

Expression Levels of t-PA,TN-C and Cav-1 in Patients with Different Clinical Outcomes after Decompressive Craniectomy for Massive Cerebral Infarction
-
摘要:
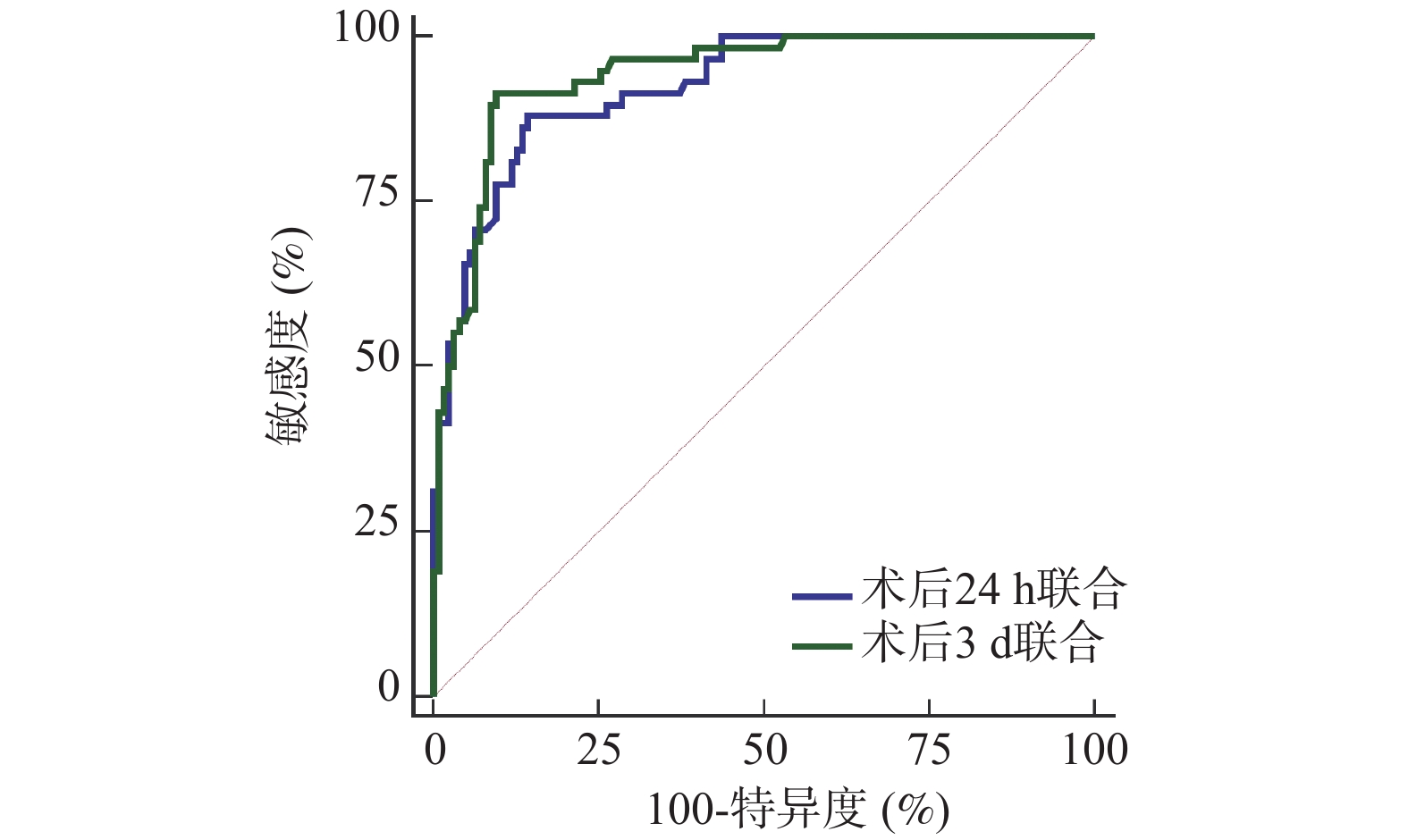
目的 分析大面积脑梗死去骨瓣减压术后不同病情转归患者组织型纤溶酶原激活物(tissue-type plasminogen activator,t-PA)、肌腱蛋白C(tenascin C,TN-C)、陷窝蛋白1(caveolin-1,Cav-1)表达水平。 方法 选取2021年1月—2024年10月北京朝阳中西医结合急诊抢救医院收治的184例拟行去骨瓣减压术的大面积脑梗死患者作为研究对象,根据术后3个月病情转归情况分为不良组(n = 58)、良好组(n = 126)。比较两组基线资料[格拉斯哥昏迷评分法(glasgow coma scale,GCS)、美国国立卫生研究院卒中量表(National Institute of Health stroke scale,NIHSS)评分等]、术后24 h、术后3 d的t-PA、TN-C、Cav-1水平及其变化值,多因素Logistic回归方程分析围手术期t-PA、TN-C、Cav-1变化值对病情转归的影响,受试者工作特征曲线(receiver operating characteristic,ROC)分析围手术期t-PA、TN-C、Cav-1变化值预测病情转归价值。 结果 不良组术前GCS评分低于良好组,术前NIHSS评分高于良好组(P < 0.05);不良组术后24 h、术后3 d的△t-PA、△TN-C、△Cav-1低于良好组(均P < 0.05);多因素分析显示,校正了GCS评分、NIHSS评分后,术后24 h、术后3 d的△t-PA、△TN-C、△Cav-1仍是大面积脑梗死去骨瓣减压术后病情转归的相关影响因素(均P < 0.05);ROC分析显示,与术后24 h比较,术后3 d的t-PA、TN-C、Cav-1变化值的ROC下面积(area under the curve,AUC)更大,预测价值更高,且术后3 d △t-PA+△TN-C+△Cav-1的AUC为0.960,显著高于术后24 h三者联合(Z = 2.735,P = 0.044),预测不良病情转归价值更高,其敏感度为91.38%,特异度为90.48%。 结论 大面积脑梗死去骨瓣减压术后不同病情转归患者t-PA、TN-C、Cav-1表达水平明显不同,联合检测三者术后3 d变化情况对病情转归预测价值更高。 Abstract:Objective To analyze the expression levels of tissue-type plasminogen activator (t-PA), tenascin C (TN-C) and caveolin-1 (Cav-1) in patients with different clinical outcomes after decompressive craniectomy for massive cerebral infarction. Methods A total of 184 patients scheduled for decompressive craniectomy due to massive cerebral infarction at Beijing Chaoyang Emergency Medical Center for Integrated Traditional Chinese and Western Medicine from January 2021 to October 2024 were selected as the research objects. According to the outcomes of the disease 3 months after operation, they were divided into a poor outcome group (n = 58) and a good outcome group (n = 126). Baseline data [glasgow coma scale (GCS), national Institute of Health stroke scale (NIHSS)score, etc.], the levels of t-PA, TN-C and Cav-1 at 24 h and 3 d after operation and their change values were compared between the two groups. Multivariate Logistic regression equation was used to analyze the effect of perioperative changes in t-PA, TN-C and Cav-1 on the outcome of the disease. Receiver operating characteristic curve (ROC) was used to analyze the value of perioperative changes of t-PA, TN-C and Cav-1 in predicting the outcome of the disease. Results The preoperative GCS score of the poor group was lower than that of the good group, and the preoperative NIHSS score was higher than that of the good group (P < 0.05). The △t-PA, △TN-C and △Cav-1 values 24 hours and 3 days postoperatively were lower in the poor outcome group than those in the good group (all P < 0.05). Multivariate analysis showed that after adjusting for GCS score and NIHSS score, the △t-PA, △TN-C and △Cav-1 values 24 hours and 3 days operation were still related factors affecting the outcome of large area cerebral infarction after decompressive craniectomy ( all P < 0.05). ROC analysis demonstrated that the area under the curve (AUC) for predicting outcome was greater for the biomarker changes measured at 3 days postoperatively compared to those at 24 hours, indicating higher predictive value. Specifically, the combined AUC for ∆t-PA + ∆TN-C + ∆Cav-1 at 3 days postoperatively was 0.960, which was significantly higher than the combined AUC for the 24-hour measurements (Z = 2.735, P = 0.044), showing superior value in predicting poor clinical outcomes with a sensitivity of 91.38% and a specificity of 90.48%. Conclusion The expression levels of t-PA, TN-C and Cav-1 in patients with different disease outcomes after decompressive craniectomy for massive cerebral infarction are significantly different. Combined detection of the changes in these three biomarkers, particularly at 3 days after operation has a higher predictive value for clinical outcome. -
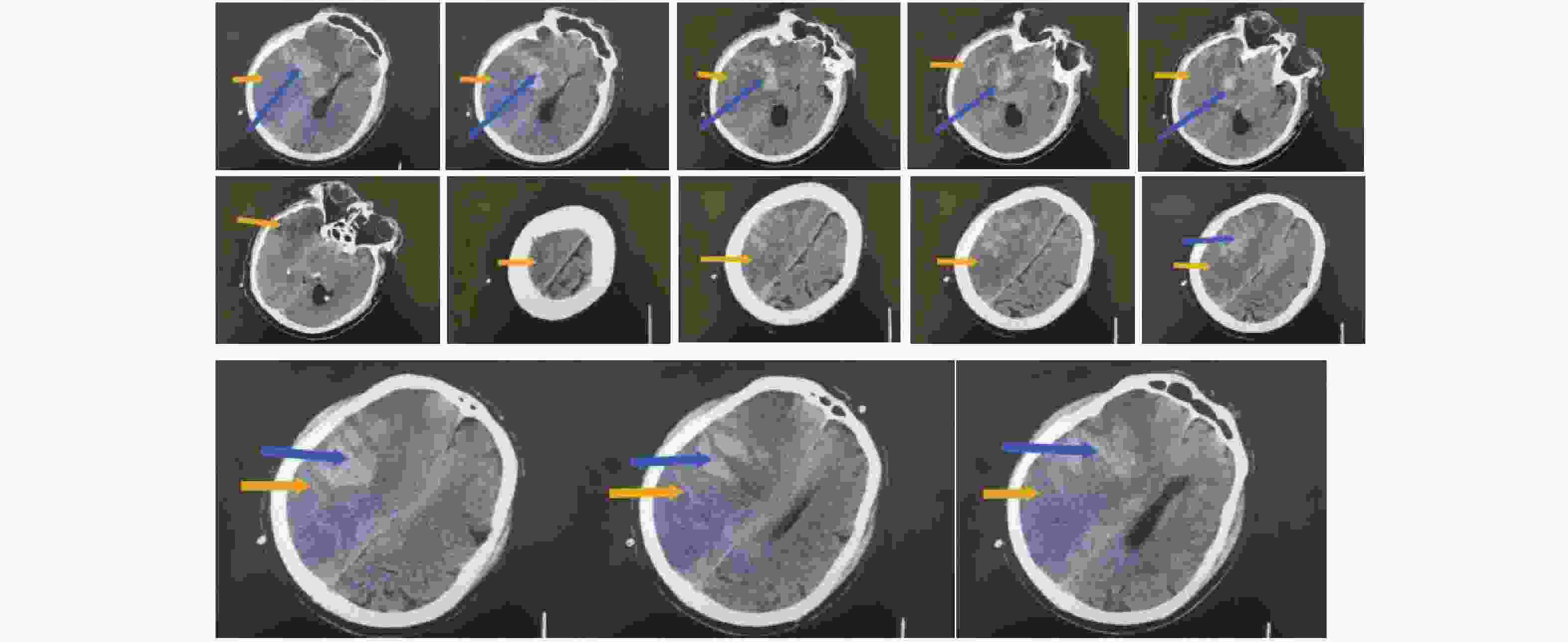
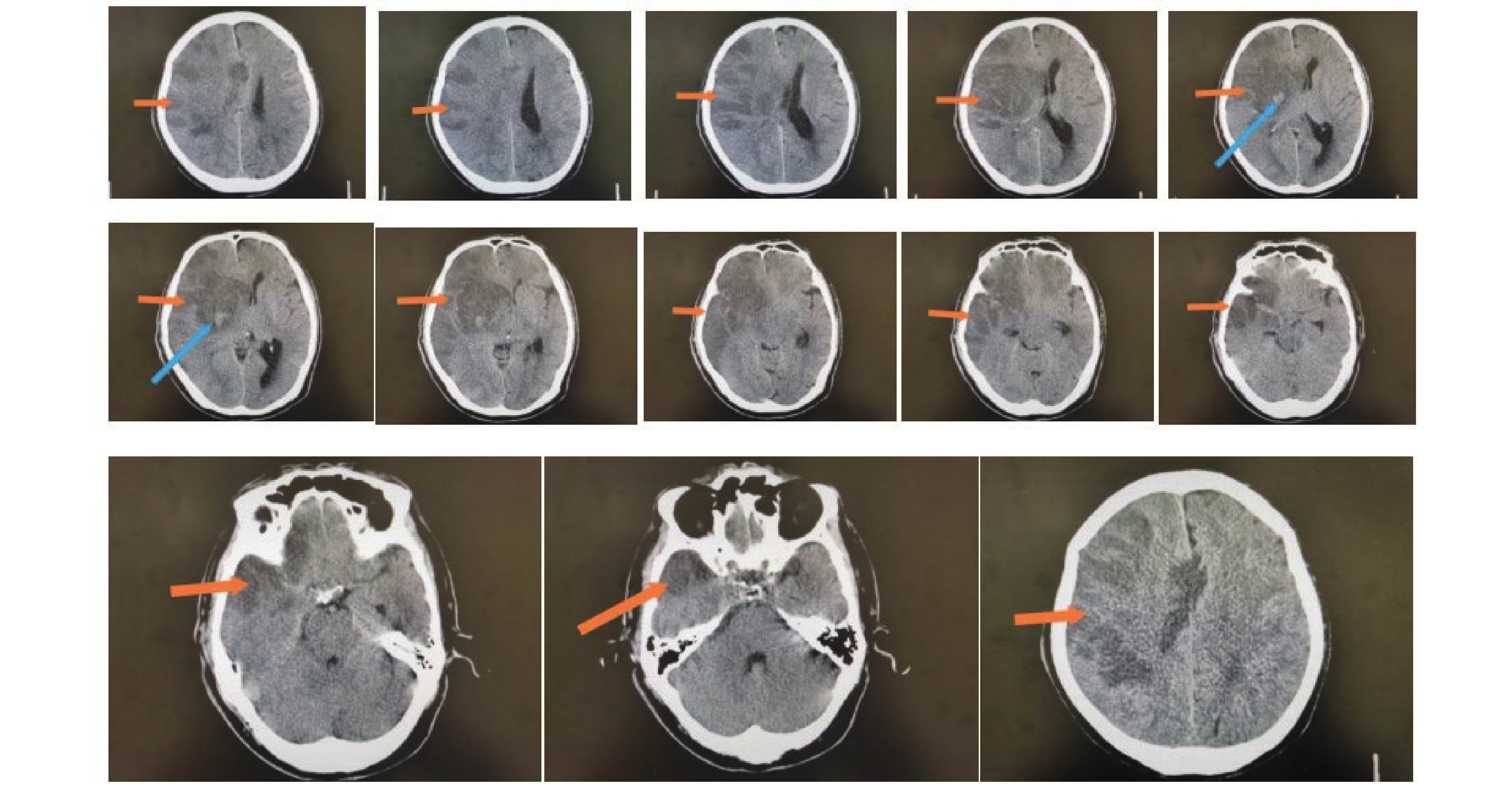
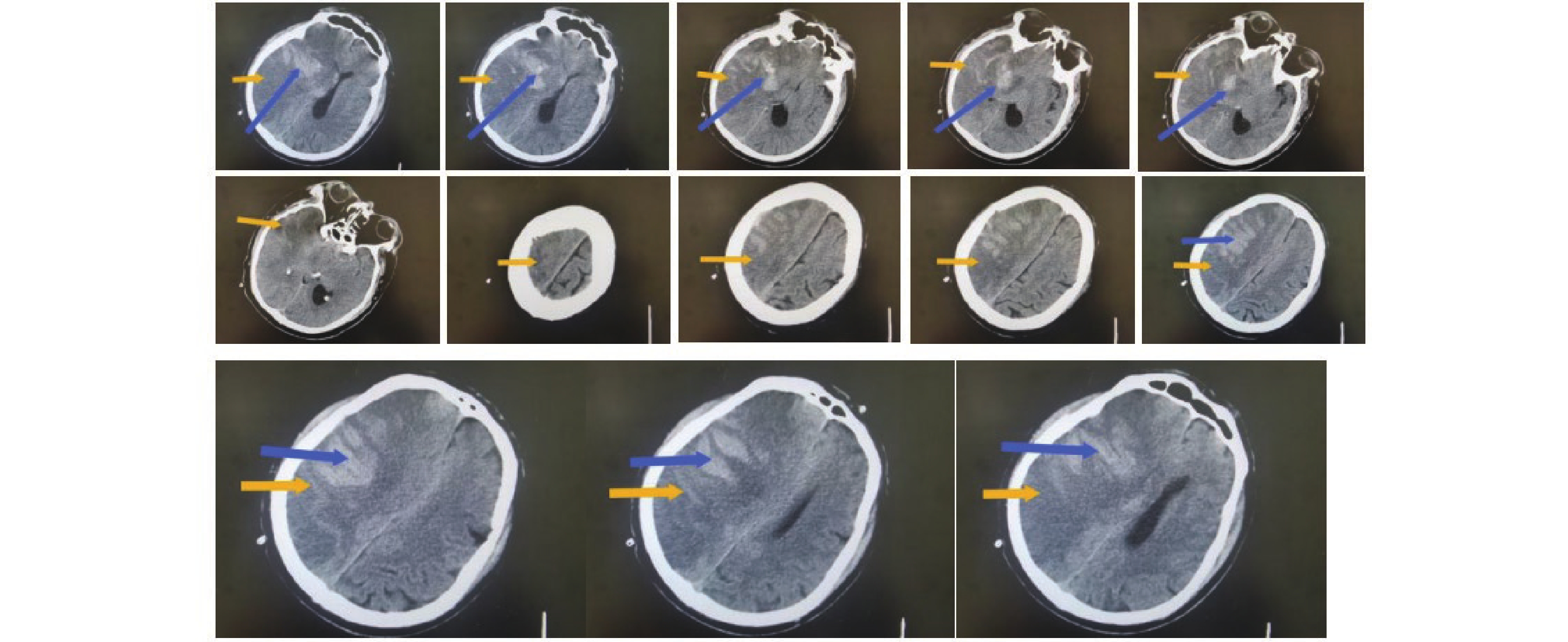
图 1 不良组术前头颅影像学表现
注:男性患者,67岁,从CT上看右侧额叶、颞叶、顶叶、岛叶大面积脑梗塞伴出血,中线左移,脑疝形成。其中橙色箭头指向低密度区为梗塞区,蓝色箭头指向较高密度区为出血。
Figure 1. Preoperative cranial imaging findings in the poor outcome group
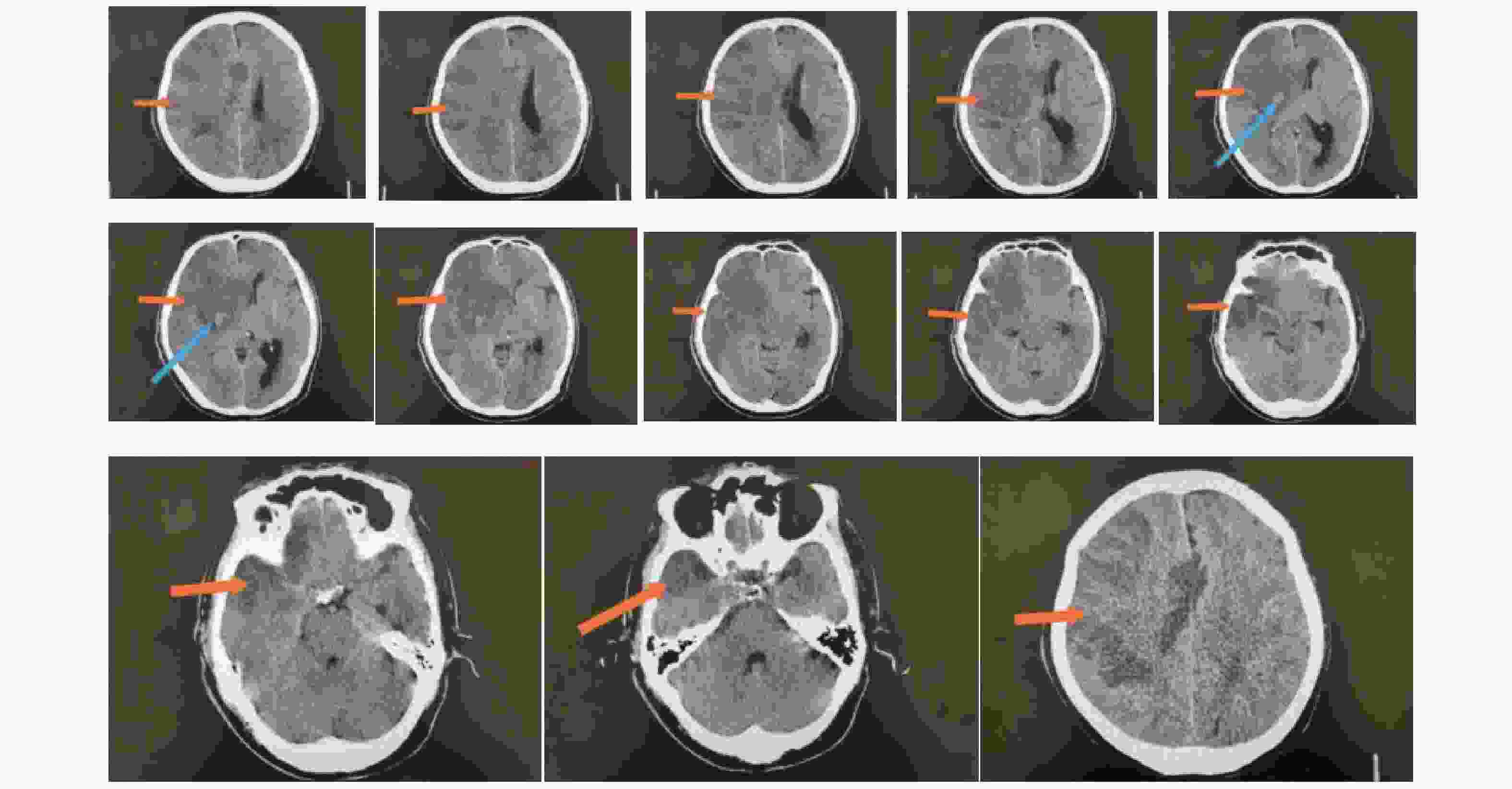
图 2 良好组术前头颅影像学表现
注:男性患者,75岁,从CT上看右侧额叶、颞叶、顶叶、岛叶大面积脑梗塞伴出血,中线左移。其中橙色箭头指向低密度区为梗塞区,蓝色箭头指向较高密度区为出血。
Figure 2. Preoperative cranial imaging findings in the good outcome group
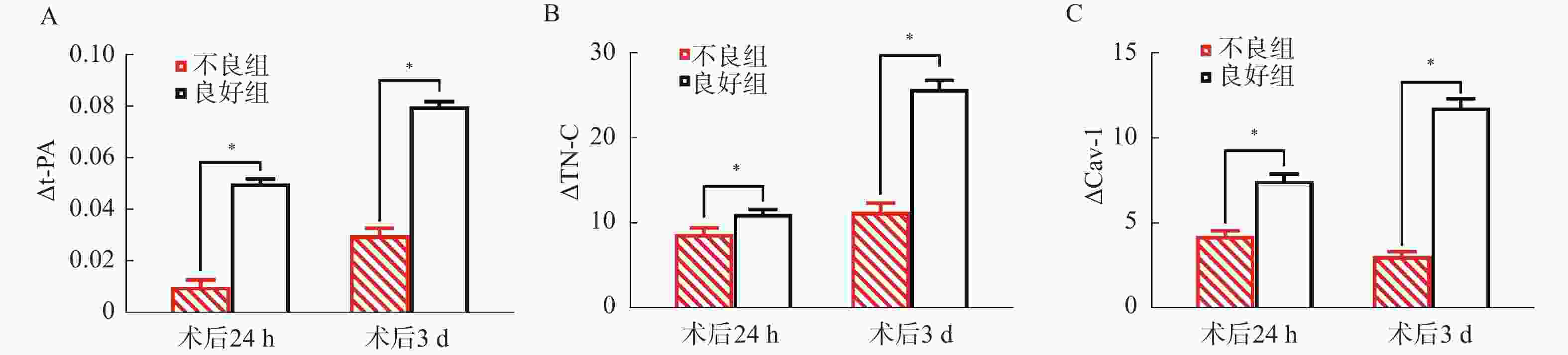
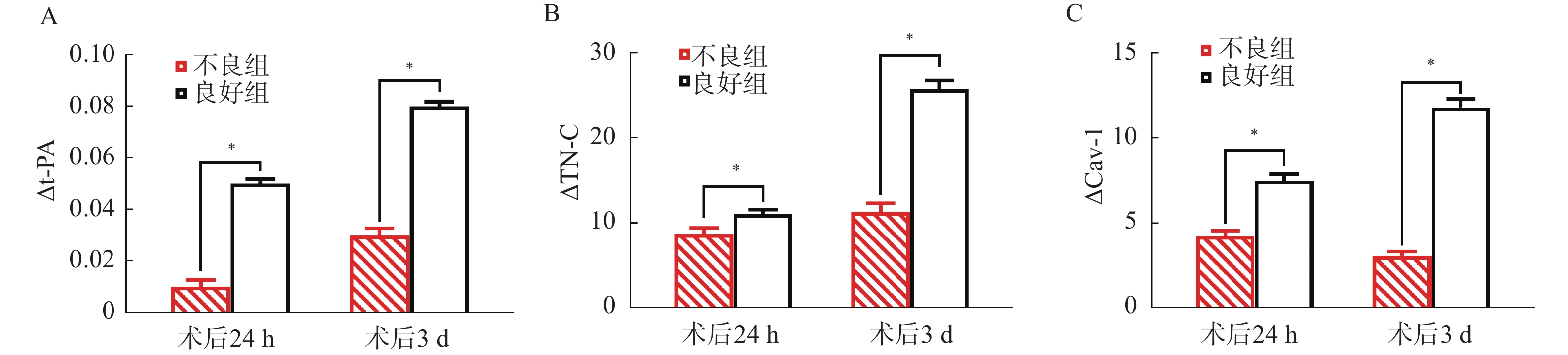
图 3 两组△t-PA、△TN-C、△Cav-1比较
A:△t-PA;B:△TN-C;C:△Cav-1;*P < 0.05。
Figure 3. Comparison of △t-PA,△TN-C and △Cav-1 between the two groups
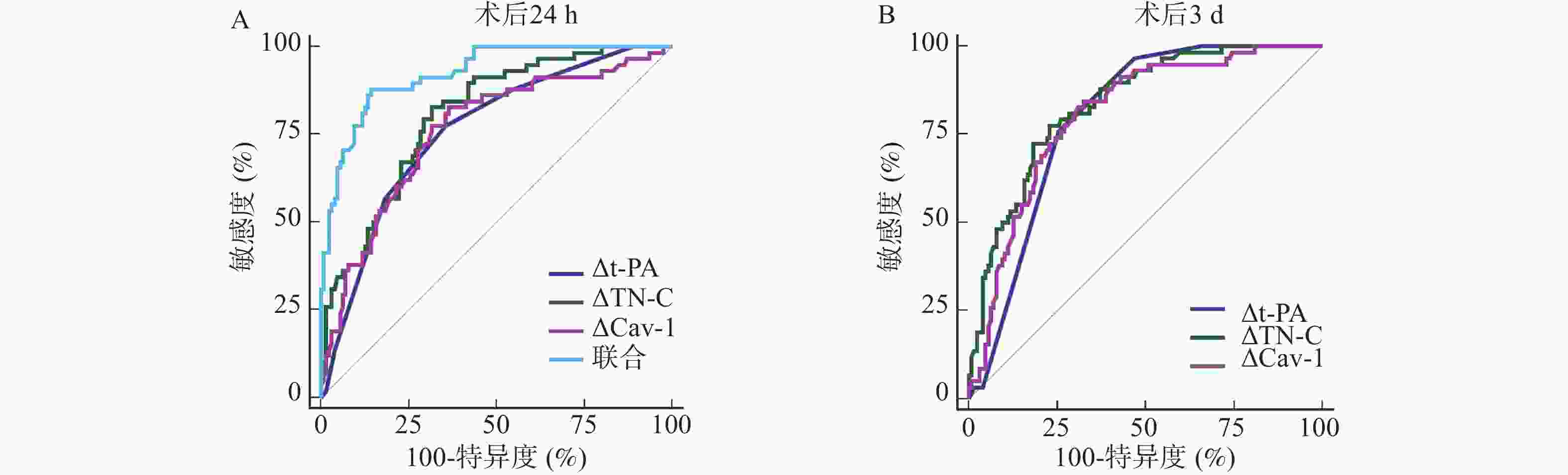
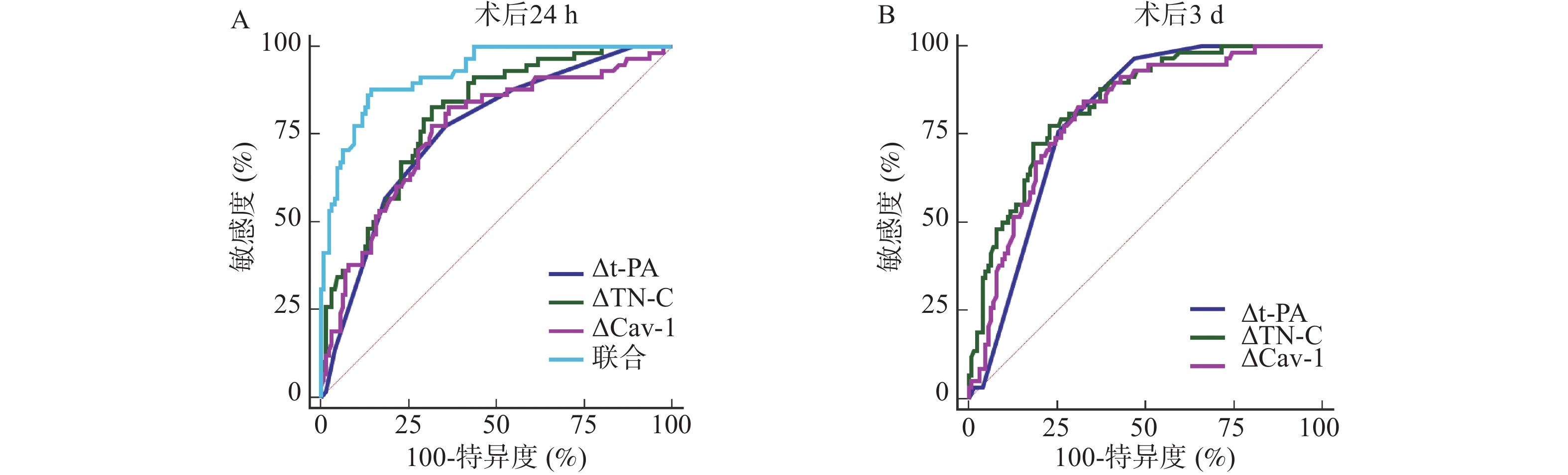
图 4 围术期t-PA、TN-C、Cav-1变化值预测术后不良病情转归的ROC
A:术后24 h t-PA、TN-C、Cav-1变化值预测术后不良病情转归的ROC;B:术后3 d t-PA、TN-C、Cav-1变化值预测术后不良病情转归的ROC。
Figure 4. ROC Curves for predicting postoperative adverse outcome using perioperative changes in t-PA,TN-C,and Cav-1
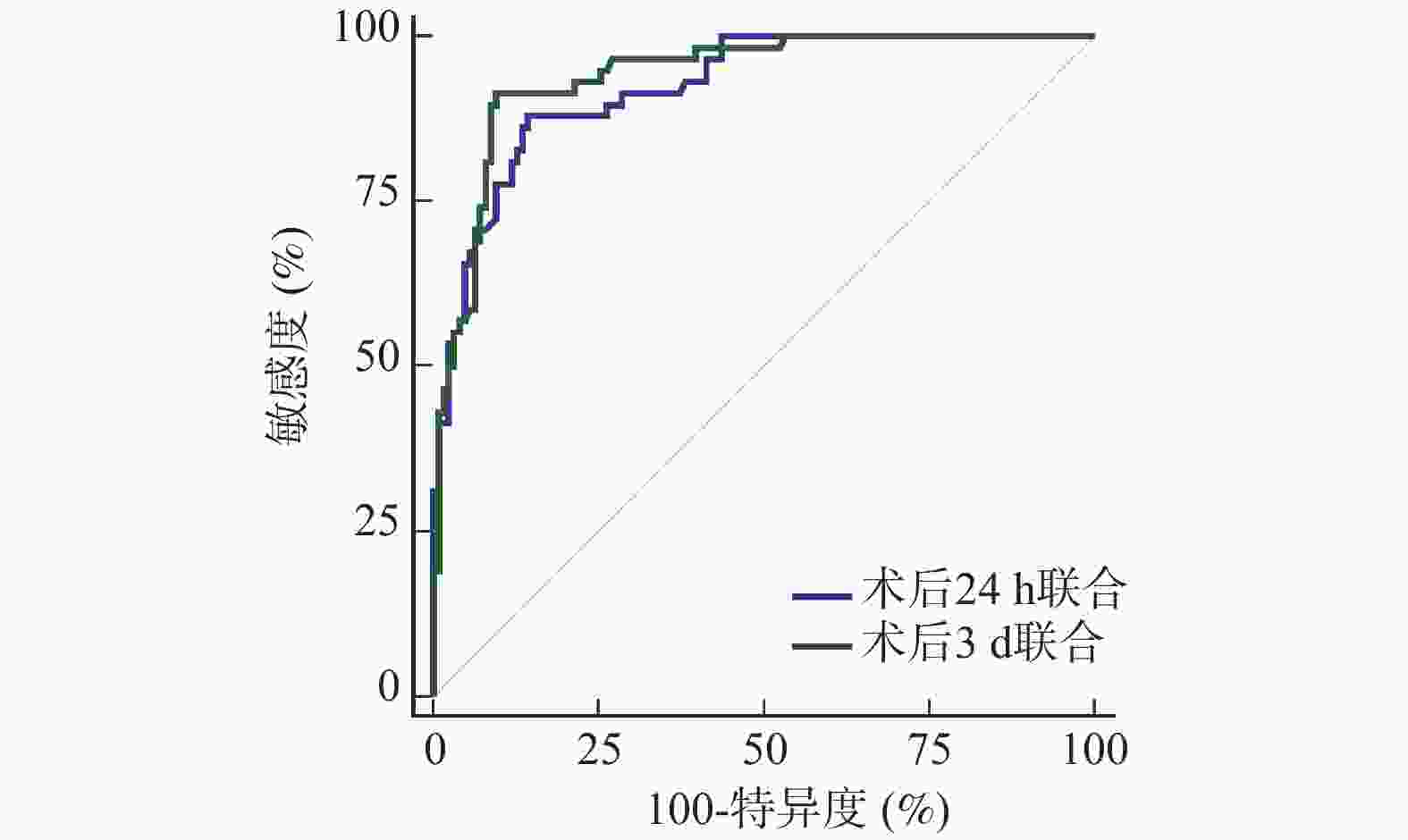
图 5 围术期t-PA、TN-C、Cav-1变化值联合预测术后不良病情转归的ROC
Figure 5. ROC curve for the combined prediction of postoperative adverse outcome using perioperative changes in t-PA,TN-C and Cav-1
表 1 围术期t-PA、TN-C、Cav-1变化计算公式
Table 1. Formula for calculating perioperative changes in t-PA,TN-C and Cav-1
指标 术后24 h变化值 术后3 d变化值 △t-PA 术后24 h t-PA—术前t-PA 术后3 d t-PA—术前t-PA △TN-C 术前TN-C—术后24 h TN-C 术前TN-C—术后3 d TN-C △Cav-1 术前Cav-1—术后24 h Cav-1 术前Cav-1—术后3 d Cav-1  下载: 导出CSV
下载: 导出CSV
表 2 两组基线资料比较[($ \bar x \pm s $)/n(%)]
Table 2. Comparison of baseline data between the two groups[ ($ \bar x \pm s $)/n(%)]
资料 不良组(n=58) 良好组(n=126) t P 年龄(岁) 56.15 ± 9.00 54.20 ± 7.38 1.551 0.123 性别 0.220 0.639 男 31(53.45) 72(57.14) 女 27(46.55) 54(42.86) 体质量 正常 19(32.76) 44(34.92) 0.082 0.774 超重 25(43.10) 57(45.24) 0.073 0.787 肥胖 14(24.14) 25(19.84) 0.439 0.508 糖尿病 28(48.28) 55(43.65) 0.343 0.558 高血压 17(29.31) 32(25.40) 0.311 0.577 冠心病 5(8.62) 7(5.56) 0.213 0.645 吸烟 22(37.93) 43(34.13) 0.113 0.737 饮酒 11(18.97) 19(15.08) 0.201 0.654 病灶位置 2.197 0.533 颞顶叶 37(63.79) 86(68.25) 额颞叶 8(13.79) 16(12.70) 额颞顶叶 7(12.07) 18(14.29) 顶枕叶 6(10.34) 6(4.76) 发病至手术时间(h) 27.30 ± 4.56 28.19 ± 5.00 1.153 0.251 术前GCS评分(分) 6.90 ± 1.22 7.86 ± 1.03 5.535 <0.001* 术前NIHSS评分(分) 14.78 ± 4.19 12.11 ± 3.78 4.300 <0.001* 梗死侧别 0.034 0.855 左侧 30(51.72) 67(53.17) 右侧 28(48.28) 59(46.83) 梗死体积(mL) 82.45 ± 15.62 78.92 ± 13.87 1.541 0.125 发病至手术时间(h) 27.30 ± 4.56 28.19 ± 5.00 1.153 0.251 术后脱水治疗强度 0.061 0.805 常规剂量 47(81.03) 104(82.54) 大剂量(甘露醇>375 mL/d) 11(18.97) 22(17.46) 抗血小板/抗凝治疗启动时间(h) 0.219 0.897 ≤48 39(67.24) 89(70.63) 49~72 15(25.86) 29(23.02) >72 4(6.90) 8(6.35) *P < 0.001。
下载: 导出CSV
表 3 两组围术期t-PA、TN-C、Cav-1比较($ \bar x \pm s $)
Table 3. Comparison of perioperative t-PA,TN-C and Cav-1 levels between the two groups ($ \bar x \pm s $)
指标 组别 n 术前 术后24 h 术后3 d t-PA(IU/mL) 不良组 58 0.11 ± 0.03 0.12 ± 0.02 0.14 ± 0.02 良好组 126 0.12 ± 0.04 0.17 ± 0.05 0.20 ± 0.04 F组间 − 12.405 18.632 24.817 F时间 − 9.763 15.328 20.541 F交互 − 18.245 12.976 16.382 P组间 − <0.001* <0.001* <0.001* P时间 − <0.001* <0.001* <0.001* P交互 − <0.001* <0.001* <0.001* TN-C(μg/L) 不良组 58 79.56 ± 18.34 70.84 ± 13.39 68.26 ± 11.94 良好组 126 75.80 ± 20.27 64.75 ± 16.28 50.03 ± 14.51 F组间 − 18.313 22.579 30.146 F时间 − 14.529 18.963 25.782 F交互 − 16.035 14.218 19.653 P组间 − <0.001* <0.001* <0.001* P时间 − <0.001* <0.001* <0.001* P交互 − <0.001* <0.001* <0.001* Cav-1(μg/L) 不良组 58 37.26 ± 9.85 33.00 ± 6.52 34.19 ± 8.46 良好组 126 35.94 ± 11.02 28.46 ± 8.39 24.13 ± 7.28 F组间 − 14.578 19.345 27.691 F时间 − 11.288 16.732 22.458 F交互 − 17.229 13.864 18.927 P组间 − <0.001* <0.001* <0.001* P时间 − <0.001* <0.001* <0.001* P交互 − <0.001* <0.001* <0.001* *P < 0.001。
下载: 导出CSV
表 4 围术期t-PA、TN-C、Cav-1变化值对病情转归的影响
Table 4. Effect of perioperative changes in t-PA,TN-C and Cav-1 on clinical outcome
影响因素 β SE Wald χ2 OR 95%CI P 下限 上限 术后24 h △t-PA −0.902 0.182 24.554 0.406 0.215 0.766 <0.001* △TN-C −1.200 0.306 15.378 0.301 0.148 0.613 <0.001* △Cav-1 −1.054 0.417 6.390 0.348 0.173 0.702 0.003* 常数项 3.681 0.082 31.527 − − − 术后3 d △t-PA −0.635 0.256 6.148 0.530 0.329 0.854 0.004* △TN-C −0.779 0.203 14.740 0.459 0.267 0.788 <0.001* △Cav-1 −0.711 0.241 8.714 0.491 0.264 0.913 <0.001 常数项 4.095 0.075 24.336 − − − <0.001* *P < 0.05。
下载: 导出CSV
表 5 围术期t-PA、TN-C、Cav-1变化值预测术后不良病情转归的效能
Table 5. Predictive Efficacy of perioperative changes in t-PA,TN-C and Cav-1 for postoperative adverse outcome
指标 AUC 95%CI cut-off值 敏感度(%) 特异度(%) P 术后24 h △t-PA 0.759 0.691~0.819 0.03 77.59 64.29 <0.001* △TN-C 0.804 0.739~0.859 10.31 82.76 68.25 <0.001* △Cav-1 0.760 0.691~0.819 5.90 82.76 63.49 <0.001* 术后3 d △t-PA 0.799 0.734~0.855 0.03 75.86 74.60 <0.001* △TN-C 0.836 0.774~0.886 13.79 77.59 76.98 <0.001* △Cav-1 0.807 0.742~0.861 4.27 84.48 67.46 <0.001* *P < 0.001。
下载: 导出CSV
-
[1] Hua X, Liu M, Wu S. Definition, prediction, prevention and management of patients with severe ischemic stroke and large infarction[J]. Chin Med J, 2023, 136(24): 2912-2922. doi: 10.1097/CM9.0000000000002885 [2] Michalski D, Jungk C, Beynon C, et al. Fokus Neurologische Intensivmedizin 2022/2023 “, ” Focus on neurological intensive care medicine 2022/2023: Zusammenfassung ausgewählter intensivmedizinischer Studien “, ” Summary of selected intensive medical care studies[J]. Anaesthesiologie, 2023, 72(12): 894-906. [3] Rochat T, Bögli S Y, Beqiri E, et al. Effect of decompressive craniectomy on intracranial pressure waveforms and vascular reactivity: A systematic scoping review[J]. Neurotrauma Rep, 2024, 5(1): 903-909. doi: 10.1089/neur.2024.0046 [4] Klijn C J, Dammers R, Sprigg N. Decompressive craniectomy for deep intracerebral haemorrhage: A SWITCH towards better outcomes?[J]. Lancet, 2024, 403(10442): 2351-2353. doi: 10.1016/S0140-6736(24)00703-7 [5] Chen R, Yan L, Xie P, et al. Use of diterpene ginkgolides meglumine injection to regulate plasma levels of PAI-1 and t-PA in patients with acute atherosclerotic cerebral infarction[J]. Neurologist, 2022, 27(6): 299-303. doi: 10.1097/NRL.0000000000000399 [6] Duan C, Xiong Y, Gu H, et al. Intravenous thrombolysis versus antiplatelet therapy in minor stroke patients with large vessel occlusion[J]. CNS Neurosci Ther, 2023, 29(6): 1615-1623. doi: 10.1111/cns.14124 [7] Chelluboina B, Chokkalla A K, Mehta S L, et al. Tenascin-C induction exacerbates post-stroke brain damage[J]. J Cereb Blood Flow Metab, 2022, 42(2): 253-263. doi: 10.1177/0271678X211056392 [8] Jin H Q, Jiang W F, Zheng X T, et al. miR-199a-5p enhances neuronal differentiation of neural stem cells and promotes neurogenesis by targeting Cav-1 after cerebral ischemia[J]. CNS Neurosci Ther, 2023, 29(12): 3967-3979. doi: 10.1111/cns.14323 [9] 中华医学会神经外科学分会, 国家卫健委脑卒中筛查与防治工程委员会, 海峡两岸医药卫生交流协会神经外科分会缺血性脑血管病学组. 大面积脑梗死外科治疗指南[J]. 中华医学杂志, 2021, 101(45): 3700-3711. doi: 10.3760/cma.j.cn112137-20210729-01687 [10] Seno S, Aoki M, Kiyozumi T, et al. Usefulness of the simple Coma scale, a simplified version of the Glasgow Coma scale[J]. Neurotrauma Rep, 2024, 5(1): 883-889. doi: 10.1089/neur.2024.0096 [11] Aguilar-Fuentes V, Orozco-Puga P, Jiménez-Ruiz A. The Glasgow Coma Scale: 50-year anniversary[J]. Neurol Sci, 2024, 45(6): 2899-2901. doi: 10.1007/s10072-024-07432-9 [12] Hendrix P, Melamed I, Collins M, et al. NIHSS 24 h after mechanical thrombectomy predicts 90-day functional outcome[J]. Clin Neuroradiol, 2022, 32(2): 401-406. doi: 10.1007/s00062-021-01068-4 [13] Wei Y, Zhang Q, Niu J, et al. Enlarged perivascular spaces predict malignant cerebral edema after acute large hemispheric infarction[J]. Cerebrovasc Dis Extra, 2024, 14(1): 30-38. doi: 10.1159/000536592 [14] Rochat T, Bögli S Y, Beqiri E, et al. Effect of decompressive craniectomy on intracranial pressure waveforms and vascular reactivity: A systematic scoping review[J]. Neurotrauma Rep, 2024, 5(1): 903-909. doi: 10.1089/neur.2024.0046 [15] Park A J, Garcia V P, Greiner J J, et al. Development of a hypercoagulable-hypofibrinolytic state early after spinal cord injury[J]. Arch Phys Med Rehabil, 2024, 105(5): 843-849. doi: 10.1016/j.apmr.2023.11.001 [16] Lin B, Shen Y, Zhang P, et al. Prognostic role of tissue plasminogen activator in coronary artery disease with or without aortic valve sclerosis[J]. ESC Heart Fail, 2023, 10(4): 2541-2549. doi: 10.1002/ehf2.14420 [17] 施罗炯, 孙静. 血栓-炎症因子水平与老年急性脑梗死患者静脉溶栓预后的关系探讨[J]. 中风与神经疾病杂志, 2023, 40(12): 1101-1107. doi: 10.19845/j.cnki.zfysjjbzz.2023.0237 [18] Hayward S J L, Chesnaye N C, Hole B, et al. Protein biomarkers and major cardiovascular events in older people with advanced CKD: The European quality (EQUAL) study[J]. Kidney Med, 2023, 6(1): 100745. [19] Patel R B, Dhanesha N, Sutariya B, et al. Targeting neutrophil α9 improves functional outcomes after stroke in mice with obesity-induced hyperglycemia[J]. Stroke, 2023, 54(9): 2409-2419. doi: 10.1161/STROKEAHA.123.042714 [20] Xie Y, Wu M, Li Y, et al. Low caveolin-1 levels and symptomatic intracranial haemorrhage risk in large-vessel occlusive stroke patients after endovascular thrombectomy[J]. Eur J Neurol, 2024, 31(8): e16342. doi: 10.1111/ene.16342 [21] Zhao Y, Zhu W, Wan T, et al. Vascular endothelium deploys caveolin-1 to regulate oligodendrogenesis after chronic cerebral ischemia in mice[J]. Nat Commun, 2022, 13(1): 6813. doi: 10.1038/s41467-022-34293-7 [22] Li Y, Liu B, Zhao T, et al. Comparative study of extracellular vesicles derived from mesenchymal stem cells and brain endothelial cells attenuating blood-brain barrier permeability via regulating Caveolin-1-dependent ZO-1 and Claudin-5 endocytosis in acute ischemic stroke[J]. J Nanobiotechnology, 2023, 21(1): 70. doi: 10.1186/s12951-023-01828-z [23] Gubern-Mérida C, Comajoan P, Huguet G, et al. Cav-1 protein levels in serum and infarcted brain correlate with hemorrhagic volume in a mouse model of thromboembolic stroke, independently of rt-PA administration[J]. Mol Neurobiol, 2022, 59(2): 1320-1332. doi: 10.1007/s12035-021-02644-y [24] Huang H, Zhang S, Du H, et al. Effect of Clopidogrel combined with aspirin in the treatment of acute progressive cerebral infarction: A retrospective single-center analysis[J]. Pak J Med Sci, 2024, 40(5): 891-895. doi: 10.12669/pjms.40.5.9206 [25] Wang Q, Cao H, Yan E, et al. The prognostic value of caveolin-1 levels in ischemic stroke patients after mechanical thrombectomy[J]. Neurol Sci, 2023, 44(6): 2081-2086. doi: 10.1007/s10072-023-06606-1 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 257
- HTML全文浏览量: 156
- PDF下载量: 60
- 被引次数: 0
