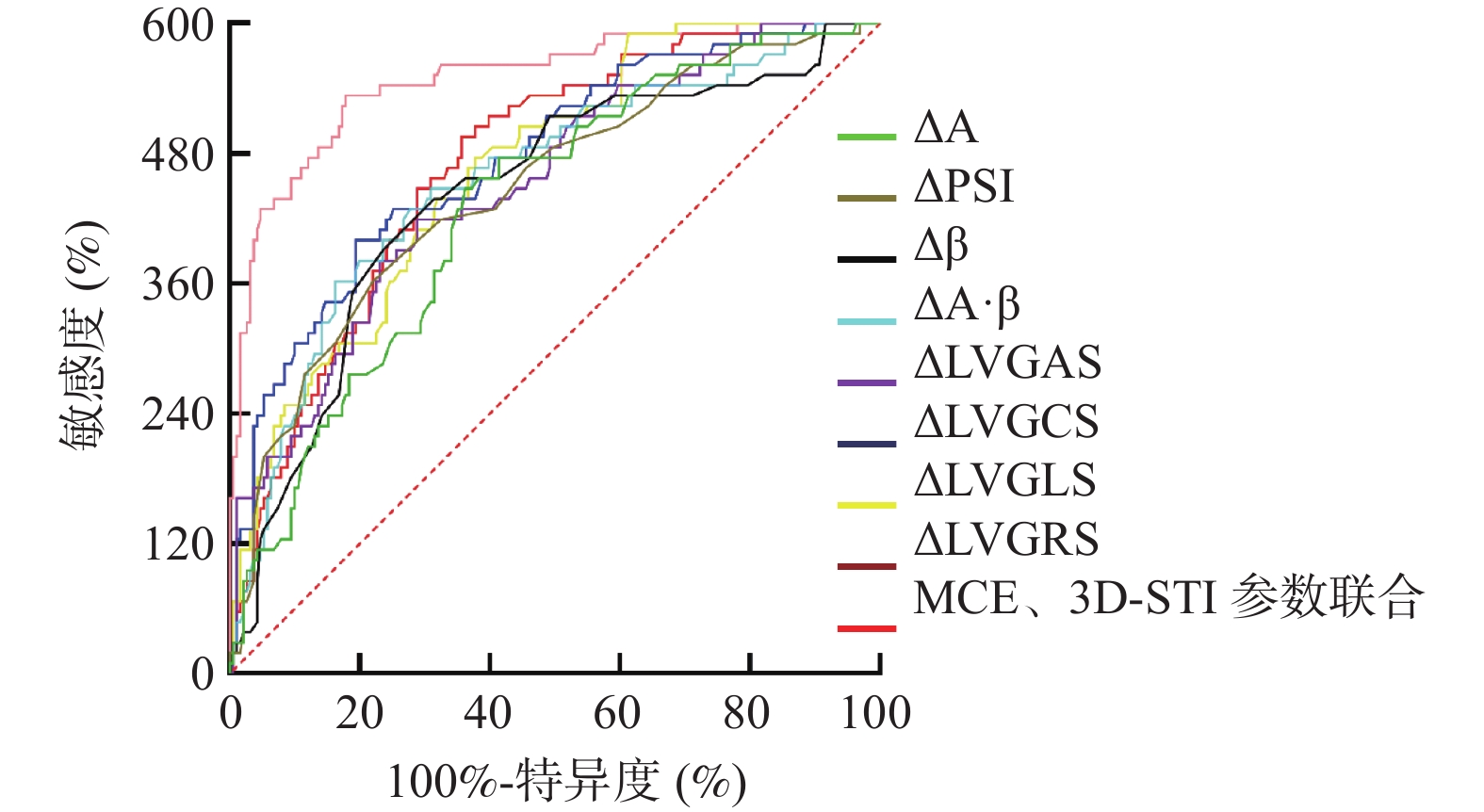
图 3 术后3个月MCE、3D-STI预测NSTEMI患者PCI术后MACEs风险的ROC曲线
Figure 3. ROC curve of MCE and 3D-STI at 3 months after PCI to predict the risk of MACEs in NSTEMI patients after PCI
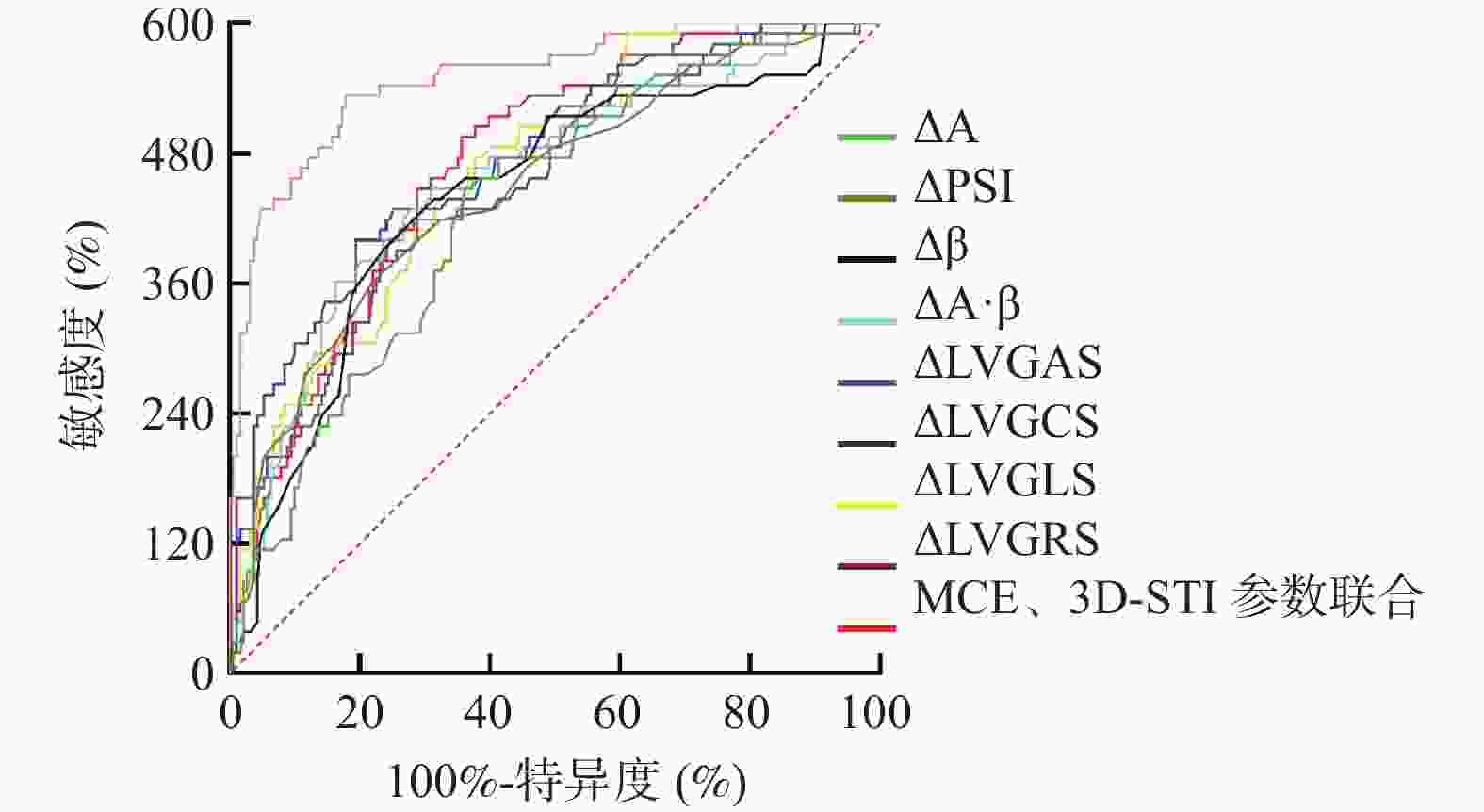
图 4 MCE、3D-STI参数动态变化预测NSTEMI患者PCI术后MACEs风险的ROC曲线
Figure 4. ROC curve of dynamic changes of MCE and 3D-STI parameters in predicting the risk of MACEs after PCI in NSTEMI patients
表 1 两组一般资料与临床特征比较[n(%)/($ \bar x \pm s $)]
Table 1. Comparison of general data and clinical characteristics between the two groups [n(%)/($ \bar x \pm s $)]
资料 MACEs组(n = 63) 无MACEs组(n = 191) χ2/t P 性别(男/女) 37(58.73)/26(41.27) 102(53.40)/89(46.60) 0.543 0.461 年龄(岁) 63.18 ± 5.69 61.59 ± 5.83 1.888 0.060 体质量指数(kg/m2) 23.86 ± 1.13 24.11 ± 1.09 −1.564 0.119 高血压 30(47.62) 86(45.03) 0.128 0.720 糖尿病 18(28.57) 47(24.61) 0.391 0.532 血脂异常 25(39.68) 64(33.51) 0.794 0.373 吸烟 26(41.27) 67(35.07) 0.782 0.376 饮酒 19(30.16) 48(25.13) 0.617 0.432 发病至PCI术时间(h) 3.72 ± 0.64 3.61 ± 0.58 1.272 0.205 病变支数(支) 1.026 0.311 1 21(33.33) 51(26.70) ≥2 42(66.67) 140(73.30)  下载: 导出CSV
下载: 导出CSV
表 2 两组药物治疗及手术情况比较[n(%)/($\bar x \pm s $)]
Table 2. Comparison of drug treatment and surgical conditions between the two groups [n(%)/($\bar x \pm s $)]
资料 MACEs组(n = 63) 无MACEs组(n = 191) χ2/t P 药物治疗情况 他汀类药物 60(95.24) 186(97.38) 0.184 0.668 抗血小板 58(92.06) 183(95.81) 0.707 0.400 β受体阻滞剂 43(68.25) 136(71.20) 0.198 0.656 ACEI/ARB 51(80.95) 160(83.77) 0.267 0.605 手术情况 支架长度(mm) 25.18 ± 6.87 23.34 ± 7.10 1.798 0.073 支架直径(mm) 2.53 ± 0.72 2.67 ± 0.65 −1.443 0.150
下载: 导出CSV
表 3 两组实验室指标及超声心动图参数比较($\bar x \pm s $)
Table 3. Comparison of laboratory indicators and echocardiographic parameters between the two groups ($\bar x \pm s $)
资料 MACEs组(n = 63) 无MACEs组(n = 191) χ2/t P 实验室指标 NT-proBNP(ng/L) 448.91 ± 126.18 305.49 ± 93.65 9.620 < 0.001* IL-6(pg/mL) 14.57 ± 3.23 9.86 ± 2.42 12.268 < 0.001* sST2(ng/mL) 27.41 ± 7.75 22.16 ± 5.91 5.636 < 0.001* VEGF(pg/mL) 153.34 ± 31.25 185.67 ± 35.28 −6.481 < 0.001* 常规超声心动图参数 LVEF(%) 53.74 ± 5.02 56.81 ± 4.63 −4.468 < 0.001* LVEDV(mL) 149.41 ± 34.92 147.63 ± 40.15 0.315 0.753 *P < 0.05。
下载: 导出CSV
表 4 两组MCE参数比较($ \bar x \pm s $)
Table 4. Comparison of MCE parameters between the two groups ($ \bar x \pm s $)
参数 MACEs组(n = 63) 无MACEs组(n = 191) t P A(dB) 术后24 h 8.23 ± 2.25 8.34 ± 2.18 −0.345 0.731 术后3个月 10.62 ± 1.94 12.19 ± 2.05 −5.340 < 0.001* 差值 2.39 ± 0.58 3.85 ± 1.12 −9.909 < 0.001* PSI 术后24 h 1.74 ± 0.52 1.81 ± 0.49 −0.968 0.334 术后3个月 1.42 ± 0.20 1.25 ± 0.21 5.637 < 0.001* 差值 −0.32 ± 0.08 −0.56 ± 0.12 14.815 < 0.001* β(dB/s) 术后24 h 1.21 ± 0.31 1.18 ± 0.34 0.620 0.536 术后3个月 1.49 ± 0.24 1.68 ± 0.33 −4.215 < 0.001* 差值 0.28 ± 0.08 0.50 ± 0.10 −15.861 < 0.001* A·β 术后24 h 9.96 ± 2.54 9.84 ± 2.49 0.330 0.742 术后3个月 15.82 ± 2.92 20.48 ± 4.03 −8.469 < 0.001* 差值 5.86 ± 1.31 10.64 ± 2.17 −16.507 < 0.001* *P < 0.05。
下载: 导出CSV
表 5 两组3D-STI参数比较[($ \bar x \pm s $)%]
Table 5. Comparison of 3D-STI parameters between the two groups [($ \bar x \pm s $)%]
参数 MACEs组(n = 63) 无MACEs组(n = 191) t P LVGAS 术后24 h −18.25 ± 4.36 −18.91 ± 4.54 1.010 0.313 术后3个月 −24.36 ± 5.83 −31.60 ± 7.49 7.001 < 0.001* 差值 −6.11 ± 1.73 −12.39 ± 3.54 13.544 < 0.001* LVGCS 术后24 h −12.59 ± 3.40 −13.04 ± 6.63 0.516 0.606 术后3个月 −16.75 ± 4.16 −22.67 ± 5.63 7.679 < 0.001* 差值 −4.16 ± 1.08 −9.63 ± 2.13 19.553 < 0.001* LVGLS 术后24 h −10.81 ± 2.75 −11.24 ± 2.69 1.094 0.275 术后3个月 −14.49 ± 3.57 −19.71 ± 4.88 7.823 < 0.001* 差值 −3.68 ± 1.03 −8.47 ± 1.25 27.483 < 0.001* LVGRS 术后24 h 23.17 ± 6.10 23.84 ± 6.38 −0.731 0.466 术后3个月 30.55 ± 7.61 39.47 ± 9.82 −6.584 < 0.001* 差值 7.38 ± 1.36 15.63 ± 4.71 −13.699 < 0.001* *P < 0.05。
下载: 导出CSV
表 6 术后3个月MCE、3D-STI对NSTEMI患者PCI术后MACEs风险的预测价值
Table 6. Predictive value of MCE and 3D-STI at three months after PCI for MACEs risk in NSTEMI patients after PCI
参数 AUC 95%CI 截断值 敏感度(%) 特异度(%) P MCE A 0.722 0.662~0.776 11.41 dB 60.32 74.35 < 0.001* PSI 0.744 0.686~0.796 1.34 79.39 63.35 < 0.001* β 0.712 0.652~0.767 1.59 dB/s 63.49 69.11 < 0.001* A·β 0.739 0.680~0.792 18.15 60.32 78.01 < 0.001* 3D-STI LVGAS 0.775 0.718~0.825 −26.94% 71.43 70.16 < 0.001* LVGCS 0.757 0.699~0.808 −17.59% 66.67 79.06 < 0.001* LVGLS 0.764 0.707~0.815 −17.26% 80.95 60.21 < 0.001* LVGRS 0.786 0.730~0.835 36.26% 79.39 61.78 < 0.001* *P < 0.05。
下载: 导出CSV
表 7 各联合方案的预测价值分析
Table 7. Analysis of predictive value for various combination therapies
参数 AUC 95%CI 敏感度(%) 特异度(%) 阳性预测值(%) 阴性预测值(%) 阳性似然比 阴性似然比 MCE参数联合 0.841 0.790~0.884 74.60 83.25 49.73 93.86 4.45 0.30 3D-STI参数联合 0.874 0.827~0.912 88.89 73.82 45.22 96.15 3.40 0.15 MCE、3D-STI参数联合 0.933 0.895~0.961 82.54 90.05 65.39 95.49 8.29 0.19
下载: 导出CSV
表 8 术后3个月-术后24 h MCE、3D-STI参数差值对MACEs风险的预测价值
Table 8. Predictive value of MCE and 3D-STI parameter difference between 3 months and 24 hours after operation for MACEs risk
指标差值 AUC 95%CI 截断值 敏感度(%) 特异度(%) P MCE △A 0.718 0.658~0.773 3.12 dB 74.60 63.87 < 0.001* △PSI 0.745 0.687~0.797 −0.44 60.32 78.01 < 0.001* △β 0.737 0.679~0.790 0.39 dB/s 73.02 68.59 < 0.001* △A·β 0.761 0.704~0.812 8.25 60.32 83.77 < 0.001* 3D-STI △LVGAS 0.751 0.694~0.803 −9.25% 69.84 71.20 < 0.001* △LVGCS 0.792 0.737~0.840 −6.89% 66.67 80.63 < 0.001* △LVGLS 0.776 0.719~0.826 −6.08% 79.37 62.30 < 0.001* △LVGRS 0.784 0.728~0.833 11.51% 82.54 64.40 < 0.001* MCE、3D-STI参数差值联合 0.915 0.873~0.946 − 88.89 82.20 < 0.001* 注:△值 = 术后3个月值-术后24 h值;*P < 0.05。
下载: 导出CSV
-
[1] 张国勇, 马铮, 刘佩林, 等. 非ST段抬高型心肌梗死患者经皮冠状动脉介入治疗后病理性Q波持续状态与预后的关系[J]. 中国医药, 2024, 19(3): 321-325. [2] Lee M, Kim D W, Park M W, et al. Multivessel versus IRA-only PCI in patients with NSTEMI and severe left ventricular systolic dysfunction[J]. PLoS One, 2021, 16(10): e0258525. doi: 10.1371/journal.pone.0258525 [3] Jenab Y, Hedayat B, Karimi A, et al. Effects of opium use on one-year major adverse cardiovascular events (MACE) in the patients with ST-segment elevation MI undergoing primary PCI: A propensity score matched - machine learning based study[J]. BMC Complement Med Ther, 2023, 23(1): 16. doi: 10.1186/s12906-023-03833-z [4] Gong X, Zhang T, Feng S, et al. Association between N-terminal pro-BNP and 12 months major adverse cardiac events among patients admitted with NSTEMI[J]. Ann Palliat Med, 2021, 10(5): 5231-5243. doi: 10.21037/apm-20-2538 [5] Kim Y H, Her A Y, Rha S W, et al. Three-year outcomes following non-ST-segment elevation myocardial infarction and new-generation drug-eluting stent implantation, stratified by patient age (under and over 75 years) and left ventricular ejection fraction: A prospective cohort study[J]. Medicine, 2024, 103(37): e39606. doi: 10.1097/MD.0000000000039606 [6] Capdeville S, Gholson B A, Lindner J R. Contrast echocardiography for assessing myocardial perfusion[J]. Curr Cardiol Rep, 2023, 25(11): 1581-1587. doi: 10.1007/s11886-023-01970-y [7] Chen F, Weng W, Yang D, et al. Myocardial contrast echocardiography evaluation of coronary microvascular dysfunction to predict MACEs in patients with heart failure with preserved ejection fraction follow-up[J]. BMC Cardiovasc Disord, 2024, 24(1): 496. doi: 10.1186/s12872-024-04173-7 [8] 吉洪花, 吴雨歌, 侯冬梅, 等. 超声斑点追踪技术在肥厚型心肌病患者心功能评估及心肌纤维化预测中的作用[J]. 临床误诊误治, 2023, 36(1): 61-64. doi: 10.3969/j.issn.1002-3429.2023.01.014 [9] 杨璐, 李丽, 王呼日, 等. 血清DJ-1、Kallistatin、TP53联合检测对急性心肌梗死患者PCI术后主要不良心血管事件的预测价值[J]. 疑难病杂志, 2026, 25(1): 14-18. doi: 10.3969/j.issn.1671-6450.2026.01.003 [10] 中国医师协会急诊医师分会, 国家卫健委能力建设与继续教育中心急诊学专家委员会, 中国医疗保健国际交流促进会急诊急救分会. 急性冠脉综合征急诊快速诊治指南(2019)[J]. 临床急诊杂志, 2019, 20(4): 253-262. [11] Zheng J J, Si Y Q, Xia T Y, et al. Optimal timing of invasive intervention for high-risk non-ST-segment-elevation myocardial infarction patients[J]. J Geriatr Cardiol, 2024, 21(8): 807-815. doi: 10.26599/1671-5411.2024.08.003 [12] Zhang W, Jia H, Zhao X, et al. Predictive value of cumulative SII for MACE in STEMI patients after PCI[J]. Medicine, 2025, 104(13): e41983. doi: 10.1097/MD.0000000000041983 [13] 吉思, 宴君, 陈其敬, 等. 血清CyPA、SDF-1及LMR水平与老年ACS患者PCI治疗后再发心肌梗死的相关性[J]. 临床和实验医学杂志, 2023, 22(4): 342-346. doi: 10.3969/j.issn.1671-4695.2023.04.002 [14] 韩福星, 王高频. 沙库巴曲缬沙坦通过调控H-FABP、NT-proBNP和LVEF对心力衰竭伴房颤患者心功能、心室重构的影响[J]. 中国老年学杂志, 2025, 45(3): 517-521. doi: 10.3969/j.issn.1005-9202.2025.03.002 [15] Roldan P, Ravi S, Hodovan J, et al. Myocardial contrast echocardiography assessment of perfusion abnormalities in hypertrophic cardiomyopathy[J]. Cardiovasc Ultrasound, 2022, 20(1): 23. doi: 10.1186/s12947-022-00293-2 [16] Kim H, Kim I C, Hwang J, et al. Surveillance of adenosine stress myocardial contrast echocardiography following percutaneous coronary intervention[J]. Int J Cardiovasc Imaging, 2022, 38(9): 1909-1918. doi: 10.1007/s10554-022-02583-2 [17] 王俊伟, 杜利军, 王旭, 等. 心肌声学造影结合应变率成像技术评价急性心肌梗死PCI术后1年内再入院风险的临床价值[J]. 中西医结合心脑血管病杂志, 2025, 23(1): 94-99. doi: 10.12102/j.issn.1672-1349.2025.01.015 [18] 汤勇, 罗裕, 颜艳, 等. 心肌声学造影对急性心肌梗死患者存活心肌及经皮冠状动脉介入术后临床预后的评估价值[J]. 心脑血管病防治, 2024, 24(9): 9-14. doi: 10.3969/j.issn.1009-816x.2024.09.003 [19] Zhang J, Guan L, Li X, et al. Value of myocardial contrast echocardiography in detecting coronary microcirculatory dysfunction in ischemia with non-obstructive coronary artery disease[J]. Ultrasound Med Biol, 2023, 49(9): 2089-2094. doi: 10.1016/j.ultrasmedbio.2023.05.014 [20] 韩卫卫, 胡钦, 翟珊, 等. 超声心肌声学造影定量与冠状动脉血流参数在冠心病诊断中的应用[J]. 临床误诊误治, 2022, 35(3): 64-68. [21] Qin W, Tian R, Feng J, et al. Three-dimensional speckle tracking echocardiography to evaluate left ventricular function in patients with acute ST-segment elevation myocardial infarction after percutaneous coronary intervention following Tongxinluo treatment[J]. J Clin Ultrasound, 2022, 50(9): 1229-1239. doi: 10.1002/jcu.23279 [22] Cho E J. Clinical implication (application) of measurement of LV function by three-dimensional speckle-tracking echocardiography: Three-dimensional myocardial strain for the prediction of clinical events in patients with ST-segment elevation myocardial infarction[J]. J Cardiovasc Imaging, 2022, 30(3): 197-201. doi: 10.4250/jcvi.2022.0059 [23] Iwahashi N, Kirigaya J, Gohbara M, et al. Global strain measured by three-dimensional speckle tracking echocardiography is a useful predictor for 10-year prognosis after a first ST-elevation acute myocardial infarction[J]. Circ J, 2021, 85(10): 1735-1743. doi: 10.1253/circj.CJ-21-0183 [24] 田园, 闫媛媛, 史海宏. 超声心动图联合三维斑点追踪成像技术对心肌淀粉样变和肥厚型心肌病的诊断价值[J]. 新乡医学院学报, 2024, 41(9): 840-846. [25] Iwahashi N, Horii M, Kirigaya J, et al. Clinical usefulness of the serial examination of three-dimensional global longitudinal strain after the onset of ST-elevation acute myocardial infarction[J]. Circ J, 2022, 86(4): 611-619. doi: 10.1253/circj.CJ-21-0815 [26] 张蓉, 薛鹏, 郭华. 三维斑点追踪技术预测心肌梗死患者经皮冠状动脉介入术后发生主要心脏不良事件的临床价值[J]. 临床超声医学杂志, 2023, 25(11): 930-935. doi: 10.3969/j.issn.1008-6978.2023.11.018 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 269
- HTML全文浏览量: 155
- PDF下载量: 135
- 被引次数: 0
